Respiratory infections are one of the major infectious threats faced by the global child population [28, 29]. In developing countries, acute respiratory infections are the leading cause of death among children [30, 31]. Influenza virus and Mycoplasma pneumoniae infections have caused multiple pandemics worldwide [32], with each pandemic potentially presenting different symptoms, signs, and laboratory test results. When the influenza virus and Mycoplasma pneumoniae co-infect and cause a pandemic, there are often situations of uncertainty.
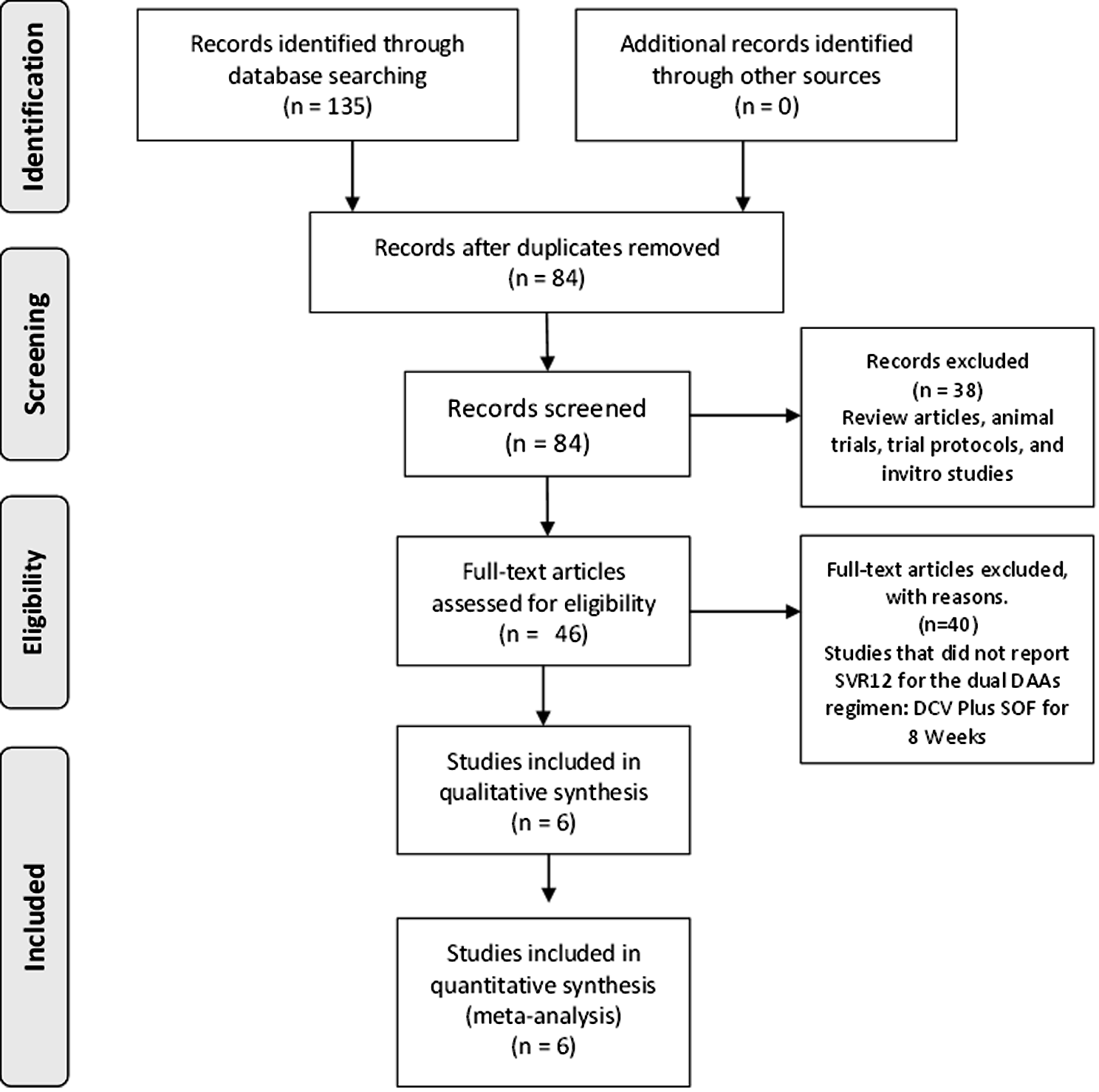
In this retrospective study, based on medical records, we investigated children aged ≤ 12 years with Mycoplasma pneumoniae or influenza virus infection. RT-PCR detection revealed 214 cases of Mycoplasma pneumoniae infection, 180 cases of influenza A, and 29 cases of influenza B. Due to the small number of influenza B cases, the influenza A and influenza B cases were combined for statistical analysis. Therefore, the data were divided into two groups: 214 cases in the MP group and 209 cases in the IV group. By comparing the routine peripheral blood parameters of the two, we explored the differences between the two infections to better understand their characteristics and clinical manifestations. This study helps doctors diagnose and treat pediatric respiratory infections more accurately and provides a basis for formulating prevention and control strategies.
