The present study aimed to evaluate LV diastolic function in patients with LV aneurysm using conventional and speckle-tracking echocardiographic parameters. As a first step, we investigated the association of echocardiographic parameters with invasive cardiac hemodynamic measures. We found that the longitudinal late diastolic strain rate at global and basal levels of the left ventricle correlated more strongly with mean PAP than conventional transmitral flow parameters and was able to detect a significantly increased mean PAP in our group of patients. It also has a significant correlation with mean PCWP and LVEDP. Lower GLSRa and BLSRa were associated with higher values for mean PAP, mean PCWP and LVEDP. Left atrial strain also demonstrated a correlation with mean PAP and PCWP.
Furthermore, we evaluated STE parameters in the outcome analysis and found that late diastolic strain rate at the global and basal level of the left ventricle, left atrial strain and ratio of early diastolic filling velocity to these parameters showed an association with event-free survival after adjustment for age and sex, as well as in a multivariate model including clinical and echocardiographic parameters. The best predictive value was demonstrated for the ratio of early diastolic filling velocity to GLSRa.
LV diastolic function by STE
Impaired LV diastolic function in patients with ischemic cardiomyopathy may be assessed using a similar integrative approach with the assessment of various echocardiographic indices, including STE parameters, such as strain rate during isovolumic relaxation and early diastolic strain rate alone or in conjunction with transmitral early diastolic filling velocity velocity [1]. Experimental studies have shown a strong association of these parameters with invasively measured LV filling [5, 22]. However, data on the assessment of diastolic function by LV diastolic strain rate in patients with ischemic cardiomyopathy are limited. In a study by Meluzin et al. [23], the late diastolic strain rate was significantly lower in patients with dilated cardiomyopathy than in controls, showed a significant correlation with PCWP and was able to detect elevated PCWP. In the same study, the early diastolic strain rate revealed no association with PCWP. Recently, PLAS has been proposed as a valuable parameter to assess LV diastolic dysfunction [1] and has been found to have predictive value in patients with heart failure with reduced ejection fraction [6].
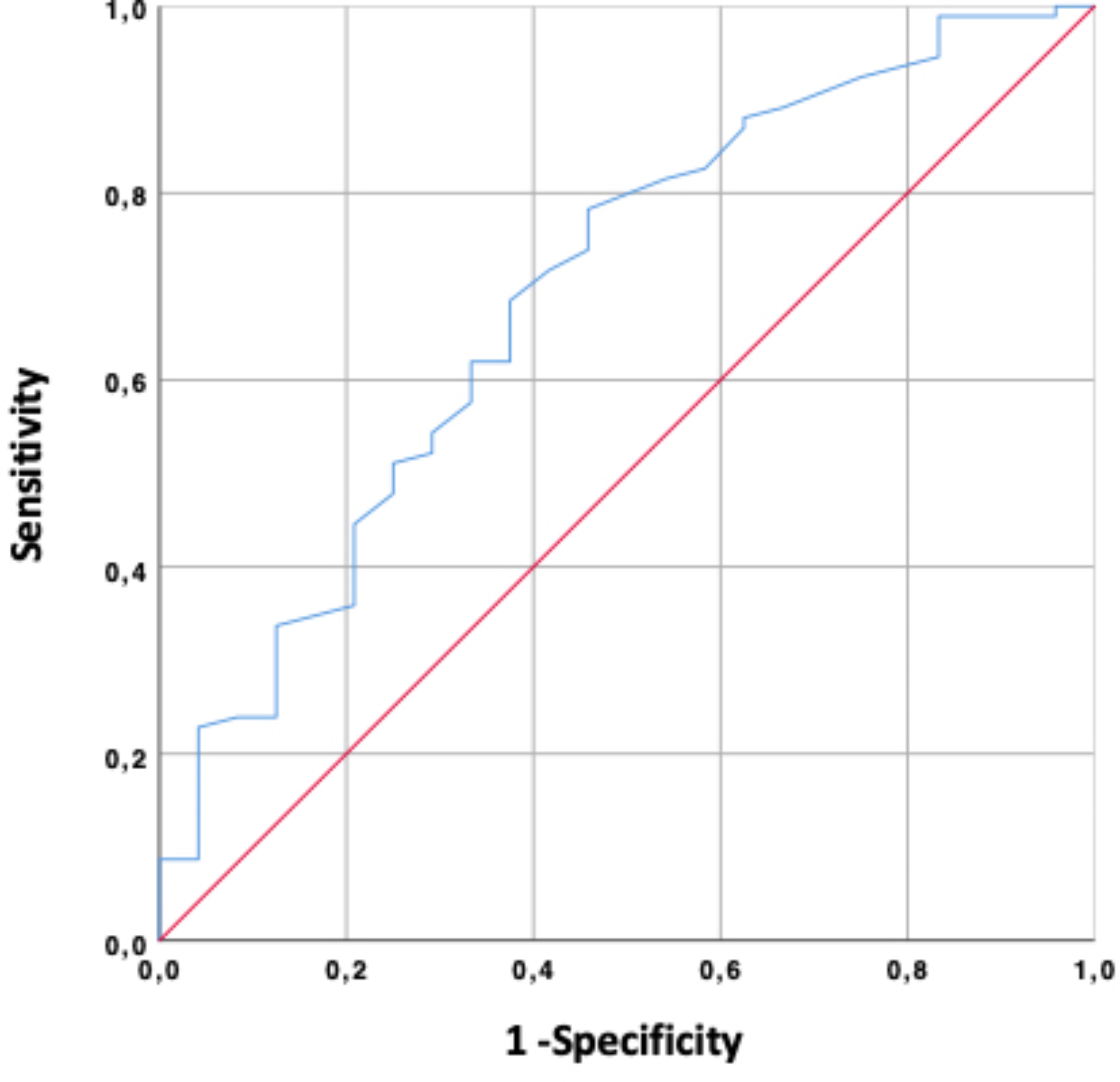
We demonstrated that STE parameters such as longitudinal late diastolic strain rate at global and basal levels of the left ventricle and left atrial strain were significantly correlated with mean PAP and mean PCWP. Furthermore, GLSRa and BLSRa showed a stronger correlation with the mean PAP than with the transmitral flow parameters. Among other STE parameters, only GLSRa and BLSRa correlated with LVEDP. GLSRa, BLSRa, PLAS and the ratio of early diastolic filling velocity to these parameters were able to detect severely elevated mean PAP (≥ 30 mmHg), with the predictive values expressed as the area under the curve (AUC) ranging from 0.81 to 0.89 and comparable to the AUC for transmitral flow velocities.
