
記住我









Silicatosis is a lung condition caused by inhalation of silicates, which comprises silicates such as talc, mica, and kaolinite, as well as silicates such as fuller’s earth [4]. In general, silicates are less fibrogenic than silica. However, in prolonged and heavy exposure, and/or combined with silica, they can cause a fibrogenic pneumoconiosis. Clinical and functional features are similar to silicosis, whereas the radiographic opacities are more irregular. On morphology, there are no silicotic nodules, as the proportion of crystalline quartz in silica in the inspired dust is low (usually < 10%). The typical features comprise patchy and stellate-shaped centrilobular interstitial fibrosis (so-called “medusa head”) composed of a mixture of fibroblasts, collagen fibres, and dust-filled macrophages. There is abundant black carbon or brown iron dust mixed with numerous crystals with varying degrees of birefringence [22].
A special form of silicatosis is talc pneumoconiosis or talcosis. Indeed, talc is a frequent filler in medications used for oral consumption or may reach the lungs by the vascular route in drug abusers (intravenous injection of crushed tablets; in this case the talc granulomas are localized close to the pulmonary vasculature) [23]. At histology, focal peribronchial and perivascular fibrosis is associated with abundant dust deposits containing needle-shaped bluish-gray birefringent particles associated with giant cell response [23]. The number of macrophages and giant cells may be variable, and, in some cases, the granulomatous reaction is a close mimicker of sarcoidosis [23].
Other rare forms of dust-related diseases include coal worker pneumoconiosis, recently reported as an alarming resurgent pneumoconiosis [24]. Particulate matters directly interact with lung cells, leading to structural damage and the release of enzymes that contribute to lung scarring. Oxidative stress ensues as immune cells like alveolar macrophages scavenge particles, producing ROS and RNS that damage lipids, proteins, and DNA. This oxidative stress is exacerbated by the presence of heavy metals, transition metals, and polyaromatic hydrocarbons contaminants associated with the exposure. Moreover, inflammation and the production of growth factors are activated as lung cells release cytokines and growth factors in response to the exposure. These mediators recruit immune cells to the lungs, amplify inflammation, and activate fibroblasts, leading to the deposition of collagen and scarring of lung tissue. Genetic factors may also play a role in susceptibility to conditions like coal workers’ pneumoconiosis, with certain polymorphisms associated with increased risk and severity of the disease [25].
From the pathological point of view, two distinct forms are recognized: simple and complicated forms. The simple form comprises centrilobular macules, when associated with fibrosis, randomly distributed nodules in the upper lobes. The complicated form features are characterized by large and usually bilateral areas of fibrosis similar to progressive massive fibrosis. Progressive massive fibrosis is defined by the presence of a conglomerate of disease, at least 1cm in size, often associated with ischaemic necrosis, and associated with abundant dust laden macrophages with fibrosis. In both of them, there is an elevated black pigmentation that looks like the so-called “Medusa head”. The content of crystalline quartz, cristabolite, and tridymilite determines the pathological picture. Amongst anthracite coal workers, the high crystalline quartz provides a pathology similar to silicosis. For bituminous and lignite coal, with lower content quartz, the pathology is more that of a silicatosis. The pathologist can therefore provide information of likely prior exposure patterns. Nonetheless, birefringent particles may sometimes be detected within black areas, reflecting the mixed nature of coal dust. Emphysematous changes are typically present at the periphery of macules. Cavitation may occur as a complication of infection such as tuberculosis or ischemia due to vascular insult.
The most frequent occupational exposure of the above-described diseases is reported in Table 1.
Table 1 Occupational exposure profiles of silicates Key morphological featuresSilicatosis or other rare forms of dust: stellate-shaped centrilobular interstitial fibrosis composed of a mixture of fibroblasts, collagen fibres, and dust-filled macrophages. When nodules predominate, a diagnosis of silicosis should be made.
