
記住我





The expected cumulative chance of a live birth is key to outline the prognosis of any patient seeking fertility preservation. Time to treatment, woman age and ovarian reserve biomarkers are the possible limiting factors. Indeed, women wishing to preserve their future chance of conceiving might have to play against the clock or, in the worst scenario, they might have to face the absence of time left to allow a non-negligible chance of success. An evidence-based definition of the appropriateness of fertility preservation, should pass through the personalised evaluation of the ovarian function of each woman, which includes her hypothetical chance of obtaining a live birth, based on age and ovarian reserve, and, if relevant, the putative effect of other factors (i.e., autoimmune, genetic, oncologic conditions and their treatments) on both ovarian reserve and oocytes competence. All these factors influence the chances of conception and taken together define the “biological ovarian age” concept.
Ovarian reserve testingAge, other than being a predictor of oocytes’ quality, is the main (physiological) reason for ovarian reserve quantitative decline. Notably, different clinical conditions, including endometriosis and ovarian surgery, autoimmune diseases, genetic diseases, and previous gonadotoxic treatments, may negatively impact on the ovarian reserve. Sometimes, the ovarian reserve is reduced without a clear cause (idiopathic diminished ovarian reserve or premature ovarian insufficiency). For these reasons, the estimation of ovarian reserve, through specific tests, is a crucial step in defining the biological ovarian age, which may or may not conform to the chronological age of the patient [5].
The parameters used in the estimation of the ovarian reserve are either biochemical (follicle stimulating hormone, FSH and Anti-Müllerian Hormone, AMH) or morphological (antral follicles count, AFC). FSH plasma concentrations at the start of the menstrual cycle represent a biochemical parameter widely used in the past. This measurement is being gradually abandoned since it shows a wide intra- and inter-cycle variation, and does not show a close correlation with the AFC [6]. Circulating FSH has a significant negative predictive value only with values above 20 mIU/ml [7]. The values