
記住我


This section will address a detailed description of the Trauma-Informed Counselor Education and Supervision (TI-CES) framework that includes key assumptions, principles, and relevant recommendations in a sequence that were suggested by SAMHSA (2014a). In addition, we will outline the application of each assumption and principle to counselor education and training settings. We will also draw practical strategies that counseling programs and counselor educators can consider integrating into the training based on the existing literature as well as the application of key assumptions and principles.
Four Assumptions of Trauma-Informed Counselor EducationThe four assumptions are characterized as 4 Rs, including (1) Realize the widespread impact of trauma, (2) Recognize the signs and symptoms of trauma, (3) Respond by fully integrating knowledge about trauma into policies and procedures, and (4) Resist retraumatization. The first assumption is to “realize” the traumatic events and their impacts on CITs’ health and functioning. This assumption emphasizes the importance of having a basic knowledge base about trauma, such as wide-ranging concepts, definitions, or types of trauma as well as lifelong impacts of trauma, specific to CITs. Everybody in the program who is involved in the training process, including counselor educators, clinic coordinators, clinical staff, administrative staff, and CITs, should understand that trauma can affect CITs’ training experience, behavior, mental health, impairment, educational functioning and outcome, and even their career path after graduation. For instance, CITs with a trauma history of physical violence and abuse being locked in a room may struggle to conduct counseling sessions in a closed counseling facility because they were personally violated in a typically secure setting. Counselor educators can help CITs realize the lifelong impacts of trauma in general so that they can be better prepared for training components with potential for (re) traumatization.
Next, everyone in the program as well as the organization or system may seek to “recognize” the signs of trauma. Recognizing can be understood as trauma sensitivity and awareness of trauma. Albeit there is an understanding that trauma symptoms are pervasive, not many individuals, including CITs and staff in the counseling program, may have sensitivity to recognize trauma symptoms for many reasons. Also, individual characteristics of CITs, such as race/ethnicity, disability, and gender, can affect the prevalence and types of trauma symptoms, and the symptoms can be gender, race, age, or setting-specific (SAMHSA, 2014b). For example, CITs who identify as racially minoritized can endorse negative race-based experiences as stressful and traumatic. Counselor educators can help CITs recognize their exposure to past or ongoing traumatic events and recognize how unique sets of trauma symptoms are manifested across individuals.
The third assumption of fully integrating trauma knowledge into policies and procedures requires that everyone and training systems at both individual and organizational levels “respond” by helping CITs touched by trauma achieve successful educational outcomes while minimizing potential harm during counselor education and training and promoting a high-quality life as future professional counselors. Responding by applying trauma-informed approaches includes modifying course or graduation policies program-wide; providing education and training for CITs, staff, and faculty; and promoting communication that involves universal precautions approach where the existence of trauma is naturally acknowledged, not stigmatized.
In addition, the fourth TIC assumption of “resisting retraumatization” encourages everyone and a training program to minimize risks of retraumatization among all people in the program and provide care to those who are retraumatized in a timely manner. People in a counseling program should be prepared to be able to mitigate the impacts of any form of retraumatization in order to prevent counselor impairment and ultimately promote client welfare. For example, CITs are required to take different courses in that the nature of the course content is sensitive, such as crisis, violence, maltreatment, and trauma. Also, CITs need to complete the practicum and internship, where they might encounter clients with a trauma history, which could trigger painful memories of past traumatic experiences for the trainee.
Six Principles of Trauma-Informed Counselor EducationIn addition, the six key principles include (1) Safety; (2) Trustworthiness and transparency; (3) Peer support; (4) Collaboration and mutuality; (5) Empowerment, voice, and choice; and (6) Cultural, historical, and gender issues.
Consistent with SAMHSA’s key principles (2014b), the TI-CES framework outlines six key principles that empower CITs and help them promote the linkage to recovery and resilience. Safety is essential to provide optimal training environments that respect CITs’ experiences and potential for learning and functioning. CITs’ feelings of physical, emotional, and psychological safety should be prioritized in the whole training process, and all stakeholders including counselor educators need to adjust the program and organization both at an individual and structural level. According to SAMHSA’s TIC framework (2014a), understanding safety in counselor training programs should be defined by CITs. Counselor educators, thus, need to continuously and regularly seek feedback from CITs about their experiences in various contexts of training. Understanding their subjective perception of safety will provide the basis for counselor educators to create safe environments by incorporating diverse pedagogical and theoretical approaches into the trauma-informed framework. In this way, counselor educators and staff can also ensure that safety is a high priority in multiple contexts of training, such as classroom environments, supervision, practicum, and internship by providing a space where CITs can share their concerns willingly and openly.