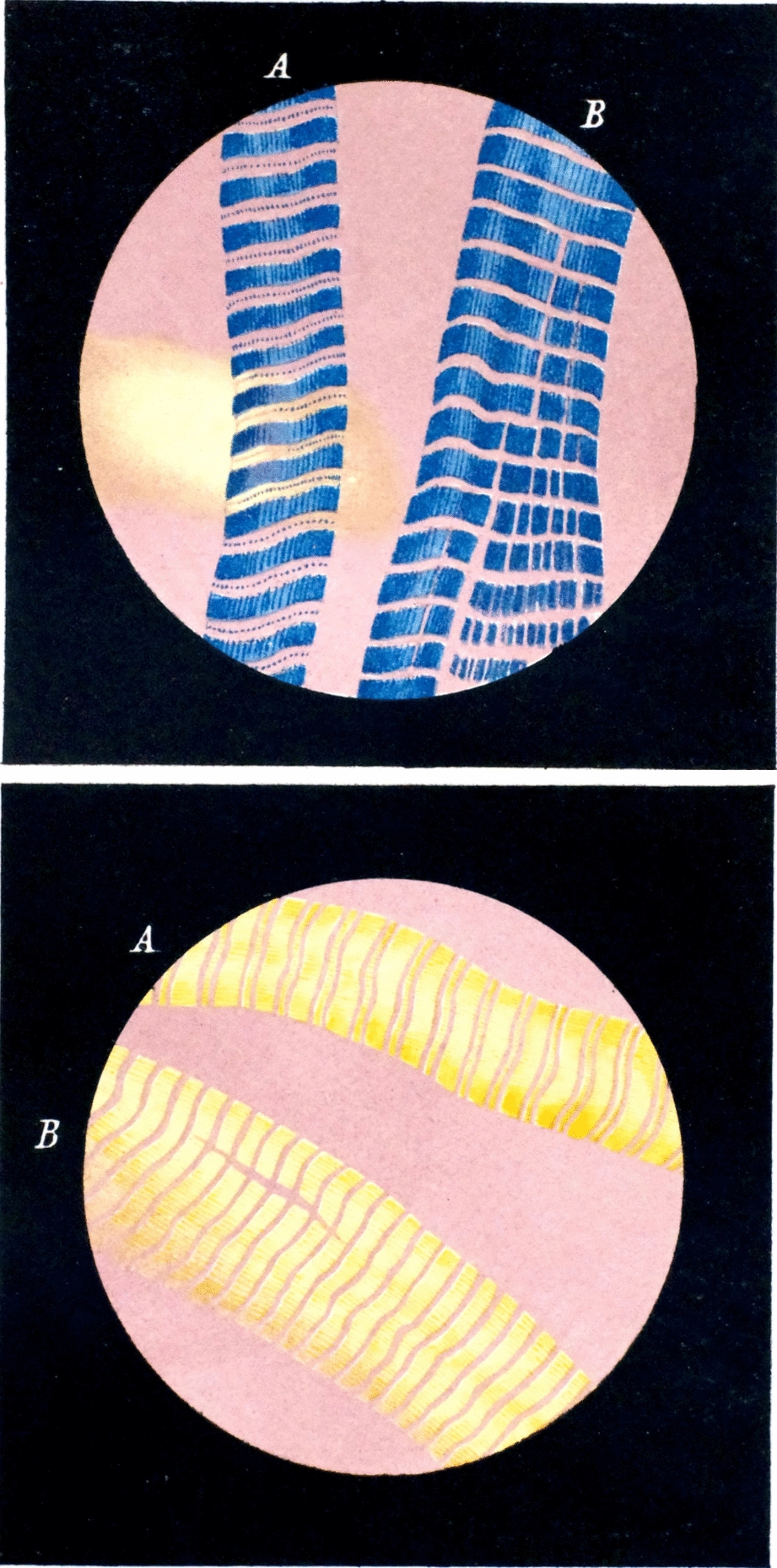
Supportive analyses a)Polarized light microscopy: birefringent crystals (silicates) in the centrilobular fibrotic brown areas of silicatosis.
b)Other investigations (used in referral centres): analytic electron microscopy and ion or laser microbe mass spectrometry (more frequently used for legal compensation).
