
記住我









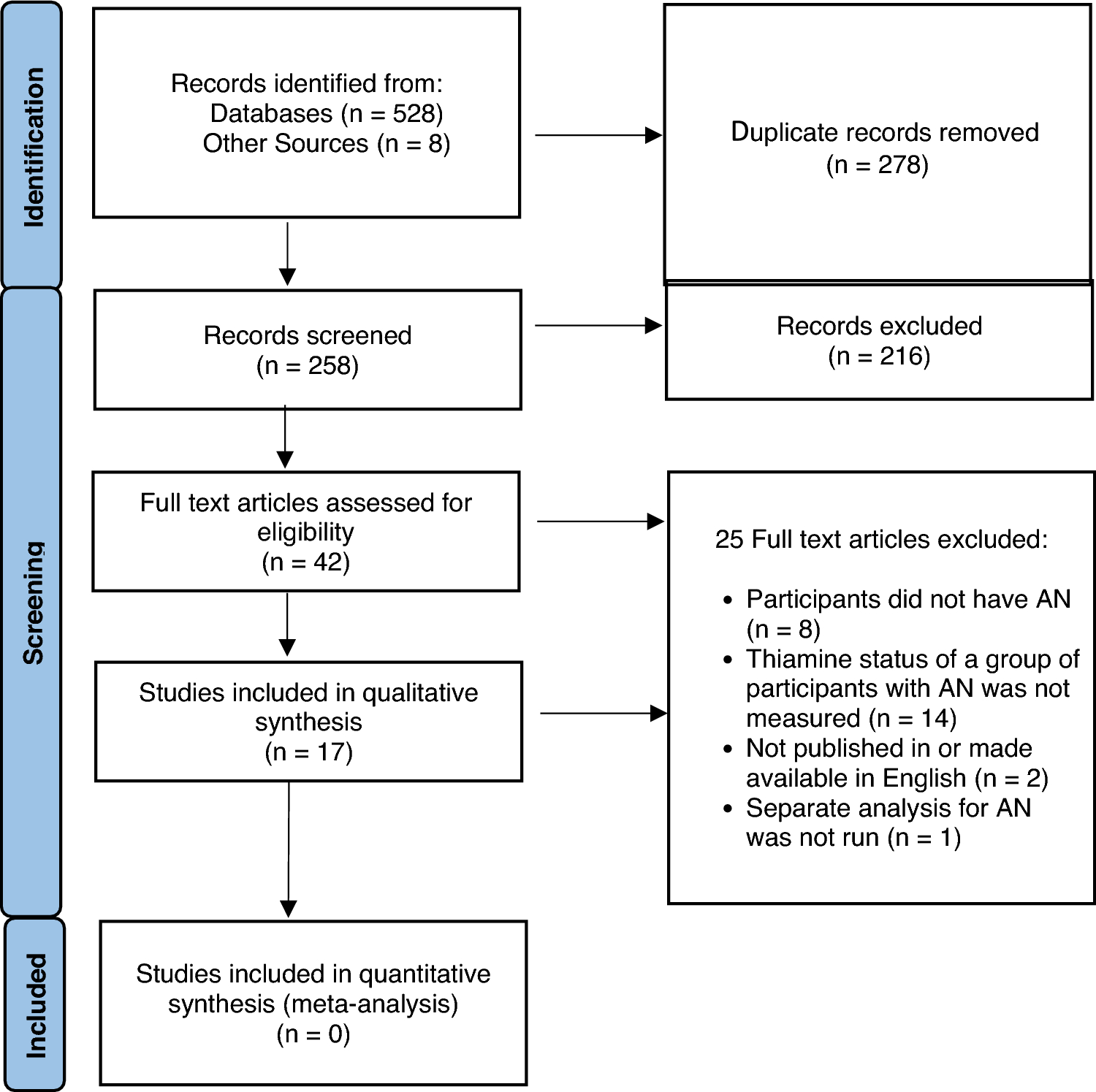
In total, 3961 articles were identified through database searching and 12 of these articles met the inclusion criteria. These 12 articles were therefore included in the review and provided information that could be extracted on the barriers and facilitators to help-seeking for mental health in adolescent boys and young men (Fig. 1).
