
記住我



We present the case of a 40-year-old female patient who visited our clinic complaining of slowly progressive paralysis of the right-sided facial muscles over the past 2.5 years, starting at the Mm. corrugator and orbicularis oculi, and progressing from the cranial to the caudal mimic muscles, finishing in complete facial palsy. The patient had no medical history and denied symptoms such as fever, night sweats or unintentional weight loss. Upon clinical examination, we observed a complete right-sided peripheral facial palsy (Fig. 1). All other otorhinolaryngological examination findings were within normal limits and blood tests showed unremarkable results.
Fig. 1
Patient; (left) before surgery with right-sided facial palsy, (right) after surgery 24 months after facial nerve reconstruction
Initially, magnetic resonance imaging (MRI) examination of the head and neck soft tissues (Fig. 2), computed tomography (CT) of the petrous bone and cranial base, as well as 18-fluorodeoxyglucose positron emission tomography-computed tomography (18-FDG PET-CT) (Fig. 3), were performed. They did not detect any cause for the peripheral facial palsy. There were no observable lesions, enlarged lymph nodes or pathological 18-FDG-uptake along the course of the peripheral facial nerve. The radiological examinations were evaluated by various highly experienced radiologists in the field of head and neck imaging at our certified head and neck tumor center.
Fig. 2
(a) MRI, T1, transversal; (b) MRI, T2, transversal. The right parotid gland shows even less parotid gland tissue then the left parotid gland. No lesions are depictable
Fig. 3
(a) 18-FDG PET-CT transversal; (b) 18-FDG PET-CT coronal; the right parotid gland shows even lower 18-FDG tracer uptake than the left side
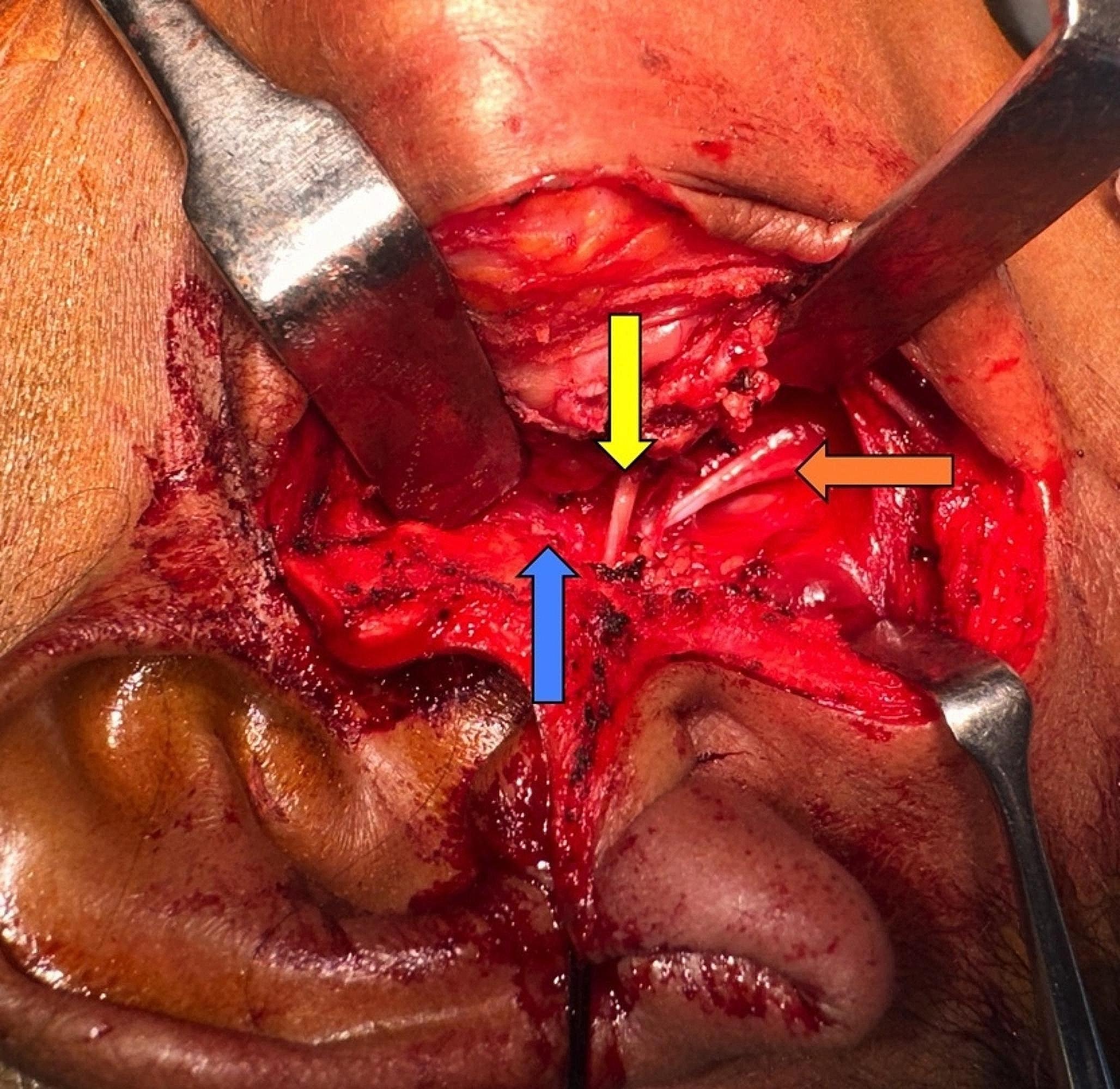
We decided to proceed with surgical exploration, which microscopically revealed no evidence of a tumor and an externally completely unremarkable facial nerve (Fig. 4). A biopsy from the main trunk area of the nerve close to its bifurcation revealed a perineural and intraneural infiltration by a p16-positive squamous cell carcinoma (Fig. 5). Following our