
記住我






The monkeypox (Mpox) virus belongs to the Orthopoxvirus family and is known to be one of the largest DNA viruses. The virus is a double-stranded, linear DNA virus that is protected by a viral envelope [1]. The Orthopoxvirus family is unique among virus families due to its large size and its ability to replicate in the cytoplasm of cells, given the presence of a DNA-dependent RNA polymerase [2]. There are four major elements of the virion: the core, lateral bodies, outer membrane, and the outer lipoprotein envelope [3]. The mpox virus, due to its double stranded DNA structure and DNA polymerase activity, was expected to have a low frequency of mutation and was considered to be a slowly evolving virus [4, 5]. In the 2022 viral outbreak however, the virus was found to be deviated from the viruses synthesized in 2018 and 2019 by approximately 50 single nucleotide polymorphisms, which is a significantly higher than expected rate of substitution; in addition, various subclusters of the virus have been identified with some “super spreader events” associated with mpox swift viral transmission, which may imply higher rates of transmission than expected [5]. The World Health Organization (WHO) declared the virus a Public Health Emergency of International concern in 2022. Cases were reported internationally including throughout Europe and North America; a total of 117 countries were ultimately reported by the WHO as having mpox population incidences, with a total of 93,000 patients infected and 176 deaths reported. The United States had the highest number of confirmed cases since the beginning of the outbreak, with approximately 31,000 diagnosed positive mpox patients. Remarkably, as of January 1st 2022, the top ten countries with newly diagnosed cases all fell outside of the African continent, accounting for 81.5% of reported cases. These countries included the United States of America, Brazil, Spain, France, Colombia, Mexico, the United Kingdom, Peru, Germany, and China [6].
There are two established pathways for the transmission of mpox virus: animal to human and human to human. Animal to human transmission occurs in endemic nations and can be seen in invasive forms of contact such as scratches and bites from infected animals as well as from non-invasive contact including close contact with animals or cleaning animal cages [7]. Reynold and colleagues categorize transmission as both “non-invasive” (i.e. touch or close contact with animals or their cages) and “complex” (i.e. bites or scratches) and report complex exposures may result in more significant systemic symptoms [7]. Human to human contact occurs via a multitude of pathways that include but are not limited to: sexual intercourse, vertical transmission via mother to child in utero, inhalation of respiratory droplets, and fomites [8, 9]. Regardless of transmission method, the virus replicates at the site of inoculation, usually the respiratory and oropharyngeal mucosa and travels to sentinel lymph nodes. This is the primary viremia. The secondary viremia stage involves spread via the lymphatic system to distant lymph nodes. The incubation process lasts between 7 to 21 days [10]. The patient is not contagious during this incubation period as they are also asymptomatic. In the subsequent prodromal stage, the secondary viremia produces gastrointestinal, respiratory, and dermatologic symptoms at which time the patient becomes the most contagious. During this prodromal stage, the classic clinical symptoms of mpox arise [11].