Fig. 1
PRISMA flowchart of the study selection process
Types of included studiesSix of the studies included were conducted using qualitative methods, such as focus groups and semi-structured interviews, and five studies were conducted using quantitative methods, namely survey questionnaires. One included study used a mixed methods approach with both surveys and focus groups.
Study characteristicsA table of study characteristics (Table 1) was created using the following categories: study type, study author(s) and year, age range and mean age, sample size, country, study context, study methods and aim, type of analysis, key findings, and study implications. The number of study participants included across the 12 included studies totalled 4842 (M = 403.5; SD = 727.82). The average participant age in each study in this review was within the inclusion criteria of 14–22 years.
Table 1 Characteristics of selected studiesFour of the studies included were based in the UK, three were based in Australia, three were based in the USA and one was based in Ireland. One study was Australian based but included an international sample, with participants mostly from the USA, Australia, and the UK. The majority of the studies included in this review (7) took place in a school setting or university setting. Three studies took place in community-based settings, including sports clubs and clinics. One study took place within a youth service, and one used an online sample of self-reported video gamers.
Quality assessment of studiesThe six qualitative and one mixed methods studies were all listed as ‘valuable’ according to the CASP criteria, although three of these studies did not adequately report on reflexivity. For the five quantitative studies assessed using the NOS, one study was rated as Good, whereas the other four were rated as Fair. This was mainly due to issues around comparability and how well studies controlled for confounding variables. However, all quantitative studies rated highly in terms of selection and outcome quality (see Tables 2 and 3 for further details).
Table 2 CASP checklist for qualitative research summary tableTable 3 NOS for cross-sectional studiesThemes identifiedAnalysis of the 12 included articles identified five distinct themes related to barriers, facilitators, and general trends in adolescent boys and young men’s help-seeking. These are highlighted in Table 4 and discussed in detail below.
Table 4 Categories of themes identifiedTheme one: the impact of social normsPapers with this theme: 12 [22,23,24,25,26,27,28,29,30,31,32,33]The impact of social norms was identified as a key barrier to help-seeking. This can be further organised into two subthemes: conformity to masculine norms and self-stigma.
Subtheme one: conformity to masculine normsAll 12 papers identified conformity to masculine social norms (CMN) as a barrier to adolescent boys and young men’s help-seeking for mental health, often due to the stigmatisation of mental health difficulties being seen as a ‘weakness’ [22,23,24,25,26,27,28,29,30,31,32,33]. CMN can be defined as rigid adherence to stereotypical notions (both positive and negative) of masculinity posited by society [34, 35]. Adolescent boys and young men felt that seeking help was embarrassing as it contradicted traditional notions of masculinity, and that they should be able to deal with problems without professional help [26, 29, 32, 33]. CMN was therefore associated with more negative attitudes towards help-seeking, which can be seen by young men as a weak behaviour and, consequently, one to be avoided [29, 31]. For example, one participant in Clark et al.’s study [24] stated “Yeah, there’s a sort of stereotype of males…. if you are suffering from one of those [mental health problems] that you are weaker than everyone else” [24] (p. 230).
Cole and Ingram [25] examined the relationship between ‘gender role conflict’ (GRC) and help-seeking. GRC is defined by O’Neil [36] as “a psychological state in which socialized gender roles have negative consequences for the person or others” [36] (p. 362). Cole and Ingram found that GRC in young men led to increased avoidant behaviour and decreased use of social support for mental health concerns, however GRC did not have an impact on seeking professional psychological support. GRC was also found to be a key factor in the gendered differences of help-seeking, which is in parallel with the findings of Sagar-Ouriaghli et al. [32] around traditional masculine stereotypes.
Masculine norms were also found to be a specific barrier for young Black men in the UK in Meechan et al.’s [30] paper. This study focused on the intersections of race and masculinity on help-seeking behaviour and found that Black men felt social pressure to be strong and to cope independently. Interestingly, all participants in this study identified mental strength as a key traditional trait for Black men in the UK and understood seeking help for mental health in the “cultural context of generations of African Caribbean men needing to be strong to overcome racism” [30] (p. 7). Participants also discussed this in comparison to white males, noting that “the notion of masculinity and strength was more pronounced within Black male communities” [30] (p. 4). CMN may therefore present differently for white and non-white ethnic groups.