Trustworthiness and transparency are another key principle that the program-wide efforts should implement. All individuals, including faculty members, clinic staff, and administrative staff, should be well-informed about policies, procedures, and practices that may impact the way they relate to CITs. Program-wide operations and decisions are conducted with transparency in pursuit of the goal of building and maintaining trust between multiple relationships, such as faculty-student relationships and staff-student relationships. Lack of trustworthiness and transparency may damage those relationships, which might eventually diminish the competencies and wellness of CITs. For this reason, it is especially important that counselor educators develop a sense of trustworthiness and transparency with trainees.
To provide trauma-informed training, Peer support is a key venue to promote recovery, healing, hope, and a sense of relatedness. Per SAMHSA (2014a, p. 11), peer support can refer to “individuals with lived experiences of trauma” or “trauma survivors.” In this regard, peer support can include help and support from not only peers who are CITs but also staff, supervisors, instructors, and faculty advisors who have experienced similar trauma or the same identity marker that can serve as underlying risks for traumatization. In counseling programs, on the other hand, CITs who face similar training-related risks for (re)traumatization can also provide mutual support to one another as “peers.”
Collaboration and mutuality refer to sharing of power and decision-making in an effort to implement TIC. This principle helps individuals at all levels of the program to recognize that everyone has a role to play in integrating key assumptions and principles into the training and education. The mutuality of TI-CES can enable all individuals in the program, including CITs, to take greater responsibility for addressing barriers to implementing shared plans effectively. For example, reverse mentoring (i.e., a reciprocal relationship between a less experienced mentor providing specific knowledge and a more experienced mentee) can be effective in education (Zauchner-Studnicka, 2017). CITs feel more empowered as active participants in the creation and implementation of policies and procedures, which can be beneficial to their recovery and competency-building as a professional.
All individuals’ strengths and experiences are recognized as valuable resources to accomplish the principle of Empowerment, voice, and Choice. It is crucial to encourage CITs to utilize their strengths, skills, and preferences, rather than focusing on deficits. Additionally, collaborative decision-making on program-wide planning on CITs’ wellness and coping will help build a sense of control and empowerment. Informing CITs of all available options for their learning and professional development that are safe and efficacious can also promote their sense of empowerment. It would also be worth recognizing not only risk factors for retraumatization, such as past traumas or individual susceptibility, but also CITs’ internal and external resources as key protective factors against the risk of retraumatization. By creating those opportunities to increase empowerment, they will be able to become active agents for change and recovery from traumatization.
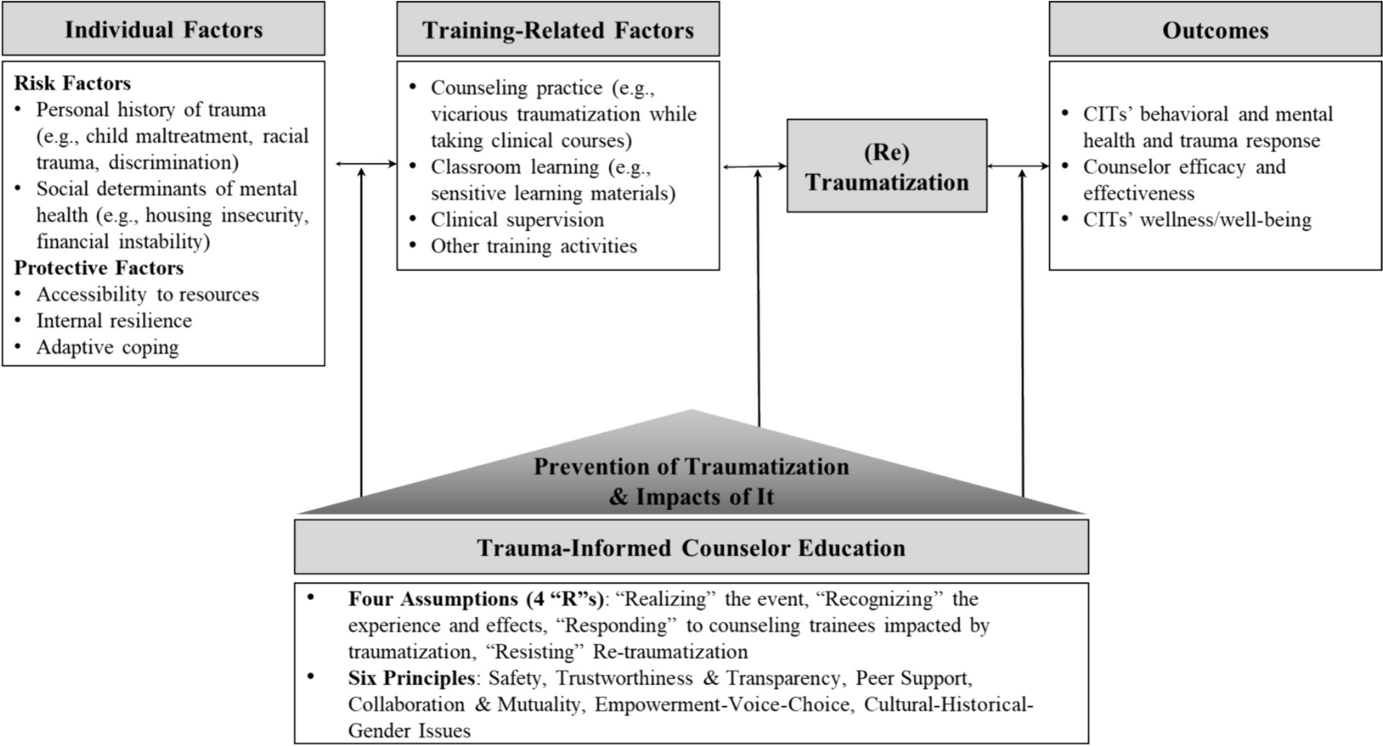
Last but not least, individuals at all levels should actively take Cultural, historical, and gender issues into consideration when building and implementing policies and procedures. All the policies, procedures, and protocols should be responsive to the cultural needs of individuals in the program. This principle can be accomplished by increasing awareness and sensitivity to culture-based trauma, such as cultural, historical, collective, or intergenerational traumas among individuals from marginalized social groups. Lack of awareness and responsiveness to those specific forms of traumas can increase the potential for retraumatization. It is essential to recognize and address cultural, historical, and gender issues in building trauma-informed counselor education and supervision. Figure 1 depicts a conceptual framework of the TI-CES, illustrating both related factors (e.g., predictors and outcomes) to CITs’ (re) traumatization, and the way TI-CES can help intervene to prevent (re) traumatization and minimize the impacts of it when (re) traumatization occurs inevitably.
Fig. 1