Current epidemiological analysis suggests that 96% of all newly diagnosed patients are male. Men who have sex with men (MSM) are those greatest at risk of transmission of the virus [6].
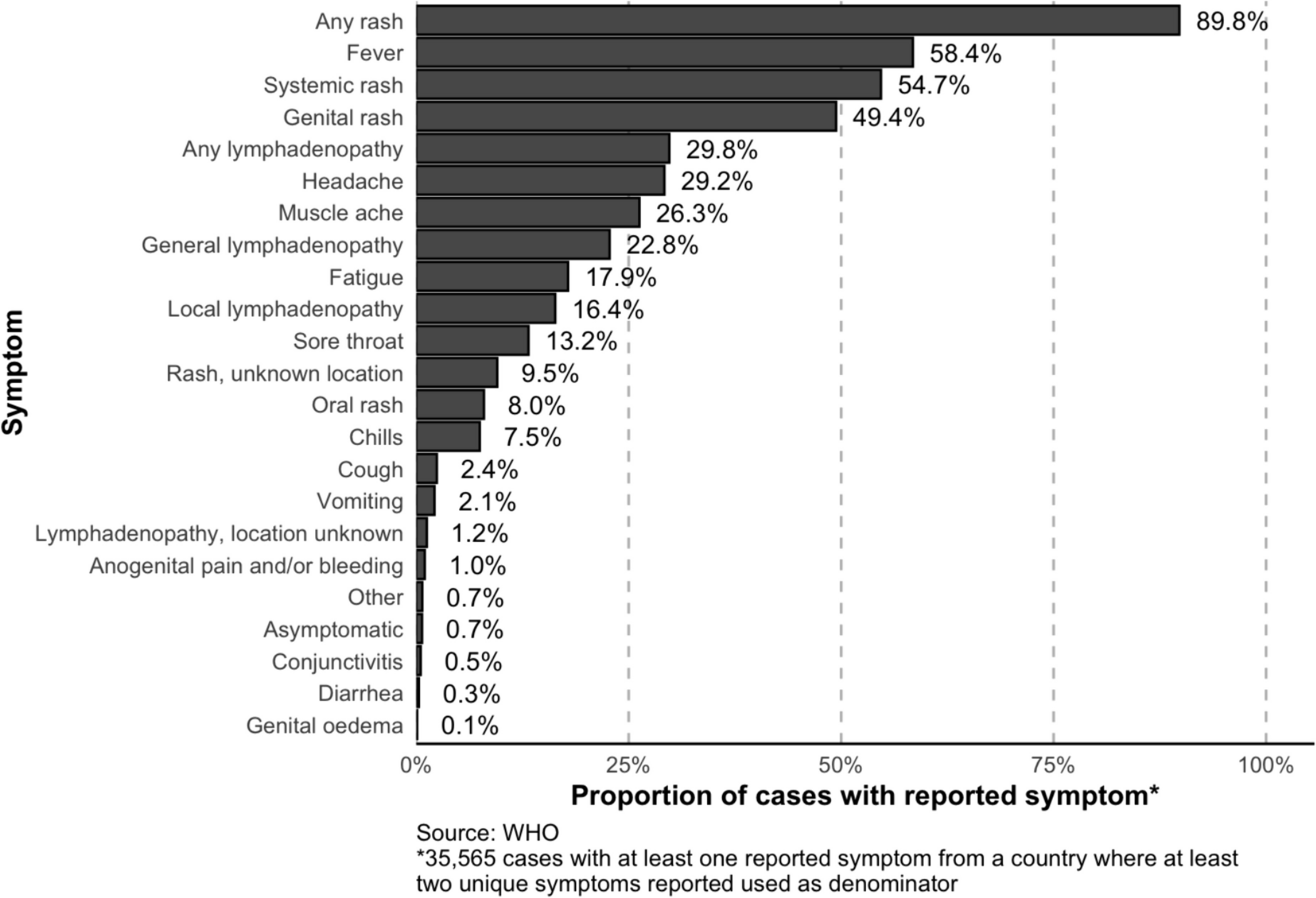
The symptoms experienced from the mpox virus vary widely amongst the patient population. According to the WHO, the most commonly reported symptoms include fever and rash. Remarkably, a rash is reported in nearly 90% of patients with at least one symptom. In the prodromal stage, non-specific symptoms including local or generalized lymphadenopathy. A supplementary figure published by the WHO reflects the incidence of various symptoms associated with mpox (Fig. 1) [6]. These include systemic or oral or genital rash, any or local lymphadenopathy, headache, myalgia, sore throat, chills, coughing, emesis, anorectal pain or bleeding, and diarrhea. A cutaneous manifestation of mpox on the forehead is presented in Fig. 2A. Less frequently, GI manifestations of the virus include nausea, vomiting, diarrhea, abdominal pain, rectal pain, rectal bleeding, rectal perforation, rectal abscess, dyschezia, proctitis, and tenesmus, among others [12]. Simadibrata and colleagues compiled a systemic review of gastrointestinal symptoms associated with mpox and note that anorexia was the most common, followed by emesis, nausea, abdominal pain and diarrhea [12]. In reality, these GI symptoms are also commonly associated with appendicitis, gastroenteritis, and diverticulitis alongside a variety of common gastrointestinal pathologies.
Fig. 1
World Health Organization (WHO) figure highlighting mpox symptoms by type and frequency
Fig. 2
Cutaneous and anorectal manifestations of mpox
Prior to the 2022 outbreak, most histopathological and immunohistochemical analyses of the mpox virus evaluated the cutaneous manifestations of the disease process. Notable features of these cutaneous manifestations included epidermal necrosis, multinucleated giant keratocytes, B-type inclusions (Guarnieri bodies) and perivascular cell infiltrates [13]. With an increase in the prevalence of proctitis in mpox, the role of endoscopic biopsies has become critical, with histopathologic findings of edematous, erythematous, friable mucosa with small erosive lesions [14, 15]. In the case series by Mazzotta et al., the group evaluated rectal biopsies performed in patients with mpox and found a consistent theme of lymphoplasmacytic infiltration with mild crypt distortion, reactive follicular hyperplasia and lymphoid aggregates observed in all specimens [16]. Of interest, there were no intracytoplasmic eosinophilic inclusion bodies, typically identified in skin lesions, that were observed in patients with GI manifestations of mpox who underwent endoscopic evaluation specimens [16].
