A prospective, multicentre, parallel-arm, randomized, controlled superiority trial was conducted between June 2021 and January 2023 across five high-volume tertiary referral centres for colorectal surgery. A power analysis was conducted to determine the number of patients enrolled in each study arm. The study protocol was approved by all local ethics committees in accordance with the Declaration of Helsinki and registered at ClinicalTrials.gov (ID number NCT03941938).
This study included consecutive patients diagnosed with histologically confirmed primary adenocarcinoma of the high-medium rectum without internal and/or external sphincter muscle involvement, with a distal margin of the tumour at least 8 cm from the anal verge, stage T2–T4 on magnetic resonance imaging (MRI) before neoadjuvant chemoradiation. Patients with squamous cell carcinoma, stage T1 or T4 adenocarcinoma with pelvic side wall involvement or requiring sacrectomy or prostatectomy (partial or total), unresectable primary rectal cancer or inability to complete R0 resection, rectal cancer less than 8 cm from the anal verge requiring coloanal or ultra-low rectal anastomosis, recurrent rectal cancer, previous pelvic malignancy, inability to return for postoperative follow-up, and inability to sign informed consent were excluded. Preoperative colonoscopy of the entire colon, computed tomography (CT) scan staging, and preoperative tumour and nodal staging using MRI and/or endorectal ultrasonography were performed for all participants. Surgery was performed within 8–12 weeks (56–84 days) after the completion of neoadjuvant therapy, when indicated. All patients were fully informed about the study, and informed consent for inclusion in the study was obtained. The participants were informed of their right to withdraw from the study or refuse initial enrolment at any point.
Randomization
Computer-generated randomization was used to create an allocation sequence to assign patients to different study arms. Randomization was centrally controlled by an operator who was not involved in the study. Patients were randomized only after the completion of neoadjuvant chemotherapy (when indicated) and before surgery. Patients randomized to the cyanoacrylate glue arm received anastomotic reinforcement with nebulised modified cyanoacrylate glue, whereas no anastomotic reinforcement was used in the control group. The modified cyanoacrylate used to reinforce the anastomosis is Glubran®2 (GEM S.r.l., Viareggio, Italy), a synthetic surgical biodegradable cyanoacrylate-based glue (NBCA + MS), modified by the addition of a monomer metacryloxysulfolane (MS) into n-butyl-cyanoacrylate (NBCA). As part of the educational intervention, all surgeons underwent training using a video demonstrating the surgical technique for the application of nebulised NBCA + MS.
Operative protocol
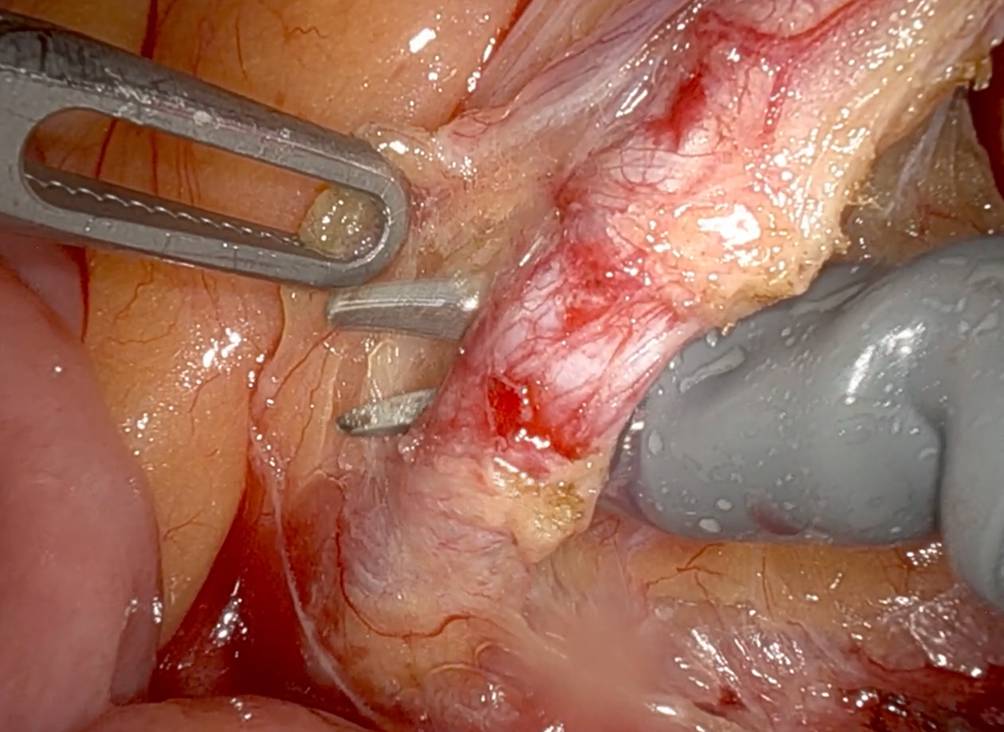
Patient preparation for surgery followed the general rules for Good Clinical Practice. Mechanical bowel preparation using an orally administered polyethylene glycol solution was performed in all patients, and antibiotic and antithrombotic prophylaxis were started immediately before surgery. The patients were placed in the lithotomy position for the abdominal and perineal procedures. Abdominal procedures (open or laparoscopic) were performed according to the oncological guidelines, including total mesorectal excision with adequate lymph node retrieval and at least 1 cm of distal clearance with an end-to-end or latero-terminal Knight–Griffen anastomosis. A pneumohydraulic test was performed to check for AL, and additional sutures were applied in positive tests. In patients randomized for the anastomotic reinforcement, the modified cyanoacrylate-based glue (NBCA + MS) was then nebulised all around the anastomosis for 2–3 s using the related special catheters for open or laparoscopic surgery.