SilicosisSilicosis is a fibrotic lung disease induced by inhalation of small particles (< 10 μm in diameter) of crystalline silica. Silica (silicon dioxide, SiO2) is a natural mineral, contained in more than 95% of the earth’s rocks. Historical and current occupational exposure are reported in Table 2 [24]. There are three different forms of silicosis whose clinical presentation is closely related to the cumulative dose of silica exposure [26]. Upon inhalation, freshly fractured silica particles trigger a complex cascade of pathological processes in the lungs. These particles can generate reactive free radicals on their surface, instigating DNA damage, mutations, and eventual cell death. Moreover, silica elicits a robust respiratory burst in lung macrophages, akin to the response seen with asbestos fibres, resulting in the release of oxidants, proteolytic enzymes, and pro-inflammatory cytokines such as TNF-α and IL-1β. This inflammatory milieu orchestrates the recruitment of additional inflammatory cells, perpetuating severe pulmonary inflammation.
Table 2 Historical and current occupational exposure to silicaOf note, chronic silicosis has a latency of 10 or more years of low to moderate exposure dose; accelerated silicosis occurs within 10 years of moderate to high levels of exposure, and acute silicosis, which is associated with a high concentration of crystalline silica, may occur within a week to 5 years from the initial contact [27]. Chronic silicosis presents as simple or nodular silicosis, which features fibrotic nodules (< 1 cm in diameter), usually in the upper lobes. The typical silicotic nodules appear as sharply circumscribed nodules consisting of whorled, densely hyalinized collagen. In the recently formed lesions, macrophages form a mantle around the fibrotic centre (Fig. 1).
Fig. 1
Silicotic Nodules. a The nodules exhibit a distinct morphology characterized by sharply circumscribed structures with whorled, densely hyalinized collagen (haematoxylin and eosin, scale bar: 500 µm). b In the early stages of lesion formation, macrophages envelop the fibrotic centre, contributing to the nodular structure (haematoxylin and eosin, scale bar: 300 µm)
Calcification and ossification may be detected in long-standing lesions. Examination with polarizing microscopy shows birefringent particulate within the fibrotic nodules. Larger brightly birefringent particles, which represent silicates or silicates-like particles, may also be detected. Silicotic nodules may also protrude through the visceral pleura. The nodules may merge to form fibrotic conglomerates (> 1 cm) typical of complicated or progressive massive fibrosis (PMF) [28, 29]. The pathological definition of PMF is still debated: for PMF to be correctly diagnosed, some have proposed an extension of at least 2 cm in any single dimension of tissue while others report that it should be at least 1 cm. Additional findings are enlarged mediastinal lymph nodes with nodular fibrosis and peripheral calcification (present in 75% of silicosis patients) [30, 31]. Acute and accelerated PMF has been described to occur in high-concentration exposure workers with a short latency. Acute silicosis or silico-proteinosis shows features of alveolar proteinosis, and accelerated silicosis may present fibrotic nodules and masses characteristic of PMF [26]. The granular eosinophilic material filling the alveoli is strongly positive to staining with periodic acid-Schiff-diastase (PAS-D). Conditions associated with silicosis comprise immunological disorders such as polyclonal hyper-gammaglobulinemia, increased rheumatoid factor or antinuclear antibodies, systemic sclerosis, and rheumatoid disease. Among all infective complications, tuberculosis is the most frequent infective complication [4]. Crystalline silica, particularly quartz, is also recognized as a potent carcinogen, classified as Group 1 by the International Agency for Research on Cancer (IARC). This classification is based on extensive evidence from epidemiological studies, animal research, and mechanistic studies demonstrating its association with lung cancer. Inhalation of quartz particles leads to the generation of ROS and RNS in the lung tissue, causing oxidative stress, DNA damage, and inflammation [25]. On the other hand, amorphous silica, lacking the crystalline structure of quartz, is generally considered to have a lower carcinogenic potential. While both forms of silica can cause respiratory diseases such as silicosis and fibrosis, epidemiological and experimental evidence suggests that amorphous silica is less likely to induce lung cancer. Regulatory agencies and health organizations typically classify amorphous silica as a lower hazard compared to crystalline silica in terms of carcinogenicity, reflected in occupational exposure limits and safety guidelines [32].
