
記住我





This study has a randomized controlled cross-over design and is approved by the ethics committee of the Department of Psychology and Sports Sciences of the Goethe University (2022-55, approved 30/08/2022). The trial was registered a priori (German Register for Clinical Trials, DRKS-ID: DRKS00030085, date of first trial registration 25/08/2022) and conducted in accordance with the ethical standards set down by the declaration of Helsinki with its recent modification of 2013 (Fortaleza) [22].
ParticipantsParticipants were recruited between August and October 2022 in a university in Germany. Eligibility criteria included being between 18 and 50 years of age with no (medical or psychosocial) contraindication against vigorous physical activity. Due to the experimental design, authors had direct contact to the participants and thus could identify individual participants during data collection. During analysis data was anonymized. Exclusion criteria were cardiovascular-, pulmonary-, or advanced degenerative musculoskeletal diseases, pregnancy and not completely healed musculoskeletal injury (that affect subjective quality of life or physical performance during walking and stair climbing).
Sample size calculations were performed based on an earlier study comparing CO2 kinetics during steady state exercise with a FFP2 and a surgical mask against a no mask control [23]. A calculation based on an effect size of Cohen’s d = 0.39 (Partial η2 0.136) a significance level of 5% and an 80% power resulted in a sample size of at least eleven participants adopting a crossover design with four measurements in repeated measures analysis of variance (rmANOVA). Calculating with a drop-out rate of 20%, a minimum of 13 participants needed to be included in this study.
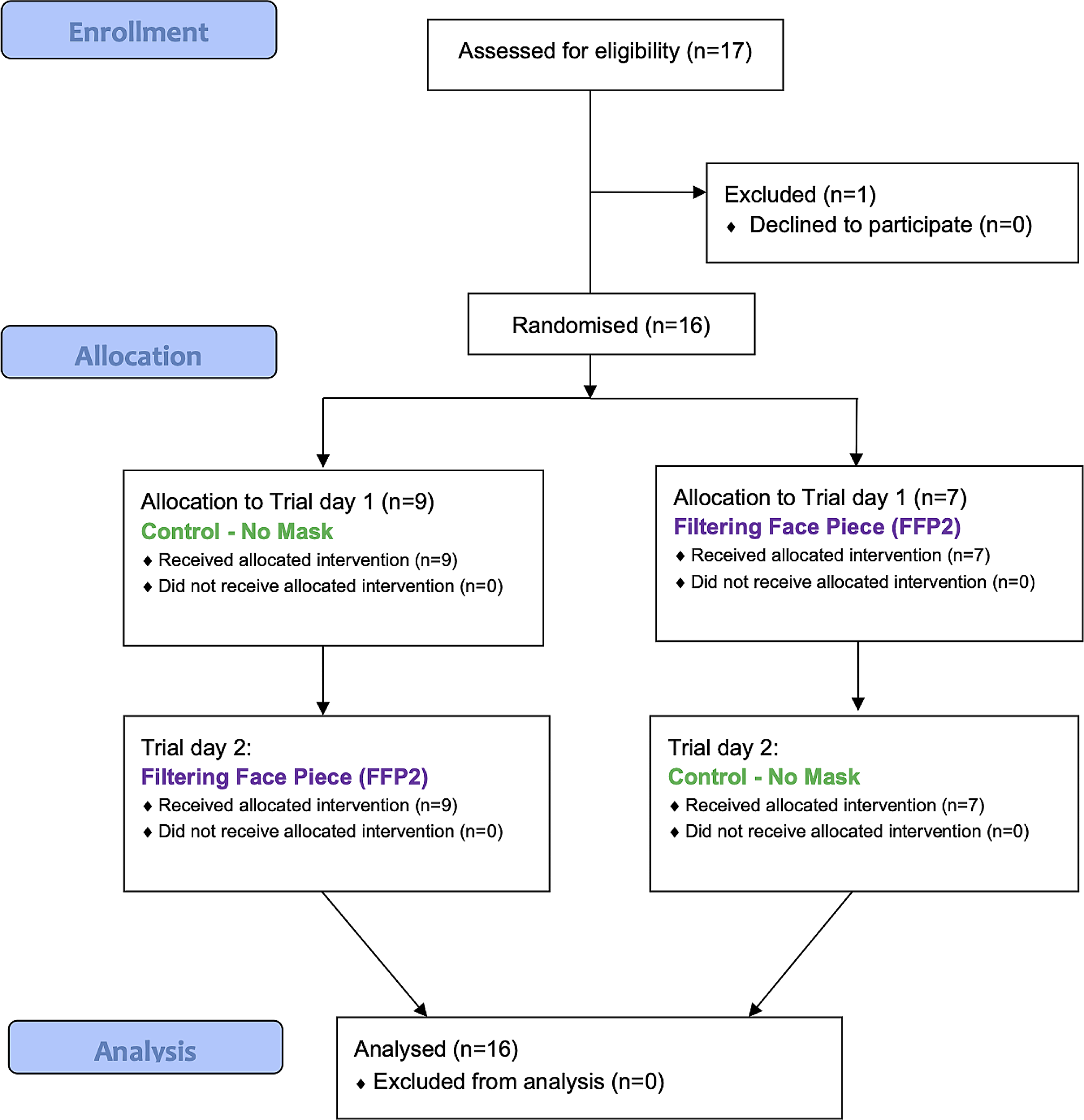
Before study participation, participants were informed on voluntary participation and signed a written informed consent. Eligibility, exclusion and randomization scheme of the protocol is shown in the flow diagram in Fig. 1.