interdisciplinary tumor board decision, a total parotidectomy with resection and reconstruction of the facial nerve using the diversification technique (auricularis magnus nerve interposition for the cranial facial nerve branches and hypoglossus-facial nerve jump anastomosis for the caudal facial nerve branches) and level II-III neck dissection were performed. After removal of the tumor-infiltrated main trunk, frozen sections were performed on the remaining nerve ends to ensure an R0 resection. Additionally, a platinum eyelid weight was implanted into the upper eyelid. The pathological examination revealed a moderately differentiated squamous cell carcinoma within the main trunk of the facial nerve without definite remnants of a primary tumor in the fully processed salivary gland (pT4a, pN0 (0/30), L0, V0, Pn1). Considering the absence of a primary tumor and other tumor formations in the otorhinolaryngological area, skin or other organs, the diagnosis of a completely regressive primary squamous cell carcinoma of the parotid gland was confirmed. Although adjuvant radiotherapy is usually performed in the case of malignant salivary gland tumor with perineural invasion, our interdisciplinary tumor board recommended a close follow-up care as an individual therapy plan due to the complete regression of the primary tumor and the sufficiently large safety margins. MRI of the soft tissues of the head and neck (after 3 months) and 18-FDG PET-CT (after 6 months) revealed no evidence of a primary tumor, locoregional lymph node involvement, distant metastases, or tumor recurrence. Whole-body CT (after 17 months) revealed no tumor regrowth or metastasis. Due to the immediate facial nerve reconstruction, the facial mimic recovered satisfactorily within 24 months, with complete eyelid closure and good facial tonus (Fig. 1).
Fig. 4
Main trunk of the facial nerve on the right in situ. Site of the biopsy (star). Biopsy was taken at the upper part of the bifurcation, as palsy started in the frontal mimic muscles
Fig. 5
Hematoxylin-eosin staining, perineural and intraneural tumor infiltration (arrows); (left) 400x magnification, (right) 200x magnification
留言 (0)