The most frequent histological differential diagnoses are reported in Table 3.
Table 3 Most frequent histological differential diagnoses of silicosis Key morphological features a)Chronic silicosis:
a.Nodules: discrete, black-pigmented fibrotic nodules, < 1 cm in diameter, frequently localized around respiratory bronchioles, small pulmonary arteries, and lymph nodes.
b.These nodules may coalesce in advanced stages giving the appearance of progressive massive fibrosis.
b)Acute silicosis:
a.Features typical of alveolar proteinosis (silico-proteinosis): granular eosinophilic material (strongly positive PAS/PAS-D).
Supportive analyses a)Polarized light microscopy: faintly birefringent particles within fibrotic nodules, which are not as extensive as in silicatosis.
b)Special stains or molecular investigation for microorganisms especially mycobacteria in case of cavitated nodules (so-called: silico-tuberculosis).
c)Other investigations (used in referral centres): analytic electron microscopy and ion or laser microbe mass spectrometry (more frequently used for legal compensation).
Metal-induced lung diseasesInhalation of metallic dust can cause different pulmonary diseases subject to host factors. While heavy metals encompass a broad spectrum of elements with diverse properties and potential health impacts, the focus in many reviews often centres on a select few metals. This selective attention is often driven by several factors, including the prevalence of certain metals in industrial processes, their widespread environmental distribution, and their documented association with significant health effects. Here we consider the most common pathological features: siderosis, aluminosis, berylliosis, and hard-metal disease.
Historical and current occupational exposure is reported in Table 4. Siderosis does not display a lung tissue reaction on exposure to iron oxide particles with only intrapulmonary pigment deposition appreciated. Iron is an inert metal with no pathogenicity to lung tissue. Usually, asymptomatic patients have no functional impairment, but imaging studies as well as histopathology show nodular accumulation characterized by macrophages loaded with yellow brown globules with dark centres [33]. A good example of siderosis is observed in arc welders. Fibrosis may be seen in forms with concomitant exposure to other fibrogenic dust such as in sidero-silicosis.
Table 4 Occupational exposure profiles of metals/hard metalsAluminosis is a rare disease caused by the inhalation of aluminium-containing dust. Aluminium is a lightweight metal widely used in industry; hypersensitivity to aluminium is believed to play a role in the pathogenesis of the disease [34]. The tissue reaction is variable from grayish dust-laden macrophages accumulated in perivascular and peribronchiolar areas to granulomatous inflammation, and in rare instances leading to interstitial fibrosis. The aluminium dust is refractile. Rare cases of alveolar proteinosis, similar to that seen acute silico-proteinosis, have also been reported [33].
Berylliosis is caused by the inhalation of beryllium containing dust. It induces diffused alveolar damage in the acute form, and non-necrotizing sarcoid-like granulomas in the chronic form with bilateral lymphadenopathy. Granulomas can sometimes show multinucleated giant cells with Schaumann and asteroid bodies. Pathogenetic mechanism is most likely a delayed hypersensitivity reaction associated with certain HLA haplotypes [35]. The differential diagnosis from sarcoidosis is impossible without clinical information or an environmental exposure history. Ancillary methods like positive beryllium lymphocyte proliferation test may be helpful in rendering correct diagnosis.
