This cohort exhibited several clinical and laboratory markers associated with an increased risk of progression to surgery or death following NEC diagnosis, many of which corroborate existing studies. Unlike the medical NEC group, the surgical NEC group exhibited significantly lower platelet levels at 24-, 48-, and 72 h post-diagnosis, as well as a significant drop in values between 24 and 48 h. This finding is consistent with previous literature, which demonstrates that a lower platelet count is associated with a greater extent of intestinal deterioration and that platelets are lower in infants who die from NEC than in survivors [13, 14].
Prior research has demonstrated elevated CRP is a biomarker for NEC diagnosis and elevated CRP concentrations are associated with higher risk of surgery [15, 16]. The CRP levels of the surgical NEC group were consistent with this trend, with a significant and rapid rise in CRP between 24 and 48 h post-diagnosis. CRP has been previously shown to be an indicator of antibiotic responsiveness, thus increasing CRP concentrations in the setting of surgical NEC suggests a failure to respond to initial antibiotic treatment [17]. While CRP is nonspecific and cannot be used to exclude or confirm a diagnosis of NEC, it has utility as a marker of disease progression in known cases of NEC. Other significant laboratory differences included both peak and nadir WBC counts within 3 days of diagnosis, with surgical NEC showing higher peak WBC counts and lower WBC nadirs. Also, surgical NEC was associated with lower hemoglobin and hematocrit levels proximal to the time of diagnosis. These findings reflect the critical illness associated with surgical NEC as compared to medical NEC. There were no differences in peak bilirubin levels taken proximal to the time of diagnosis.
A positive blood culture and the need for vasopressors or intubation within 24 h of diagnosis were also associated with NEC severity, supporting prior similar findings [14]. When taken together, the above laboratory and clinical indicators may be used to assess an infant’s likelihood of progressing to surgery or death at the time of diagnosis and “flag” high-risk cases for increased monitoring and lower clinical threshold for surgical intervention.
Consistent with the standing literature, intake of any maternal milk was associated with medical NEC vs. surgical NEC in this cohort, though this result was not significant. Babies receiving fortification of any human milk also showed significantly less progression to surgery or death than babies receiving unfortified milk. This association remained even after adjustments for age of diagnosis and birth weight, meaning this finding was not associated with the timing of the feeding protocol. Clinical events prompting medical providers to remove fortifiers may contribute to this relationship. For example, the perceived reaction to fortification and subsequent removal of HMF may be a risk factor for the development of severe NEC. Feeding type (mother’s milk vs. formula) has been shown to alter splanchnic intestinal blood flow in neonates [18]. It is unknown if the increasing caloric density of nutrition affects splanchnic blood flow or tissue oxygenation during digestion. Feeding intolerance may serve to unmask other hemodynamic issues such as a patent ductus arteriosus. However, the removal of fortification (or withholding fortification) did not seem to protect neonates against the development of severe NEC in this cohort, as many of the severe NEC cases were not receiving fortification at the time of diagnosis (Fig. 1).
Alternatively, fortification may be protective against severe NEC. Prior studies have demonstrated similar or reduced rates of NEC with earlier receipt of human milk fortification, though the overall relationship is not well understood [6, 10, 19]. Overall, these findings support the idea that early fortification and strict adherence to feeding protocols may help reduce cases of NEC-related surgery and death [20].
This study did not find a significant difference in NEC severity between infants fed with formula versus human milk, though an increased incidence of NEC in formula-fed neonates has been extensively observed [3, 7, 21]. The majority of infants included in this study were premature and received either donor human milk or maternal milk by protocol, therefore this study was not large enough to observe this effect. As a follow-up to a previous pilot study, this data did not show a significant correlation between NEC severity and the time between NEC diagnosis and antibiotic initiation [22].
This study identified a novel risk factor in the development of severe NEC: abdominal circumference at birth was significantly larger in the surgical NEC group, even though these neonates trended towards having lower birth weights (Table 1). This suggests that increased abdominal circumference at birth may be associated with a higher risk of progressing to surgery or death following NEC diagnosis. This could signify early-onset intestinal immaturity and underlying motility issues in these infants, predisposing these infants to more severe GI outcomes. Abdominal distention is a common presenting clinical sign preceding NEC diagnosis, though NEC did not occur until the mean day of life 29.4 in this cohort; therefore, this marker could be detected approximately 30 days before full disease onset. Interestingly, a study found that preterm infants with a higher risk of NEC had altered superior mesenteric artery dopplers on day of life 1 [23]. Therefore, distension may be related to poor motility or a consequence of intestinal blood flow. Of note, many hospitals nationwide have recently discontinued the measurements of abdominal circumference in their standard anthropometric birth measurements. A limitation of this observation includes the evaluation of positive pressure support or ventilation at delivery. Delivery interventions were not analyzed in this study. Further research may be warranted to confirm the significance of this measurement as a risk factor for severe NEC.