Trauma-Informed Counselor Education and Supervision (TI-CES) framework
Key Recommendations for TI-CESTI-CES emphasizes step-by-step prevention and intervention efforts that can be considered for implementation at multiple levels (e.g., individual, interpersonal, organizational, and institutional levels) to minimize the risks of (re) traumatization while promoting healing from human suffering (see Table 1). In the framework, Step 1 strategies should be considered beginning with the interview process through the onboarding of incoming students. Step 1 recommendations prioritize efforts to help create and strengthen a psychologically safe culture in the counseling program where CITs’ underlying risks for (re) traumatization could be voluntarily screened or assessed. The underlying risks may include CITs’ trauma history and intersecting identities and social determinants. The psychologically safe programmatic culture may facilitate program-wide screening for a history of trauma or traumatic experiences for incoming trainees. Specifically, counselor educator advisors may administer a brief screening for a personal trauma history or social identity markers that might have intersected with their stressful life experiences. Results of the screening either through program-wide procedures or individual advising sessions can inform counselor educators of the students’ underlying risks for (re) traumatization.
Table 1 A summary of key recommendations for Trauma-Informed Counselor Education and SupervisionStep 2 recommendations are primarily focused on prevention efforts throughout the training process. A key concept addressed in Step 2 is preventing (re) traumatization across multiple contexts of training, such as classroom learning, fieldwork (e.g., practicum and internship), and supervision. Specific recommendations for this step may include the following: integrating wellness activities into classroom learning; creating a structured and predictable learning environment that fosters a sense of safety; minimizing potential triggers for trainees’ painful memories; implementing assessment to increase self-awareness about the impact of their trauma experience; expanding trauma education into the curriculum (Chatters & Liu, 2020); helping CITs build a realistic self-care plan and regularly employ check-ins; and incorporating content in counselor burnout, vicarious traumatization, compassion fatigue, and trauma-informed practices (Sommer, 2008).
Given that a realistic aim of TI-CES is not to eliminate all possible risks of (re) traumatization but to minimize the risks, strategies for the post (re) traumatization are essential. Step 3 recommendations are concerned with postvention efforts to address “what already has occurred” during training. Topics addressed in this step include minimizing the adverse impact of (re) traumatization and promoting healing from (re) traumatization. Examples of practical recommendations may include the following: implementing a culturally responsive trauma-informed approach that recognizes context and intergenerational vulnerabilities, allowing mental health or wellness day that CITs can take a moment to process their emotional difficulties triggered by (re) traumatization, providing a safe space for CITs to process and talk about their experiences during training across different modalities (e.g., individual supervision and group healing session), and providing direct emotional coaching and support.
Throughout the entire process of TI-CES, all principles and assumptions from the TIC framework can be primary guidance for any type of effort suggested previously. For example, CITs’ sense of agency and safety should be prioritized in the screening process in Step 1. Also, screening protocols should be sensitive to respondents' potential retraumatization, and enough time should be spent to prepare and explain the screening process. CITs may choose to delay or not respond to the screening at all.
In summary, the primary intent to apply TI-CES should not only be focused on initiating specific activity or policy but also on constructing a safe and mutually respectful culture in which everyone’s individual experiences can be properly recognized, accommodated, and respected. In other words, The TI-CES framework should be about collective efforts to provide a safe culture in counselor education and training. Table 1 summarizes the specific, step-by-step recommendations for counselor educators and counseling programs to consider.
留言 (0)