Hard metal lung disease: Hard-metal lung disease (HMLD) represents a hypersensitivity reaction caused by exposure to inhalation of hard-metal particles, whose major components are tungsten carbide (approximately 90%) and cobalt (approximately 10%) [36]. HMLD often manifests as giant cell interstitial pneumonia characterized by fibrotic thickening of alveolar septa accompanied by a mild/moderate chronic inflammatory infiltrate. Multinucleated giant cells, which are often bizarre cells, are a frequent feature and are found within both the alveolar space and lining of the alveolar septa. Giant cells can show features of emperipolesis. Heavy metals are naturally occurring elements characterized by their high atomic weight and density. The toxicity of heavy metals is influenced by several factors, including the amount of exposure, the route of exposure, chemical form, as well as individual factors such as age, gender, genetics, and nutritional status. Among the prioritized metals with significant public health implications are arsenic, cadmium, chromium, lead, and mercury. In this context, cobalt merits particular attention due to its prevalent use in hard metal alloys. While cobalt is not the only metal of concern, it is one of the major components found in hard metal alloys and has been associated with various health risks, including respiratory issues and dermatological reactions.
Causative metal is cobalt which is difficult to detect because of water solubility. Initially, it elicits fibrosis in the airway wall, which clinically manifests as small airway disease. It is estimated that only 1% of exposed individuals develop interstitial lung diseases, while asthma is diagnosed in 10% of exposed cases (Fig. 2).
Fig. 2
Pathological features in hard metal disease lung tissue. a Occasional features reminiscent of usual interstitial pneumonia (UIP)-like areas, characterized by microscopic “honeycomb” patterns indicative of fibrosis, can be detected (haematoxylin and eosin, scale bar: 3 mm). b Additionally, some macrophagic alveolitis with DIP-like features and several multinucleated giant cells are observed (haematoxylin and eosin, scale bar: 200 µm)
The most frequent histological differential diagnoses of the above-reported metal and hard-metal diseases are reported in Table 5.
Table 5 Most frequent histological differential diagnoses for metal/hard metal diseases Key morphological features a)Siderosis: peri-bronchial/perivascular deposition of dark brown to black material (iron oxide).
b)Aluminosis: peri-bronchial/perivascular deposition of refractile gray dust.
c)Berylliosis: well-formed non-necrotizing granulomas.
d)HMLD: giant cell interstitial pneumonia and multinucleated giant cells with emperipolesis.
Supportive analyses a)Special stains: iron stain useful in siderosis, and Irwin’s aluminon in aluminosis.
b)Polarizing microscopy: negative for all these dust particles with no birefringence detected.
c)Other investigations (used in referral centres): analytic electron microscopy, ion or laser microbe mass spectrometry, and wet chemical analyses, particularly useful in berylliosis, beryllium lymphocyte proliferation test.
Asbestos-related lung diseasesAsbestos is a collective term that defines a regulated group of six naturally occurring, highly fibrous silicate minerals. The six minerals fall into two groups: serpentine, of which the only asbestiform type is chrysotile (white asbestos), and amphibole asbestos, which comprises the commercial forms of asbestos—amosite (brown) and crocidolite (blue)—as well as the non-commercial forms: asbestiform tremolite, asbestiform anthophyllite, and asbestiform actinolite. The two groups—amphibole asbestos and serpentine chrysotile—have different physical, chemical, and biological properties. The propensity of asbestos minerals to induce disease correlates closely with the retention of biopersistent fibres in the body. Amphibole forms of asbestos are far more potent in the induction of disease than chrysotile. Although in the western world, the levels of exposure are currently kept in check by strict regulations, past asbestos exposure continues to affect many due to the latent nature of the pathophysiological response of the body to the inhaled fibres. Historical and current occupational exposures are reported in Table 6.