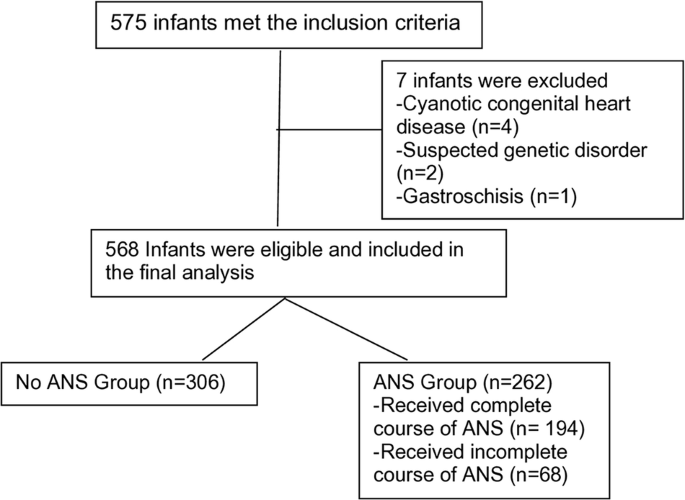
In this cohort, there was a higher proportion of neonates who received antenatal steroids (ANS) in the surgical NEC group as compared to the medical NEC group. This could be an effect of ANS being more often administered to smaller and more premature neonates; however, the relationship and its significance remained after adjustment for gestational age and birth weight. This finding was initially surprising as multiple sources, including a 2017 Cochrane meta-analysis report, lower the overall incidence of NEC with receipt of ANS [7, 24]. However, the association between ANS use and NEC severity is not well studied, and other studies report similar findings to those seen in this cohort. Chawla et al. released a cohort study in 2022 reporting higher rates of medical NEC, 12.3% vs. 6.9% (OR 1.30, 95% CI 0.56–3.04), and higher rates of surgical NEC, 6.6% vs. 4.2% (OR = 2.05; 95% CI 0.57–7.35), among neonates receiving a complete course of antenatal steroids between 21 and 22 weeks gestation as compared with those receiving partial or no steroids, though there was a lower rate of all-cause death (including that from surgical NEC) among the group receiving a complete course of steroids (OR 0.69; 95% CI 0.42–1.15) [25]. Though their results regarding NEC did not reach significance, they showed the same trends seen in this study (i.e. lower rates of surgical NEC with increased ANS receipt) throughout all of their comparisons. Other studies report neither a risk nor protective relationship between ANS receipt and NEC rates, though ANS receipt does lower overall neonatal mortality [26, 27]. More work is needed to assess the true relationship between antenatal steroid use and NEC severity, which is likely complex and multifactorial.
This study included neonates with cyanotic heart disease and patent ductus arteriosus (PDA) in its analyses. Cardiac NEC is suggested to be a distinct disease due to differences in initial severity, age at diagnosis, and prognoses between subjects with necrotizing enterocolitis with and without heart disease [28]. Thus, it was necessary to assess for any differences in neonatal cardiac anomalies between the medical and surgical NEC groups. There was no significant difference in cyanotic heart disease (8.3% in medical NEC, 6.0% in surgical NEC, p = 0.53) or PDA (45.1% in medical NEC, 51.8% in surgical NEC, p = 0.34) between the two outcome groups (see Table 1). This suggests that cardiac NEC within this cohort did correlate with the outcome of surgery or death. Additionally, as rates are highly similar between the two groups, cardiac NEC is unlikely to have influenced other differences seen between outcome groups. The study is however limited in that it did not distinguish between cardiac and non-cardiac NEC, and so cannot draw conclusions about whether the demographic, laboratory, clinical, or nutrition factors discussed are more specific to one subtype of NEC or the other.
Additional limitations of this study include the fact that CRP in the surgical group may be confounded by the surgery itself; i.e. some of the elevated CRP levels occurring within 72 h post-diagnosis in the surgical group occurred following neonatal surgery and therefore could be a result of the operation itself rather than an indicator of disease severity. However, of the 36 surgical NEC cases that exhibited a CRP value above 0.07 mg/dL (above the upper limit of normal), only 8 of these cases had CRP values included in this study which occurred following surgical intervention, and four of the eight had already displayed high (significantly >0.07 mg/dL) CRP levels before any surgical intervention. Overall, the influence of surgical intervention on CRP data is unlikely to have affected overall data trends but should be accounted for when applying this finding to clinical practice.
This study’s characterization of nutrition using the single most recent feed before NEC diagnosis also presents a limitation, as this method provides only a snapshot of nutrition status and may not be wholly reflective of the neonate’s diet. For example, the infant may have been receiving maternal milk for several weeks but was supplemented with a donor milk feed as their last feed before NEC diagnosis, and so was categorized as a “donor milk” case in our study. Future research assessing a wider data set of feedings for each neonate is required to assess the validity of the data presented here.
Additionally, thrombocytopenia, one of the significant markers of progression to surgery/death in this study, is included as a sign in the modified Bell Staging criteria for NEC. As the modified Bell staging criteria are known and used widely, the presence of this laboratory anomaly included in the Bell criteria may have influenced clinicians’ decisions for surgical management, confounding the association between thrombocytopenia and surgical NEC. Finally, this study does not account for populations without a diagnosis of NEC, so the risk factors described are limited by this perspective. However, as this research corroborated well-studied associations relating NEC to elevated CRP, decreasing platelet count, and lower maternal milk intake, there is established validity to the findings. The study only accounts for associations between risk factors and NEC outcomes and does not conclude causal relationships.
In summary, elevated CRP, low platelets, positive blood culture results, and the need for inotropic medication or vasopressors within 24 h of NEC diagnosis are significantly associated with progression to NEC-related surgery or death. Few maternal or demographic markers predicted the risk of surgical vs. medical NEC beyond birth weight and gestational age. Neonates receiving fortified human milk showed lower rates of NEC-related surgery or death; surgery and death rates were lowest among neonates receiving fortified, maternal milk compared to all other nutrition types. Increased abdominal circumference at birth is a potential early marker of increased risk for severe NEC. Further investigation is warranted to clarify the association between antenatal steroid receipt and NEC severity and to determine the utility above markers in clinical practice.

留言 (0)