of circulating AMH and AFC are instead strongly correlated to the ovarian reserve, reflecting the number of follicles potentially recruitable with controlled ovarian stimulation (COS) [8, 9]. The AFC is measured by transvaginal ultrasonography and it consists in counting the number of small antral follicles (< 10 mm of mean diameter) present in the ovaries in a specific time of menstrual cycles. AFC strongly correlates with AMH circulating concentrations, since it is produced by the same antral and preantral follicles. AFC and AMH are currently the most sensitive indicators for a quantitative evaluation of the ovarian reserve and as predictors of ovarian response to COS. They are not, however, predictive of oocytes’ quality and of the chances of obtaining a spontaneous pregnancy in the short term [9].
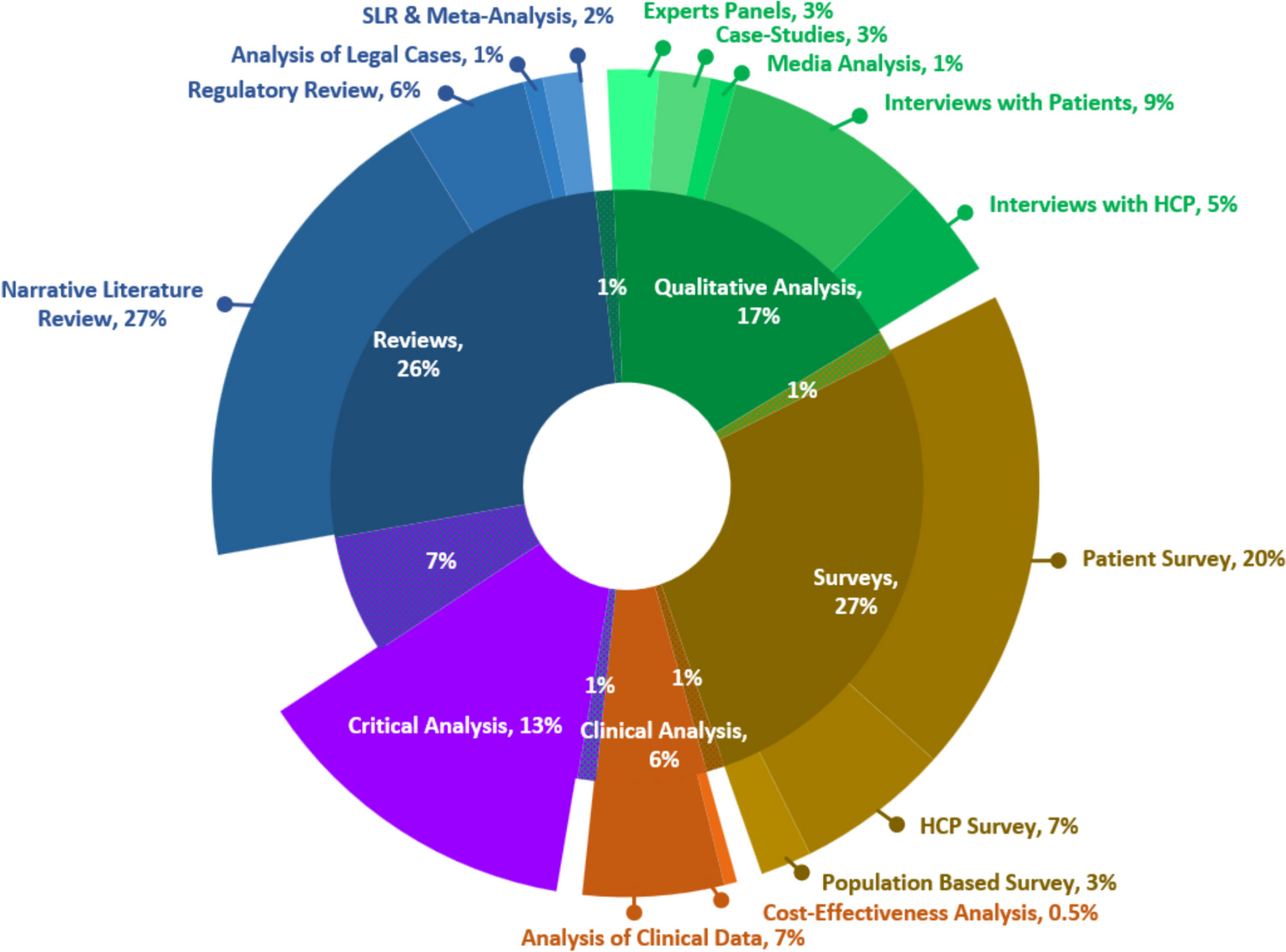
Factors that may influence ovarian ageFertility preservation has been traditionally focused on cancer patients at high risk for their reproductive health. However, a wide array of other factors may increase the risk of not being able to reach the desired family size (see Fig. 1).
Fig. 1
Factors that may influence biological age, reducing the ovarian reserve
Environment and lifestyleWhile a comprehensive discussion of all the lifestyle and environmental factors that may influence fertility is outside the scope of this paper, it's noteworthy to mention some that have demonstrated disruptive effects [10]. Cigarette smoking affects all stages of reproduction, being associated with lower fecundity rates, adverse pregnancy outcomes, and ultimately an earlier onset of menopause [11]. The effects of alcohol on female fertility are more inconsistent and probably a low-moderate use does not affect the ovarian reserve. On the contrary, the effects of alcohol on implantation and pregnancy are well known, and pregnant women should abstain completely from alcohol intake [12]. The use of illicit drugs is related to ovulatory and menstrual disturbances and to adverse pregnancy outcomes [12], but no effect on the age of menopause has been reported. It has to be noted that an abuse of all the mentioned substances might also determine epigenetic changes and DNA damage in germ cells, potentially resulting in inherited imprinting and genetic defects [13].