Table 6 Occupational exposure profiles of asbestosIn asbestosis, there is a significant influx of macrophages into the lung tissue, which triggers an upregulation of inflammatory mediators such as TNF and interleukins (IL-1β and IL-6) [37]. This inflammatory response is further intensified by the heightened generation of ROS. These inflammatory processes, coupled with increased ROS levels, contribute to the destruction of alveolar type 1 cells, impairing their ability to facilitate gas exchange. Concurrently, the deposition of asbestos fibres results in the formation of characteristic asbestos and ferruginous bodies. These bodies, composed of asbestos fibres enveloped in iron-containing proteins, serve as distinctive markers of chronic asbestos exposure. The toxicity of mineral fibres is influenced by various factors, including chemical composition, surface reactivity, crystallinity, and the presence of transition metals. Additionally, fibre size and shape impact their ability to penetrate the alveolar space and provoke an inflammatory response. Mechanistically, frustrated phagocytosis of longer asbestos fibres by alveolar macrophages leads to chronic inflammation, activating the NLRP3 inflammasome and promoting malignant transformation. The WHO defines asbestos based not only on mineralogy but also on fibre dimensions. The NLRP3 inflammasome responds to diverse stimuli, including asbestos and carbon nanotubes, inducing granulomatous inflammation. Scavenger receptors, particularly MARCO and SR-B1, play a role in recognizing and mediating the cellular uptake of asbestos fibres, contributing to pulmonary fibrosis and asbestos-related diseases.
Indeed, long asbestos fibres, which persist in the pleura, trigger prolonged inflammation due to frustrated phagocytosis, leading to the activation of the NLRP3 inflammasome and the release of inflammatory cytokines like IL-1ß. This chronic inflammatory state generates ROS and RNS capable of causing DNA damage. Additionally, the presence of excess iron, associated with asbestos bodies further exacerbates carcinogenesis. Mutations in the BAP1 gene, observed in a significant proportion of mesotheliomas, play a crucial role in suppressing cell death mechanisms. BAP1 mutations enable mesothelial cells to evade apoptosis and accumulate further DNA damage, leading to carcinogenesis. The BAP1 protein regulates DNA repair and apoptosis following DNA damage, and cells with reduced BAP1 activity are less susceptible to cell death processes like ferroptosis. Furthermore, HMGB1 released during cell necrosis promotes autophagy and suppresses apoptosis, facilitating the accumulation of mutations associated with carcinogenesis. In summary, asbestos creates a mutagenic microenvironment rich in ROS and HMGB1, promoting DNA damage in mesothelial cells. Subsequent mutations, particularly in genes like CDKN2A, NF2, and TP53, accumulate due to the impaired cell death mechanisms mediated by BAP1 mutations. As consequence, the adverse effects of asbestos generally fall under two major categories: non-neoplastic (pleural thickening, effusion and plaque, and asbestosis) and neoplastic thoracic disease (mesothelioma and lung carcinoma).
Here, we particularly emphasize the pathological features of asbestosis, mesothelioma, and lung carcinoma.
AsbestosisAsbestosis is defined as diffuse pulmonary fibrosis due to a prolonged cumulative inhalation of massive doses of asbestos fibres with a positive correlation between the number of asbestos fibres and the severity of the disease. The latency period is approximately 15 years but could be longer. The disease may continue to progress even if occupational exposure has ceased.
In 2010, a joint report by the Asbestosis Committee of the College of American Pathologists and the Pulmonary Pathology Society published by Victor Roggli et al. [38], updated the diagnostic criteria, which was followed by an update in 2016 [39], responding to critical issues addressed after the initial publication. The diagnosis is usually based on (1) previous history of exposure to any type of asbestos fibres (AF), (2) clinical findings, (3) CT scan showing reticular linear diffuse opacities in the lower lobes, (4) restrictive alterations of lung functions and alteration in CO transfer, and (5) in some cases hyaline fibrous plaque or diffuse pleural fibrosis. Criteria 1 and 3 are mandatory for clinical diagnosis in symptomatic patients. However, even in the second half of the twentieth century, many cases of asbestosis remain asymptomatic. In asymptomatic patients, histologic assessment is required when the context of AF is equivocal when the clinical or radiologic features are atypical in the case of associated lung cancer, or at autopsy for medico-legal purposes. The disease is more severe in the sub-pleural regions and lower lobes.