Treatment is guided by severity of the illness and underlying patient comorbidities. In mild cases, patients are treated with supportive therapy that includes hydration, analgesia, stool softeners, and topical lidocaine, depending on the patient’s symptomology [17]. Pain control can contribute up to one third of cases that require inpatient admission [18]. Pain recommendations by the Centers for Disease Control (CDC) include the use of non-steroidal anti-inflammatory medications (NSAIDs), acetaminophen and at times opioids and gabapentin [17]. Patients also require counseling on the incidence of bacterial infection and anticipatory guidance for symptoms including increased pain, swelling, purulent drainage, or erythema, which can suggest abscess formation [17]. We have also presented the case of a patient who presented with anal abscesses requiring procedural management with an incision and drainage at our institution [19].
With respect to proctitis, rectal pain, perianal abscess, and rectal perforation have been reported with mpox manifestation [20]. Fig. 2B reflects the anorectal manifestation of mpox with viral perianal abscess and lesions. Treatment considerations include the use of stool softeners, topical lidocaine, over the counter medications including NSAIDs and acetaminophen, and sitz baths. Patients with genital lesions can consider the use of topical steroids to assist with swelling; patients with severe oropharyngeal lesions may require a mouth wash with antiseptic or local anesthetic; and oral antihistamines or calamine lotion may alleviate the discomfort of itching associated with some mpox lesions [17].
For more severe cases in the United States, there are currently no established protocols for treatment of mpox. Considerations for treatment include severe disease or involvement of sensitive anatomic areas with physiologic consequences of disease sequela. Severe disease, as defined by the CDC, includes symptoms that reflect hemorrhagic disease including confluent or necrotic lesions, involvement of multi-organ systems, severe lymphadenopathy compromising respiratory status, a status that requires inpatient admission or severe cardiac, pulmonary, ophthalmologic or neurologic involvement [21]. Patients requiring special consideration also include pediatric patients, obstetric patients (pregnant or postpartum), immunocompromised patients, or patients with prior dermatologic conditions that have compromised the skin barrier. There are currently a variety of studies and therapeutics under review, which will be briefly summarized as below. There are several exemptions for off-label use of medications such as Tecovirimat and immune globulin (IVIG) by the FDA. Tecovirimat is an antiviral medication that compromises cellular viral transmission and is currently the drug of choice for patients suffering with severe symptoms, patients who are immunocompromised, and those with eye infections [22]. Tecovirimat has an ongoing clinical trial (STOMP), a randomized, placebo controlled double blind study to establish efficacy for treatment of people with laboratory confirmed or presumptive mpox. The trial is currently a Phase 3 trial with an estimated required enrollment of 530 participants and an expected completion date in 2025. Study participants receive a course of medication for 14 days and monitor symptoms for 29 days or until resolution with weekly follow up. The primary outcome of the study is the time to resolution of symptoms described as the first day on which all skin lesions are scabbed, desquamated or healed and visible mucosal lesions are healed. Secondary outcomes include assessment of pain control and level of mpox in skin lesions, genital secretions and rectum [23]. A similar trial is also ongoing in the United Kingdom (PLATINUM), assessing the efficacy of treatment with Tecovirimat [24]. The mechanism of action of Tecovirimat is via the inhibition of VP37 envelope protein, which is responsible for viral formation, maturation, and release [10]. Other medical options include brincidofovir, a prodrug of cidofovir, that has been used for human smallpox disease in adults and children; it appears in animal models to be effective against mpox. Emergency use approval has been granted for patients with severe disease and who are unable to proceed with tecovirimat therapy. In addition, cidofovir is FDA-approved for the treatment of cytomegalovirus in patients with acquired immunodeficiency syndrome; again in animal models cidofovir has been shown as effective against the orthopox virus families. While cidofivir has been proven effective in treatment it is not without risk as it is known to have dose related nephro-toxic effects due to accumulation in the proximal renal tubules.proximal renal tubules [37]. Finally, the vaccinia immune globulin intravenous is also under review as an investigational drug that can rarely be used for prophylaxis in patients with a severe immunocompromised status [21]. In addition, there is an active enrollment for the VIRISMAP study that assesses virologic and immunologic characteristics of severe mpox in people with advanced HIV disease [25]. JYNNEOS is a live attenuated vaccine given as two doses 4 weeks apart either into the subcutaneous or intradermal layer of the skin. It is recommended by CDC for high risk individuals such as sex workers, having a partner with a diagnosis of mpox and individuals with occupational exposure to orthopoxviruses (i.e.laboratory workers.) [38].
留言 (0)