In the SGSG-012/GOTIC-004/Intergroup study, 47% of the patients with recurrent endometrial cancer responded to the re-administration of platinum-based therapy. Among these responders, the DSPR exceeded the PFI in 31% of the patients. In particular, the DSPR exceeded 12 months in 39% of the cases. Furthermore, the DSPR lasted for ≥ 36 months in 6% of the cases. Thus, re-administration of platinum-based chemotherapy for recurrent endometrial cancer is expected to produce long-term effects in a significant number of patients.
Several studies have revealed that secondary responses to platinum-based chemotherapy in patients with recurrent ovarian cancer are highly dependent on PFI [1, 2, 8,9,10,11]. Second-line platinum-based regimens are expected to be effective in a longer period, the longer the PFI. A retrospective review by Markman et al. revealed that the DSPR rarely exceeded the PFI [7]. Only four (3%) out of 121 patients with assessable secondary responses had DSPR of longer duration than the prior response period in their study [7]. The SGSG-012/GOTIC-004/Intergroup study revealed that the PFI is a predictor of response and survival after second-line platinum-based chemotherapy in patients with recurrent endometrial as well as in ovarian cancers [4]. However, the DSPR exceeded the PFI in 40 (31%) of 130 patients with recurrent endometrial cancer. PFI may not determine DSPR as clearly in patients with recurrent endometrial cancer as in those with ovarian cancer. Endometrial cancer has a lower rate of homologous recombination deficiency compared with epithelial ovarian cancer. The mechanisms by which platinum drugs responded to may differ [12, 13]. As presented in Table 5, more than two-third of the patients whose DSPR exceeded the PFI received different first- and second-line chemotherapy regimens. However, differences in chemotherapy regimens administered at initial treatment and recurrence had no clear effect on the DSPR (Table 4).
We could not identify significant clinical factors that might have influenced the DSPR (Table 4). Although this study included many patients with a high-risk type of histology, such as carcinosarcoma and non-endometrioid, we did not find any effect of the histologic type on the DSPR. In addition, the regimen of chemotherapy administered did not have a clear effect on the DSPR. On the other hand, although there were only 9 patients with previous RT, they had very short DSPR, suggesting that RT might have had negative effects on the DSPR.
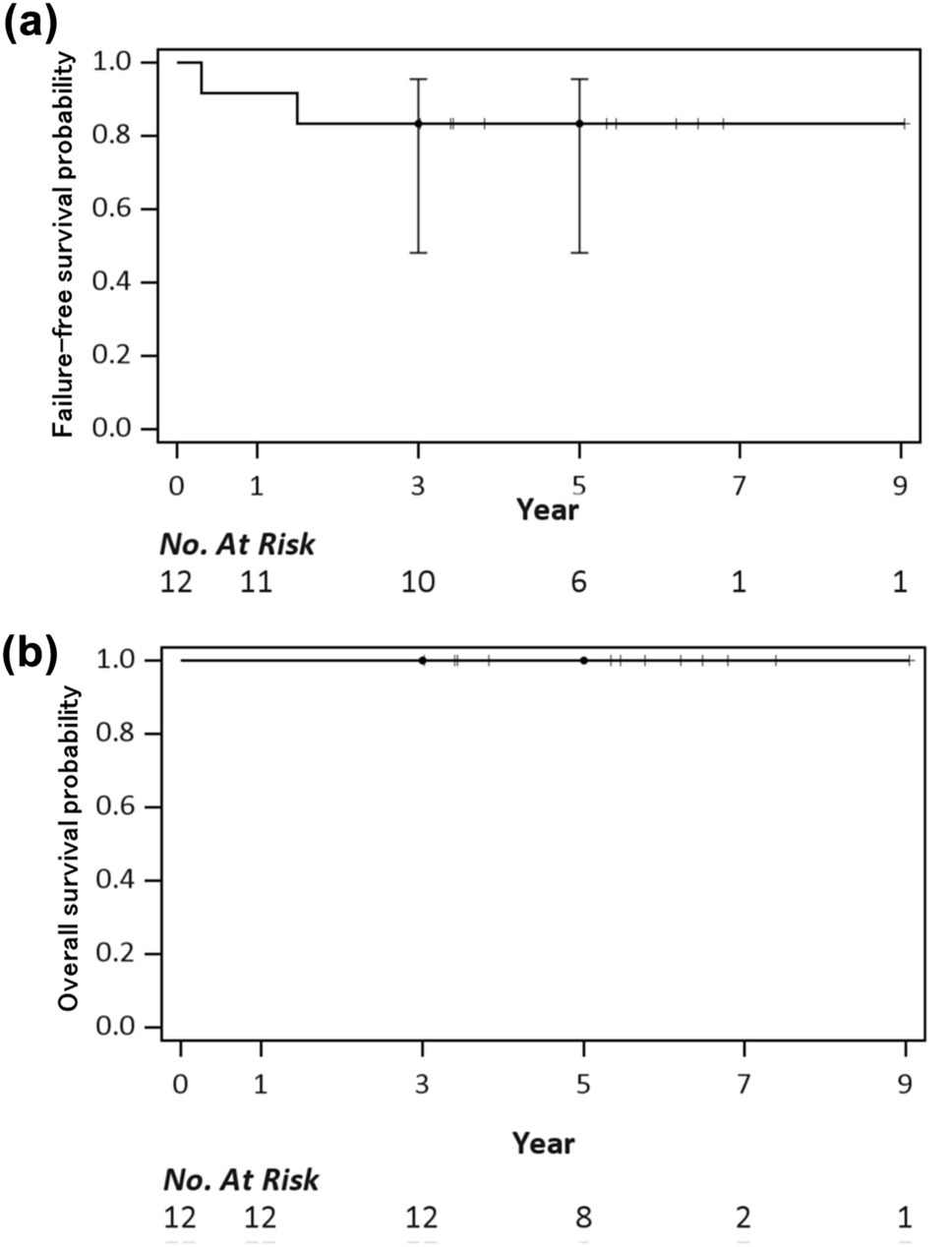
In the LEN/PEM group in the KEYNOTE-775 trial, responses were observed in 33.8% of patients. The median PFS period for whole patients was 7.3 months [6, 14]. Based on the shape of the PFS curve, it was estimated that slightly less than 20% of the patients would have very long-term recurrence-free survival. A certain number of patients are expected to have a very long survival period or cure with LEN/PEM. On the other hand, the shape of the survival curve of the DSPR (Fig. 1A) in our study reveals a flat tail. Re-administration of platinum-based chemotherapy can also result in very long survival or cure in slightly less than 20% of patients with recurrent endometrial cancers. In addition, as many as 39% of the patients had a response longer than 12 months, 6% of the patients had a response longer than 36 months. Similar to that with LEN/PEM, re-administration of platinum-based chemotherapy may afford very long-term survival in a certain number of patients.