Endocrine disrupting chemicals (EDCs) may be found in a variety of foods and beverages, in the water and in the air [10]. Bisphenol A (BPA), 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD), methoxychlor (MTX), and phthalates have all been demonstrated to interfere with human folliculogenesis, ultimately reducing the follicle pool and potentially causing early ovarian failure [14]. However, the combined toxicity of EDCs on human reproduction, as well as the protective role of the body’s antioxidant systems, is a complex phenomenon, only partially understood that warrants further research.
Endometriosis and other benign gynaecological diseasesVarious benign gynecological conditions, such as endometriosis or dermoid cysts, can significantly influence ovarian age and consequently affect reproductive potential in multifaceted ways [15]. The ovarian damage may arise from: the effect of time on ovarian reserve as for some diseases, such as uterine myomas, a recovery time is required post their removal before trying to conceive; the direct negative effects of the disease itself (for instance, in endometriosis); and/or the potential iatrogenic consequences resulting from surgical treatment on the ovary, especially when bilateral [15]. However, quantifying the precise reproductive risks posed by each benign pathology or their treatments remains challenging due to the scarcity of reliable data. For instance, any ovarian surgery inevitably compromises a portion of the healthy ovary, leading to an unavoidable reduction in ovarian follicular reserve. This reduction varies depending on factors such as the extent of the pathology, its bilateral nature, and the surgeon's expertise [16].
Among these conditions, ovarian endometriosis and its association with infertility have garnered the most attention in research. Managing endometriosis involves a combination of medications and surgeries aimed at alleviating symptoms and eradicating visible implants. Despite these efforts, the chronic nature of endometriosis and its high recurrence risk often result in repetitive surgeries, potentially culminating in premature ovarian insufficiency (POI) [17]. Furthermore, even in cases where surgery is not pursued, ovarian reserve appears to be decreased in some studies, especially in women with ovarian endometriosis [18]. One possible pathogenic mechanism proposed was follicle depletion due to the excessive activation of primordial follicles triggered by pro-inflammatory pathways such as the PI3K-PTEN-Akt pathway [19]. Moreover, reactive oxygen species (ROS) and proteolytic substances permeating the surrounding tissues were hypothesized to cause the substitution of normal ovarian cortical tissue with fibrous tissue causing follicular loss and intraovarian vascular injury [20].
Available data on fertility preservation in women with endometriosis are scant and support the notion that age would be the most important prognostic factor. However, the cumulative live birth rate (CLBR) seems to be significantly reduced in young women (less than 35 years old) who received ovarian surgery compared to age-matched non-operated women with the disease (CLBR 72.5 vs 42.8% respectively) [21]. These data also show that CLBR is comparable in endometriosis and elective fertility preservation candidates, supporting the available evidence about the quantitative and not qualitative effect of endometriosis on ovarian function [21, 22]. Obviously, women operated two or more times are at higher risk of ovarian failure, and their CLBR decreases together with the reduction of the number of oocytes obtained from a single stimulation [21, 23]. To optimise the chances of reaching the desired family size, fertility should be repeatedly discussed, starting from diagnosis, including the possibilities for fertility preservation, when indicated. According to the available data, the ideal candidates for fertility preservation should be young women with a diagnosis of ovarian endometriosis, before surgery and ideally before age 35, since in this scenario the highest risk of recurrence and the best CLBR coexist.
Fertility counselling is indicated also before ovarian surgery for reasons other than endometriosis, especially when there is a chance of recurrence and/or bilaterality. Dermoid cysts (or mature teratomas) represent up to 70% of benign ovarian tumours in women under the age of 30; the total recurrence rate following cystectomy is 11% [24]. In 90% of the cases, the cysts are unilateral and about 1–2% may undergo malignant transformation [25]. No data are available on the risk for future infertility in this population. However, given their frequency and risk for multiple ovarian cystectomies, an estimation of individual risk of fertility loss should be proposed.