SRIVRT was not used in our study despite its proven role in the assessment of LV diastolic function [1, 5]. In our particular group of patients with severe LV remodeling, quantification of SRIVRT appeared to be poorly reproducible; therefore, we decided to focus on other STE diastolic parameters.
Prognostic role of LV diastolic function by echocardiography in patients with LV aneurysm
Previous studies have demonstrated that advanced diastolic dysfunction is associated with impaired survival after SVR [12, 22, 23]. A recent analysis of the STICH trial also confirmed that LV diastolic dysfunction assessed by the E/A ratio was a stronger predictor of survival than LV geometry assessed by the sphericity index [24]. In previous reports, diastolic dysfunction was evaluated using transmitral Doppler parameters [12, 23] or the more sensitive parameter E/e′ [22]. In one study, postoperative LV remodeling after SVR was evaluated using SRIVRT and demonstrated a good association with LV filling pressure [25]. Neither PLAS nor diastolic LV strain rate were previously evaluated for preoperative assessment of patients with LV aneurysm planned for SVR. In our previous study, we found that basal LV strain was associated with outcome and with improvement of regional LV function after SVR [26]. In the present study, STE parameters of diastolic dysfunction, such as PLAS and longitudinal late diastolic strain rate, were predictors of event-free survival and demonstrated incremental predictive value after adjustment for clinical and echocardiographic parameters. The highest predictive value was demonstrated for echocardiographic indices: ratio of early diastolic filling velocity to GLSRa and BLSRa. In other studies, it was also shown that the combination of early diastolic filling velocity with diastolic parameters of LV mechanics is useful for the assessment of LV diastolic pressure and plays a predictive role in various groups of patients [5].
In this study, the early diastolic strain rate was not associated with hemodynamic measures or with outcome. These data are consistent with the study of Meluzin et al. [23], where the early diastolic strain rate was also not associated with PCWP in patients with dilated cardiomyopathy. While early diastolic parameters mainly reflect active relaxation of the LV, parameters of late diastole are related to LV compliance [1]. This might be explained by significantly increased stiffness and decreased compliance of the left ventricle at this stage of heart failure.
Future perspectives
Recent advances in echocardiography allow automated quantification of LV myocardial mechanics using the speckle-tracking technique. This opens future opportunities for complex automated analysis of LV systolic and diastolic function, which could also be implemented in point-of-care ultrasound [27]. Our results demonstrate that the use of STE to assess LV diastolic function can play a prognostic role and might be useful in the preoperative evaluation of patients planned for SVR. STE quantification does not require a high level of expertise or additional image acquisition, and the analysis can be performed offline and has a low inter-observer variability, as demonstrated by our data and previous studies [28].
Assessment of additional diastolic parameters with STE may play important role in the integrative evaluation of LV diastolic function and become a part of a complex integrative approach, particularly in patients with ischemic cardiomyopathy. Its diagnostic and prognostic role should be further evaluated in different populations.
STE can be used for postsurgical assessment of LV diastolic function in patients with various pathologies. For this purpose, prospective studies are needed.
Limitations
It should be acknowledged that the current study has certain limitations. First, by its nature, it is subject to the restrictions of a nonrandomized single-center observational retrospective study. Only patients with feasible data were included; therefore, selection bias cannot be overcome. Women were underrepresented. Furthermore, there was a limited number of patients with tissue Doppler for quantification of early mitral annulus velocity. Thus, these data are not available for comparison. We included in the analysis those patients for whom the evaluation of diastolic function without e′ was possible based on other echocardiographic parameters.
Only a small number of patients underwent cardiac catheterization. Although there was no statistically significant difference in clinical and echocardiographic parameters between this group of patients and total cohort, there was a tendency for more deterioration in systolic and diastolic LV function and greater cardiac remodeling in patients who underwent catheterization. We believe that this group can be representative to demonstrate the association of STE parameters of diastolic function and heart hemodynamics and that the data can be generalized to a larger population of patients with post-ischemic LV aneurysm.
At the time of data collection, STE was already a standard technique in our institution, and 2-dimensional echocardiography was performed according to the highest level of expertise. All echocardiographic data were acquired using a single vendor ultrasound machine; thus, the cutoff values for STE parameters may be different for other vendors.







留言 (0)