The final analysis of the ENGOT-En9/LEAP-001 phase III randomized controlled study, which directly compared the efficacy and safety between LEN/PEM and paclitaxel and carboplatin combination therapy (TC) as a first-line chemotherapy for endometrial cancer, revealed that LEN/PEM did not significantly extend PFS or OS [15]. However, LEN/PEM prolonged PFS and OS in the subgroup of dMMR (the hazard ratios were 0.61 and 0.57, respectively). In addition, LEN/PEM significantly prolonged PFS and OS in patients with previous neoadjuvant/adjuvant chemotherapy (the hazard ratios were 0.52 and 0.64, respectively), which comprised approximately 15% of whole study participants. Unfortunately, the results by PFI in this study have not been disclosed. On the other hand, according to the real-world data from the US, there was no significant difference between the response to platinum-based chemotherapy and LEN/PEM re-administration in patients with recurrent endometrial cancer who had previously received platinum-based chemotherapy [16]. Patients with PFI ≤ 12 months had a 44.1% and 46.5% response to LEN/PEM and platinum-based chemotherapy, respectively; patients with PFI > 12 months had a 75.0% and 66.7% response, respectively. As observed in the ENGOT-En9/LEAP-001sudy, in patients with dMMR, LEN/PEM may offer longer survival than TC therapy, and there are no clear criteria for the re-administration of platinum-based chemotherapy for the treatment of recurrent endometrial cancer [15]. In future, it is expected that the criteria for treatment selection will be clarified by carefully collecting clinical information. The Japanese Gynecologic Oncology Group is currently collecting real-world data to clarify treatment strategies for recurrent endometrial cancer (JGOG2055s study: UMIN000050897).
This study has a few limitations. The patients in the SGSG-012/GOTIC-004/Intergroup study received treatment of recurrence between 2005 and 2009 [4]. Although the standard primary treatment of endometrial cancer has not changed, the social backgrounds of patients may differ. It cannot be denied that this could have had some influence on the treatment outcomes. In addition, the data collected in this study did not include the date of response confirmation; therefore, calculating the duration of the response was impossible. Therefore, the comparability with data from recent clinical trials, including those on immune checkpoint inhibitors, has decreased. Furthermore, data regarding the expression status of mismatch repair genes and microsatellite instability were not included. Although there are some problems, as described above, there is no other large-scale, properly cleaned dataset of patients with recurrent endometrial cancer who received platinum-based chemotherapy, which does not undermine the significance of this analysis.
Re-administration of platinum-based chemotherapy for recurrent endometrial cancer might result in a long-term response beyond the PFI. Even in the current situation where immune checkpoint inhibitors have been introduced for management, re-administration of platinum-based chemotherapy is worth considering.







留言 (0)