Following the enhanced recovery after surgery protocol [27], the nasogastric tube was removed in the operating room after surgery completion, and the urinary catheter was removed within 72 h for rectal resection. Early mobilisation was strongly encouraged in all patients on the first postoperative day. Patients were allowed to drink clear liquids in the postoperative period once awake and were able to drink safely.
Postoperative management
Postoperative care was provided in accordance with the current standards directed by the operative surgeon. Narcotics or analgesics for pain were initially administered through the parenteral route (intramuscular, intravenous, or epidural), followed by oral administration when the patient resumed oral intake. Oral intake was allowed according to the patients’ tolerance. The patients returned to the ambulatory clinic for postoperative follow-up after 30 days. During follow-up, the postoperative data were recorded, and proctography was performed by transanal injection of 100 mL of hydro-soluble contrast medium (Gastrografin, sodium amidotrizoate and meglumine amidotrizoate, Bayer S.p.A.) to check the integrity of the anastomosis. AL was graded according to the classification system developed by Rahbari et al. Patients who did not attend the follow-up were contacted by a research nurse by phone or email, where available, to ascertain whether the patient had experienced any complications and/or adverse events treated in other hospitals. Patients unavailable for postoperative evaluation were considered lost to follow-up.
Outcomes measures
Demographic data (age, sex, weight, BMI (kg/m2), ASA classification, smoking status, and comorbidities) and intraoperative data (type of operative approach, operative time, type of anastomosis, and sutures) were recorded. Postoperative complications were classified in accordance with the Clavien–Dindo classification [28] and recorded along with the length of in-hospital postoperative days, 30-day readmission rate, and death. AL was defined as a defect in the intestinal wall integrity at the colorectal anastomotic site, leading to communication between the intra- and extraluminal compartments [29], with the presence of faecal discharge from the pelvic drainage at any time after surgery, rectovaginal fistula (defined as faecal or mucus discharge from the vagina), and pelvic sepsis (defined by the collection of pus/faecal material in the pelvis documented by a CT scan). ALs were classified according to the Rahbari et al. classification: grade A, AL requiring no active therapeutic intervention; grade B, AL requiring active therapeutic intervention but manageable without relaparotomy; and grade C, AL requiring re-laparotomy [29].
Statistical analysisSample size determination
The expected mean percentage of AL after rectal cancer is 16%, and a reduction to 10% was considered clinically significant. The sample size calculation determined that 67 patients per arm was sufficient to reject the null hypothesis with a power of 0.8 and a type I error probability of 0.05, with a confidence level of 95% (sample size calculated by R Studio Version 1.1.419, ©2009–2018 RStudio, Inc.). To account for a predicted 5% estimated loss to follow-up, the sample size was calculated as 138 (134 + 4).
Statistical methods
All statistical analyses were performed in an intention-to-treat manner. No interim analyses were planned. A P value of 0.05 indicated statistical significance. Student’s t test was used to provide an unadjusted estimate of the difference between treatment arms. Analysis of covariance, a more robust method that allows the control of key differences in baseline characteristics, was used to enable adjusted comparisons.
Similar to the primary outcome, continuous secondary outcomes (such as safety and efficacy) were modelled using t tests and analysis of covariance. The relationship between AL and other possible adverse factors was evaluated using univariate and multivariate regression analyses. When the complete case analysis excluded more than 5% of patients owing to missing data, exploratory analyses were performed to investigate the effect of missing data. To explore the mechanism of missing data and the validity of a complete case analysis for each endpoint, patient characteristics were compared between those with and without missing data, and multilevel logistic regression models were used to identify any associations between prognostic variables and determine if data were missing at random. The prognostic effect of each baseline parameter on AL outcomes (present/absent) was analysed using logistic regression. All parameters were analysed individually using logistic regression, and parameters with a probability level less than 0.1 were selected for analysis using stepwise multivariable regression. A polychotomous stepwise logistic regression model was used to correlate prognostic factors with Clavien–Dindo classification grades. Multilevel logistic regression was used to estimate the odds ratios (ORs) for conversion to laparotomy, intraoperative complications, and postoperative complications between the treatment groups.






留言 (0)