Our study first compared the clinical features of pediatric influenza patients and Mycoplasma pneumoniae patients. The results showed that the most common symptoms in influenza patients included fever, runny nose, sore throat, and headache, while Mycoplasma pneumoniae patients mainly presented with cough, sputum, and wheezing. This finding is consistent with the research results of Wang M [33]. In addition, we found that there was no significant difference in sex distribution among the patient population, whether it was influenza or Mycoplasma pneumoniae, which is consistent with the research results of Zhang J [34].
We then analyzed the peripheral blood parameters of influenza and Mycoplasma pneumoniae patients and identified parameters with significant differences and AUC ≥ 0.7, including Lym#, Eos#, Bas#, Mon%, Eos%, PLT, PCT, HFC#, PLT-I, and PLR. Although our analysis identified several indicators with relatively high AUC, a single indicator as a standard for disease diagnosis has not yet achieved the expected results. In our expectations, using artificial intelligence models based on big data to perform multifactorial joint diagnostic differentiation between Mycoplasma pneumoniae infection and influenza infection can further enhance the efficacy of diagnostic discrimination, making it more effective and practical in clinical applications. There are many interference factors, and the highest AUC is only 0.824. To further explore the role of multiparametric joint diagnostic differentiation between Mycoplasma pneumoniae infection and influenza infection, we applied ten effective parameters with AUC ≥ 0.7 to various artificial intelligence models. Ultimately, we found that the combined diagnosis using multiple parameters significantly enhanced the AUC. We then selected the top five models, which showed consistent and superior performance in both training and test sets, namely RF, LDA, SVM, GB, and MP, for the Delong test analysis. These five models have shown effective predictive performance in distinguishing between Mycoplasma pneumoniae and influenza patients (AUC > 0.89). However, since the RF model had the highest AUC in the training set and its difference was statistically significant (p < 0.01) compared to the other four models, we finally chose the RF model as the prediction algorithm (AUC > 0.99). The random forest model is one type of machine-learning algorithm and is widely used in the biomedical field [35, 36]. Through the refinement process of the random forest model, we identified a subset of six key indicators, including Lym#, Eos#, Mon%, PLT, HFC#, and PLR.
Lymphocytes (Lym) are widely considered to be an important indicator of viral infection [37]. After influenza virus infection, lymphocytes usually decrease, which is consistent with our research results. Compared with Mycoplasma pneumoniae patients, influenza patients usually have a decrease in Lym# [2.155(1.595–2.833) vs. 1.050(0.770–1.670), p < 0.0001].
Eosinophils (Eos) are considered potential biomarkers for respiratory viral infections [38] and play a role in various important biological processes such as immune regulation [39], autoimmunity [40], and host defense against bacterial and viral infections [41]0.1 Under the action of cytokines, eosinophils in the blood and bone marrow can be recruited to the site of inflammation, thereby producing a large number of immune regulatory factors and pro-inflammatory factors. We found that there were significant differences in eosinophils in influenza and Mycoplasma pneumoniae infections. Compared with influenza, Mycoplasma pneumoniae patients had higher Eos# [0.010(0.000-0.030) vs. 0.120(0.040–0.278), p < 0.0001], which is similar to the report by Yan Q [42].
