The relationship between sickle cell disease and hearing loss has been clearly documented (between 12 and 66% among individuals with sickle cell disease), and most of the cases have progressive bilateral hearing loss (progressive cochlear damage by hypoxia stemming from the sickle shape of the red cells) [1].
Sickle cell disease is also recognized as a contributing factor to sudden SNHL, with a reported incidence of 2.2% among pediatric cases [2, 3]. In cases of sudden bilateral sensorineural hearing loss, expeditious cochlear implantation is advocated in sickle cell patients, owing to the heightened risk of precipitous cochlear sclerosis [4]. In the general population, the etiologies of sudden SNHL are markedly heterogeneous and frequently elusive; idiopathic sudden sensorineural hearing loss is the predominant diagnosis [5,6,7]. In individuals with sickle cell disease, sudden SNHL is predominantly attributed to vaso-occlusive crises. As early as the 1970s, Berry reported the presence of sensorineural hearing loss in sickle cell patients, noting that hearing loss in the high frequencies may quite possibly be related to cochlear thrombosis in microcirculations [8].
Regarding the patient in question, it is substantiated that the individual experienced a vaso-occlusive crisis, which is further corroborated by the occurrence of a concomitant frontal cerebral infarction. The crisis likely involved the common cochlear artery, which supplies the cochlea and the posterior semicircular canal [7, 9].
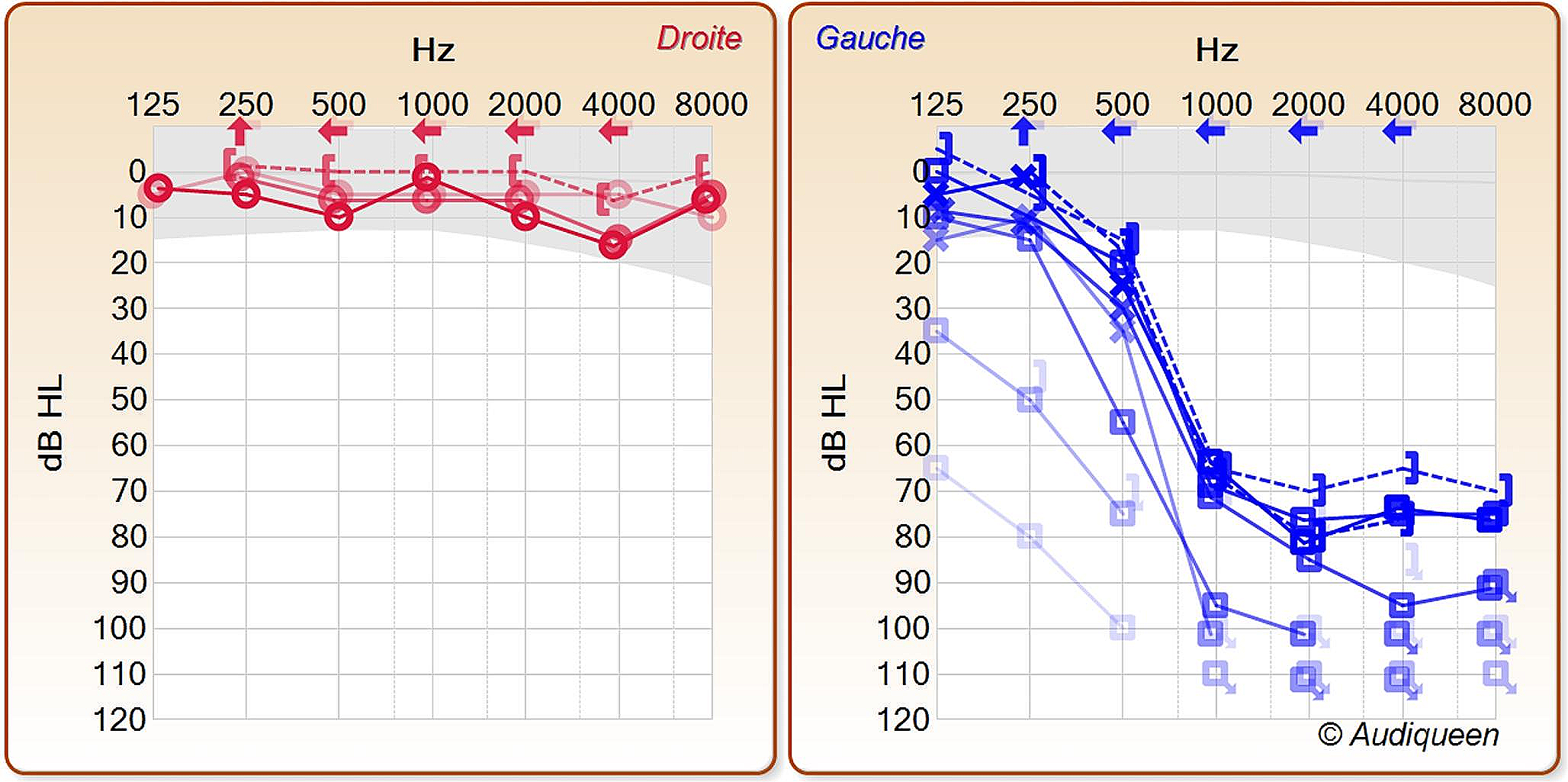
This assertion is supported by clinical instrumental findings, including auditory impairment in PTA and isolated dysfunction of the posterior semicircular canal as assessed by vHIT, and by radiological (MRI) evidence indicating the involvement of the posterior semicircular canal and cochlea.
Furthermore, the utilization of delayed post-contrast MRI of the inner ear using 3D FLAIR HR sequences is being refined for the in vivo delineation of endolymphatic and perilymphatic fluids [10]. This diagnostic modality has demonstrated utility in the diagnosis of hydropic ear diseases [11, 12] and their auditory sequelae, albeit certain images may present interpretative challenges.
In emergency presentations of sudden SNHL with a strong suspicion of vascular etiology, this imaging technique permits the in vivo examination of inner ear fluids during the crisis. This could provide invaluable insights into the pathophysiological underpinnings of sudden SNHL and its etiological assessment.
In the present case, the clinical-radiological congruence is particularly evident, reinforcing the notion that delayed post-contrast MRI with 3D FLAIR HR sequence is capable of illustrationg the repercussions of localized arterial occlusion within the inner ear. Additionally, Eliezer et al. have documented an analogous presentation in a 60-year-old female patient with rheumatoid arthritis [13]. This case is differentiated by the hematologic pathology of the subject, bolstering the vascular etiology for what they have termed “Cochleovestibular artery syndrome”.
The absence of vertigo reported by the patient can be explained by the limited involvement of the posterior labyrinth (only the posterior semicircular canal), the lower gain of the posterior semicircular canal compared to the lateral canal, its non-alignment with the axis of head rotation, and the patient’s focus on his hearing loss which may have led to overlooking any added sensation of vertigo.
The right horizontal vibratory nystagmus indicates vestibular asymmetry affecting the left labyrinth. Despite no evidence of lateral canal involvement at high frequencies (vHIT), it may exist at very high frequencies (vibration-induced nystagmus). Cochlear ischemia also explain vestibular asymmetry by impairing the blood-labyrinth barrier and the stria vascularis, disrupting the endolymph (ionic, pressure, potential) balance, which affects all labyrinthine structures [14, 15].




留言 (0)