Subtheme two: self-stigmaCMN is closely linked to the subtheme of self-stigma. All 12 papers acknowledged stigma or stigmatising attitudes towards mental health [22,23,24,25,26,27,28,29,30,31,32,33]. Cole and Ingram [25] define self-stigma as “the belief that one is inadequate or weak, if he wants to seek professional help” [25] (p. 442). Adolescent boys and young men may view help-seeking as a personal failure, as they have been unable to solve the problem themselves. The specific relationship between masculine norm adherence and self-stigma was highlighted by several studies, with men who endorse greater masculine norms experiencing higher levels of self-stigma [25, 27, 31]. Cole and Ingram [25] reported that men who experience higher levels of self-stigma are less likely to seek informal help from friends, family, and peers. They also found that these men were more likely to practice avoidant behaviours, which may help to explain comorbidity of substance abuse disorders in this age group [25].
Heath et al. [27] identified self-stigma as a barrier for adolescent boys and young men that is consistently associated with lower help seeking intentions. Heath et al. [27] used a self-stigma scale to measure the relationship between this and professional help-seeking in participants and found that self-stigma was positively related to self-disclosure risks. Meechan et al. [30] found that stigma within Black communities influenced young men’s identities, and that generational stigma was passed down through families and served as a barrier for help-seeking within this community, which is similar to Burke et al.’s [23] findings on generational stigma. Ellis et al. [26] found that some participants identified facing self-denial in addition to self-stigma and acknowledged that whilst mental health difficulties were not a sign of weakness, they felt it was when it related to them personally. One young man stated, for example “…I guess there’s still a stigma of mental health being a weakness… I realise that it’s not but it’s just something that I’d find difficult coming to terms with” [26] (p. 6).
Theme two: limited availability of information about mental health and help-seekingPapers with this theme: 6 [24, 28,29,30, 32, 33]Limited availability of information about common mental health disorders, especially anxiety, was also found to be a barrier to help-seeking amongst adolescent boys and young men. Within Meechan et al.’s [30] paper, some participants discussed how they view mental health as a disability and as something that cannot be recovered from, suggesting that they were not well-informed about the causes of or treatments for mental health problems. Clark et al. [24] identified a similar theme, where participants felt that they and their peers did not have the understanding that anxiety was a condition that could be treated or did not know how effective anxiety treatment would be for them. A perception of anxiety as “not a real illness” was also discussed [24] (p. 230). Further to this, it was found by Clark et al. [24] that participants held the belief that parents and teachers would also lack knowledge of mental health conditions such as anxiety, and therefore would not be able to offer help or support to adolescent boys and young men. Likewise, a lack of knowing where to go to get help served as a barrier, as well as fear of being prescribed medication from a health professional if they were to divulge mental health concerns [24, 29].
Sagar-Ouriaghli et al. [32] reported participants identified difficulty in assessing the severity of symptoms for anxiety and/or depression, and subsequently, when these would require professional intervention. This is reflected by one participant who shared that for them “the difficult part was thinking, convincing myself I need help” [32] (p. 7). Having limited awareness of common mental health conditions, and not understanding information when it was available, was also acknowledged by participants across several studies [28, 32, 33].
Some participants reported that limited mental health information meant they saw mental health conditions as ‘secret’ problems. In Clark et al. [24], participants considered mental health to be a hidden concern, while in Meechan et al. [30], mental health was seen as something that adolescent boys and young men could hide from others.
Theme three: “male-friendly” campaigns to promote interventions or mental health literacyPapers with this theme: 5 [23, 24, 29, 30, 32]Creating ‘male-friendly’ mental-health campaigns and promoting literacy was identified as a key facilitator for adolescent boys and young men amongst five studies, as a way of increasing the availability of information on mental health [23, 24, 29, 30, 32]. Expanding on the previous theme, using ‘simple’ or lay terms to explain mental health conditions can be seen as a facilitator to help-seeking. Additionally, transparency about psychological information and general service information was a facilitator to help-seeking. Clark et al. [24] highlight how mental health literacy campaigns could explain more clearly the severity of anxiety but also the treatability of the condition. Interestingly, some participants identified the importance of not emphasising mental health related words in interventions or support, with a focus group participant in one study stating “if you’re struggling with depression and what not as a man, let’s be real are you going to go to this workshop talking about men’s mental health? Probably not” [32] (p. 8).
Lynch et al. [29] identified the need for young men to be invol
留言 (0)