Fig. 1
CONSORT flow diagram of the protocol procedures
Figure description: Sixteen participants were assigned to either the FFP2 mask (n = 7) or the unmasked condition (n = 9) by randomisation, followed by crossover to the other condition. CONSORT 2010, Consolidated Standards of Reporting
InterventionsAll participants performed two interventions types (walking and stair climbing), each once with and once without a fold-flat type FFP2 (IMSTec GmbH, Klein-Winternheim, Germany) on two different trial days separated by a minimum of 48 h. The manipulation (FFP2 or no mask) order was randomized (simple balanced randomization using www.randomizer.org).
Each trial day consisted of a six-minute walking phase, followed by an eight-minute stair climbing phase with ten minutes resting time without wearing a mask in-between. Order allocation was done blinded. The participants were blinded to the respective manipulation until the beginning of each intervention.
Each session was performed at a comparable time of the day (± 2 h) and at days with comparable routines (i.e. working days). Participants had to avoid vigorous physical activities in the 48 h preceding each test and had to maintain their habitual diet behaviour during the timeframe of all three interventions. Furthermore, participants were requested not to take any food or drinks (except for water) in the period of two hours prior to each examination.
At each session, participants first rested for five minutes in a seated position without wearing a FFP2. Baseline data for spiroergometric outcomes, blood gas analysis and subjective response were assessed during this time slot. After that the six minutes ground level walking phase was rolled out in a hallway. The walking speed was standardized and Participants walked 612 m (1,7 m per second). Between the walking and stair climbing intervention, a resting period of ten minutes was held during which the participants were not manipulated (did not wear a mask). Afterwards, the eight minutes stair climbing was performed in on in a two-story staircase. Again, the speed was standardized and all participants completed 24 floors upstairs and downstairs on a standard stairway (stair height 16.5 centimeters, 69.3 m of elevation).
OutcomesDuring baseline testing at each trial day and during the interventions, spiroergometric data and heart rate were measured continuously. Participants self-reported perception was asked every two minutes using standardized scales. The capillary drawings for blood gas analysis were done at the end of baseline testing and immediately after both interventions at the ear lobe with participants in a seated position.
Baseline examination including standard anthropometrical values, educational status (school and study years), habitual physical activity and sedentary behaviour (International Physical Activity Questionnaire IPAQ) [24, 25] took place before the first intervention. Furthermore, participants underwent a step incremental exercise test (7–8 km/h at the start depending on individual fitness; 7° inclination; 0,5 km/h increment every 30 s) on a treadmill until volitional exhaustion to assess maximal oxygen uptake (VO2max), maximal heart rate and maximal respiratory exchange ratio. For spiroergometric measures during VO2max, baseline and intervention testing a valid and reliable portable analyser was applied (K5, Cosmed, Werneck, Germany) [26].
Baseline data for spiroergometric outcomes, blood gas analysis and subjective response were assessed after five minutes of sitting without a FFP2 at the start of both trial days. Spiroergometric measures during baseline and interventions included ventilation (in litres per minute, l/min), breathing frequency (breaths per minute), tidal volume (in litres, l), oxygen uptake (VO2 in millilitres per minute, ml/min), carbon dioxide exhalation (VCO2 in millilitres per minute, ml/min), respiratory exchange ratio, end tidal carbon dioxide (PetCO2 in millimetres of mercury, mmHg) and end tidal oxygen pressure (PetO2 in millimetres of mercury, mmHg). For blood gas analysis, capillary blood (100 µl) was drawn from an earlobe of the participant and analysed using a validated on-site device (epoc® Blood Analysis System, Epocal Inc., Ottawa, Ontario, Canada) [27]. Outcomes included pH, carbon dioxide partial pressure (pCO2 in millimetres mercury, mmHg), oxygen partial pressure (pO2 in mm/Hg), lactate (mmol per litre, mmol/l) and base excess (BE in mmHg). Subjective response included perceived exertion, based on a 15-point Borg Scale ranging from “very very light” (lowest rating 6) to “very very hard” (highest rating 20) [28], and dyspnoea based on a modified Borg Scale with the same range [29]. Participants were furthermore asked to rate their perception of pain based on a numeric rating scale ranging from “no pain” (lowest rating 0) to “most severe pain imaginable (highest rating 10) [30].
Data analysis and statisticsWe applied Microsoft Excel (Version 16.68) for data processing, Jamovi (Version 2.3.19) for data analysis, and Prism (Version 9) for data presentation. Data were checked for outliers, the distribution was analyzed using box and whisker plots and tested for normal distribution using Shapiro-wilk tests. Descriptive data were reported as means and standard deviations (baseline values and post intervention values) or 95% confidence intervals for all data points available. If datasets were incomplete, missing data was indicated using the number of included datasets in all tables.
Repeated measures analyses of variance (rmANOVA) were applied to analyse the effect of the manipulation (FFP2 versus no mask) on all outcomes and differences between baseline values of both trial days. In a second step, the impact of potential confounders including sex, age, weight, Body-Mass-Index (BMI), physical activity and maximal oxygen uptake capacity was assessed using analysis of covariance (ANCOVA). Pearson correlation was applied to detect associations between subjective measures and spiroergometric or blood gas analysis data which were affected by FFP2 application. We applied Bonferroni corrections for multiple comparisons. Due to 34 between-manipulations-comparisons p ≤ 0.001 is considered statistically significant.
留言 (0)