Autoimmune diseasesAutoimmune diseases (AD) affect approximately 5% of the population with a clear gender bias, occurring at a rate of 2 to 1 amongst women [26]. Importantly, many of these conditions often first manifest or are diagnosed during reproductive age, with possible significant implications for fertility and pregnancy outcomes [27,28,29].
The relationship between AD and fertility is highly heterogeneous, varying from one pathology to another and within each individual case. Generally, patients with AD are at a higher risk of infertility and tend to have lower parity compared to the general population. [30, 31]. Several putative mechanisms have been advocated. Firstly, specific autoimmune disorders carry an increased risk of POI, which can be either idiopathic, part of an autoimmune polyglandular syndrome [32] or iatrogenic, as a consequence of gonadotoxic treatments (for example cyclophosphamide for systemic lupus erythematosus and vasculitis [33, 34] or the autologous hematopoietic stem cells transplantation for multiple sclerosis [35]). Furthermore, these patients are more likely to experience recurrent miscarriages, preterm birth, and other obstetrical complications, compared to the general population [36], the most known and studied association being with antiphospholipid syndrome [37].
A second factor contributing to poor reproductive outcomes in patients with AD is the "time window" in which they may be required to postpone pregnancy. This circumstance may arise due to the requirement for invasive investigations, during which pregnancy is contraindicated, or the need to attain disease stabilisation before actively pursuing pregnancy [28]. As a result, there can be a considerable duration in which patients are unable to fulfil their desire for pregnancy, despite their longing to do so.
The presence of AD is also known to lead to sexual dysfunction due to chronic fatigue, pain, anxiety, depression, negative body image and reduced libido [38]. These effects can be related to the disease itself and/or be a consequence of pharmacological treatments used to manage the condition. Lastly, certain AD are associated with other causative conditions of infertility. For example, there is a high correlation between multiple sclerosis and endometriosis, both of which can contribute to fertility challenges in affected individuals [39].
It is important to note that the impact of autoimmune disorders on fertility is complex and multifaceted, and the specific effects can vary widely depending on the individual and the autoimmune condition they have. Hence, it is essential to conduct comprehensive reproductive counselling at the time of an AD diagnosis, providing patients with insightful information regarding the potential reproductive risks they may face in the future. When appropriate, the potential benefits of oocyte cryopreservation should be discussed. This counselling should be personalised, considering the individual's specific characteristics such as age, partner status (if any), pregnancy desire and any existing comorbidities.
Genetic disordersSeveral genetic disorders result in a diminished ovarian reserve and therefore could represent an indication for fertility preservation [40]. Together with the fertility evaluation, a preconception genetic counselling regarding the chances of transmissibility of the genetic disease/predisposition to the offspring and possibilities and limits of preimplantation genetic testing for monogenic diseases (PGT-M) and prenatal diagnosis (when applicable), is recommended [40, 41].
Turner syndrome (TS) or monosomy X is a chromosomal disorder affecting approximately 1 in 2,500 live-born females [42]. Only 2–5% of the affected women has regular menstrual cyclicity and the chance to obtain spontaneous pregnancies [43]. Indeed, women with full 45 X genotype usually reach POI as adolescents, with small fibrous ovaries. On the other hand, in TS mosaic genotype a residual ovarian activity could be observed through adolescence and early adulthood [44]. The crucial issue is to identify women with residual ovarian function that could be candidates for fertility preservation and to define the perfect timing for it. AMH represents a promising marker of ovarian function in TS women [45]: women with AMH below 8 pmol/l are at increased risk of POI with a sensitivity and specificity of 96% and 86%, respectively [45]. AMH levels correlated also with breast development and spontaneous menarche [46]. In prepubertal girls, ovarian tissue cryopreservation through the removal of an entire ovary may represent an option for future fertility preservation [47]. In post pubertal women oocytes cryopreservation represents another valid option: a few case series confirmed satisfactory results, with a range of mature oocytes of 8.1 ± 3.4 [48]. A careful preconceptional evaluation of TS women should be carried out taking into account that there is an increased risk of endocrinological disorders, hypertensive disorder and diabetes [49]. Cardiac evaluation and the assessment of aortic dissection risk is strongly recommended in women with TS: an aortic size index above 2 cm/m2 is a contraindication for pregnancy [50].