A pathologist is required to identify both the pattern of interstitial lung fibrosis—in asbestosis it is defined as acellular and collagenous rather than fibroblastic and inflammatory, plus the presence of necessary biomarkers of asbestos exposure—either asbestos bodies determined by light microscopy, or asbestos fibres defined by mineral analysis. Attanoos [40] showed that the pattern of lung fibrosis in asbestosis is one best regarded as a fibrotic non-specific interstitial pneumonia (NSIP) with subpleural accentuation and fibroelastotic degeneration rather than a usual interstitial pneumonia. The presence of UIP should alert the pathologist to a causation other than asbestos, such as idiopathic pulmonary fibrosis, chronic hypersensitivity pneumonitis, or collagen vascular disease. The asbestos body count requires the presence of two asbestos bodies (AB) (rod-like beaded or dumbbell-shaped structures with a thin translucent core) per square centimetre on fresh or formalin-fixed tissue biopsy samples (from the peripheral lower lobe) to exclude the diagnosis of fibrotic NSIP with subpleural accentuation. Cryobiopsy has recently been found to allow for larger specimens compared to transbronchial biopsy which should not be performed in this setting except in exceptional circumstances. BAL containing > 1 AB/ml indicates a high probability of AE [41].
Histological features include diffuse fibrosis, which is characteristically paucicellular, more collagenous than fibroblastic, with lack of inflammation, numerous intra alveolar macrophages, most severe at the periphery of the lung with some degree of pleural fibrosis, and commonly with pleural plaques. Fibroblastic foci are very uncommon (Fig. 3).
Fig. 3
Histopathological characteristics of asbestosis. a Lung tissue from a patient with asbestosis with a fibrotic thickening of two close respiratory bronchi (dotted lines), extended to some alveoli (haematoxylin and eosin staining, scale bar: 3 mm). b Microscopic examination using Perls stain highlighted an asbestos body (Perls Prussian blue stain, scale bar: 200 µm)
In early asbestosis, the grading scheme proposed by Roggli et al. [38] is subdivided into four grades (see table 7). Initially, the fibrosis is limited to the wall of the alveoli around the bronchioles. However, small airway disease (≤ 2 mm) is still a matter of debate [42]. To avoid confusion with smoking bronchiolitis, in 2016 [39], the committee decided that patients with only bronchiolar wall fibrosis have obstructive disease rather than asbestosis. Accelerated asbestosis may occur with a fibrotic lung without honeycombing in association with numerous AB caused only by amphiboles.
Table 7 Histologic grading scheme according to Roggli and Sporn modified 2010–2016 from the scheme presented by Craighead et al. (Archi Pathol Lab Med 1982) Key morphological featuresKey features with the respective grading score are reported in Table 7. However, the hallmark of the disease is the occurrence of asbestos bodies (at least 2/cm2).
Supportive analyses a)Special stains: iron stain is useful since it may facilitate the detection of asbestos bodies (deep blue colour).
b)Polarizing microscopy: not useful.
c)Other investigations (used in referral centres): analytic electron microscopy. Mineral analysis may be conducted by various methods—light microscopic methods are now recognized as of limited utility as they cannot characterize minerals and do not detect most small particulates. Electron microscopy is useful in determining disease diagnosis and disease causation—it has particular use when the exposure history is not clear.