Monocytes (Mon) play an important role in antiviral immunity. They can directly phagocytose pathogenic microorganisms and can also participate in antiviral immunity through various antibody receptors and lymphokine receptors. When monocytes phagocytose antigens, their carried antigen-determinant clusters can be transferred to T lymphocytes to induce lymphocyte-specific immune responses. When inflammation occurs in the body, it may cause changes in the total number and percentage of monocytes. Therefore, compared with common cold patients, the increase in monocytes in influenza patients is more obvious. Our research also found that the Mon% of influenza patients [0.098(0.079–0.121)] is high, which is similar to the report by Zheng Y [43].
Platelets have many types of surface receptors, which can regulate the interaction between platelets and endothelial cells in an inflammatory state [44]. Some recent reviews have detailed the types and functions of these surface receptors in platelet-mediated responses, especially their interactions with bacteria, bacterial toxins, and endothelial cells [45, 46]. These studies have confirmed the association between platelet count (PLT) and inflammatory response and infection. In our study, we found that the PLT level of Mycoplasma pneumoniae patients [308.000(245.000-377.000)] was significantly higher than that of influenza patients [234.000(195.000-283.000)], p < 0.0001, indicating that the PLT level may play an important role in distinguishing these two diseases.
High fluorescence intensity cells (HFC) are a new type of peripheral blood parameter. In one study, researchers found that high fluorescence cells (HFC) combined with biochemical immune indicators have application value in identifying the nature of pleural effusion [47] and another study found that the absolute value and percentage of high fluorescence intensity cells have a certain value in the differential diagnosis of benign and malignant pleural effusion [48]. It can reflect the activity of immune cells. In cases of Mycoplasma pneumoniae, this activity may be more obvious [0.070(0.040–0.110)], compared with influenza cases, the activity is lower [0.030(0.020–0.040)], p < 0.0001. On the other hand, PLR (platelet to lymphocyte ratio) has been widely reported to be associated with respiratory diseases [49, 50] and participates in systemic inflammation and immune responses. Our research found that the PLR level of influenza cases [207.890(143.450–306.100)] was higher than that of Mycoplasma pneumoniae cases [145.985(104.515-184.162)], p < 0.0001. Therefore, PLR may be a valuable indicator to distinguish these two diseases.
We found that the indicators retained by the model have special significance for differentiating between Mycoplasma pneumoniae infection and influenza infection, but the model’s algorithm requires further validation. Consequently, we attempted to find new cases as an external validation set, using this set to analyze and verify the reliability of the model. We randomly selected a group of cases from the First Affiliated Hospital of Sun Yat-sen University, which were tested at the same time with the same equipment. These cases strictly met our inclusion criteria, namely, they were under 12 years old and there was no sex difference. In this way, we successfully obtained an external validation set. The development and validation of the IV@MP algorithm based on random forests showed good diagnostic performance, with an AUC of 0.845 in the external validation set. This highlights the potential of our model in assisting clinicians in accurately diagnosing these respiratory infections This result suggests that using combined indicators for diagnosis can better distinguish between the two, thus it has a higher value.
Our findings not only corroborate the universality and efficacy of our model but also underscore its potential in the broader context of respiratory pathogen diagnostics. Given the diverse spectrum of respiratory pathogens, including but not limited to Mycoplasma pneumoniae, influenza viruses, respiratory syncytial virus (RSV) [51], adenoviruses [52], human rhinoviruses [53], and the novel coronavirus (SARS-CoV-2) [54], each with distinct biological traits and clinical presentations, our model’s adaptability is particularly noteworthy. The prevalence of these pathogens fluctuates across different demographics and timeframes, emphasizing the importance of a diagnostic tool that can evolve with emerging data. Should ample data for other pathogens become available, employing a similar methodology could extend our diagnostic reach, thereby amplifying the comprehensiveness and effectiveness of our diagnostic toolkit.









留言 (0)