X fragile premutation (FMR1) consists in the expansion of CGG repeat to 55 to 199 copies in untranslated FMR1 genes [51] and is associated with a high risk of infertility and POI [52]. In women with FMR1 with an adequate ovarian reserve at the time of the consultation, oocytes cryopreservation could be proposed despite the very few data available in literature [53]. Interestingly, a retrospective analysis of 18 carriers of FMR1 premutation showed a positive correlation between CGG repeats and the number of oocytes retrieved [54]. PGT should always be offered in this condition to avoid full X fragile disorder in the offspring. Pregnancy outcomes in women with FMR1 premutation seems comparable to the general population [55].
Galactosemia is a rare, hereditary disorder of carbohydrate metabolism that affects the body's ability to convert galactose to glucose. It was estimated that more than 70% of women with this condition are at risk of POI at a mean age as young as 13 years [56]. Despite this, natural conception is not impossible: literature shows how it may happen in up to 40% of cases within one year from the POI diagnosis [57, 58]. Fertility preservation through oocytes cryopreservation could be offered to women not desiring a pregnancy at the time of the consultation, despite some studies reporting a reduced response to gonadotropin in women with classic galactosemia compared with age-matched controls [52]. In young prepuberal women ovarian tissue cryopreservation is the only option, with few cases reported in literature, however the patient should be informed that transplanted tissue will face premature functioning failure due to the primary disease [52, 59]. Few data are available about maternal and neonatal outcomes of pregnancies in affected women. In particular the role of galactose metabolites on cognitive long-term functioning of children has not yet been fully investigated [57].
It is well established that BRCA 1–2 mutated carriers are at risk of breast and ovarian cancer. The current guidelines recommend prophylactic bilateral oophorectomy by the age of 40–45 years of age and the fertility consultation should take place before the occurrence of cancer [60]. Cryopreservation of oocytes is an established procedures in these women with good outcome and the possibility to perform PGT-M to prevent transmission in the offspring [60] Ovarian response seems to be similar comparing BRCA carriers to non-carriers [61]. On the other hand, there are conflicting evidence regarding the impact of BRCA mutation on ovarian reserve [62, 63]. Pregnancy appears to be safe in BRCA mutated carriers, even after a previous breast cancer, and does not affect their oncological prognosis [64].
Idiopathic premature ovarian insufficiency (POI)POI affects approximately 1% of the population and, while it can be related to many etiological factors, such those discussed above, in the majority of cases POIs are idiopathic [65].
Some irregular and unpredictable ovarian activity can occur in up to 25% of these women, mainly within one year of diagnosis, with pregnancy reported in up to 5% of cases [66]. However, it is crucial to understand that when there is clinical evidence of POI, the opportunity for fertility preservation has probably already expired since its success depends on the number of oocytes retrieved [67].
Cryopreservation of oocytes, embryos or ovarian tissue can be considered when the risk of POI is assessed early, however, safety and efficacy data lacks in this population [66]. Ovarian tissue cryopreservation may be a successful strategy since it enables fertility preservation at a very young age, including prepubertal girls, and ovarian function restoration for a few years [68]. However, mild clinical symptoms (for example, in very young women vasomotor symptoms are usually absent [69]) and a relative lack of awareness makes such an early evaluation difficult [70].
A detailed family history, especially maternal age at menopause, can be useful to rise suspicion, since it has been demonstrated that first-degree relatives of women with POI have an 18-fold increased risk of POI compared with controls relative risk [71]. These data support the hypothesis of a genetic aetiology of POI, in line with an increasing number of studies demonstrating that multiloci analysis could increase the diagnostic power and the accuracy of POI diagnosis up to 75%, in contrast to the current 25% of positive diagnosis obtained by screening few POI genes [71,
留言 (0)