MesotheliomaAmong asbestos-related diseases, mesothelioma is certainly the most common. Diffuse mesothelioma is the most frequent primary neoplasm of the pleura, strongly associated with occupational exposure to commercial amphibole asbestos in more than 80% of men and 20–40% of women after latency period of 30–40 years. Other rare causes include different mineral fibres, such as erionite, and therapeutic and occupational radiation, with mesothelioma development occurring only 10 years after exposure [43]. Amongst patients with mesothelioma with no clear external exposures, there is a clear recognition that these arise through internal genetic mechanisms associated with age and cumulative DNA replicative mutations. Germline mutations with pathogenic variants are found in 12% of patients, with 25% of those exhibiting the BRCA1-associated protein-1 (BAP1) predisposition syndrome [44]. This group is reported to have an increased risk of developing mesothelioma at a younger age. Subjects with mesothelioma associated with inherited genetic syndromes are considered more likely in those < 50 years age; in those with peritoneal site disease; epithelioid histology, low grade with high inflammatory tumour microenvironment pathology, a personal history of cancer, and a family history of cancer. Amongst young subjects, especially with peritoneal mesothelioma, there is a requirement for testing for specific genetic fusions. The fifth edition of the 2021 WHO classification [45] has changed the terminology of malignant mesothelioma to mesothelioma (“malignant” is no longer recommended) and has maintained the subdivision into three major subtypes (epithelioid, biphasic, and sarcomatoid) regardless of whether the tumour is diffuse or localized. The most significant changes of the fifth WHO classification is the identification of mesothelioma in situ (MIS) in the clinical context of an unresolving pleural effusion with no radiological or thoracoscopic evidence of tumour. MIS is described as a pre-invasive single-layer surface proliferation of neoplastic mesothelial cells showing either BAP1 nuclear loss or MTAP cytoplasmic loss by immunostaining a surrogate of CDKN2A homozygous deletion by fluorescence in situ hybridization assay (Fig. 4).
Fig. 4
In situ mesothelioma. a The image shows the abnormal growth of neoplastic mesothelial cells in a single layer (haematoxylin and eosin, scale bar: 200 µm). b The immunohistochemical staining pattern demonstrates a notable loss of BAP1 expression (BAP-1 immunohistochemistry, scale bar: 200 µm)
The diagnosis cannot be made on cytology alone and needs a minimum of 100 to 200 mm2 of biopsy tissue sample. A multidisciplinary approach is essential [45]. Recently, Galateau Salle et al. reported a series of MISs mimicking well-differentiated papillary mesothelial tumours (WDPMT) showing BAP1 loss, supporting the decision to change the terminology of well-differentiated papillary mesothelioma in WDPMT to avoid confusion and misdiagnosis for treatment and medico-legal purposes [46]. Indeed, WDPMT is a single or multifocal papillary lesion, with retained BAP1 and absence of CDKN2A homozygous deletion lesion characterized by a slowly growing disease, usually without relation to asbestos exposure [45]. Although mesothelioma is a particularly aggressive tumour, with a survival of nearly 12 months without treatment, and with less than 5% of patients alive at 5 years, the prognostic value of histopathological subtypes impacts treatment decisions and surgery options. Epithelioid mesothelioma (EM) is the most frequent subtype (~ 80%) with a slightly better survival compared to the highly aggressive sarcomatoid mesothelioma (SM) (7%) which is drug resistant, and the biphasic subtypes (13%) with survival usually being dependent on the percentage of the sarcomatoid component [47].
At histology, a major effort has been made to better stratify the histopathologic characteristics divided into architectural pattern, cytological, and stromal features according to prognostication (Table 8) [47]. The key histological features of epithelioid subtypes of poor prognosis are solid and micropapillary, architectural pattern, and highly aggressive pleomorphic cytological features (large anaplastic and giant cells and bizarre nuclei), while EM with myxoid stroma and < 50% of solid component support the best prognosis. Lympho-histiocytoid mesotheliomas that may mimic lymphoma or lymphoepithelial carcinomas are also indicators of a better prognosis. Grading has emerged as an important prognostic factor only for epithelioid subtype and a two-tiered grading system (low versus high grade) based on atypia; mitotic count and necrosis have been integrated in the fifth WHO edition (Table 9) [
留言 (0)