
記住我


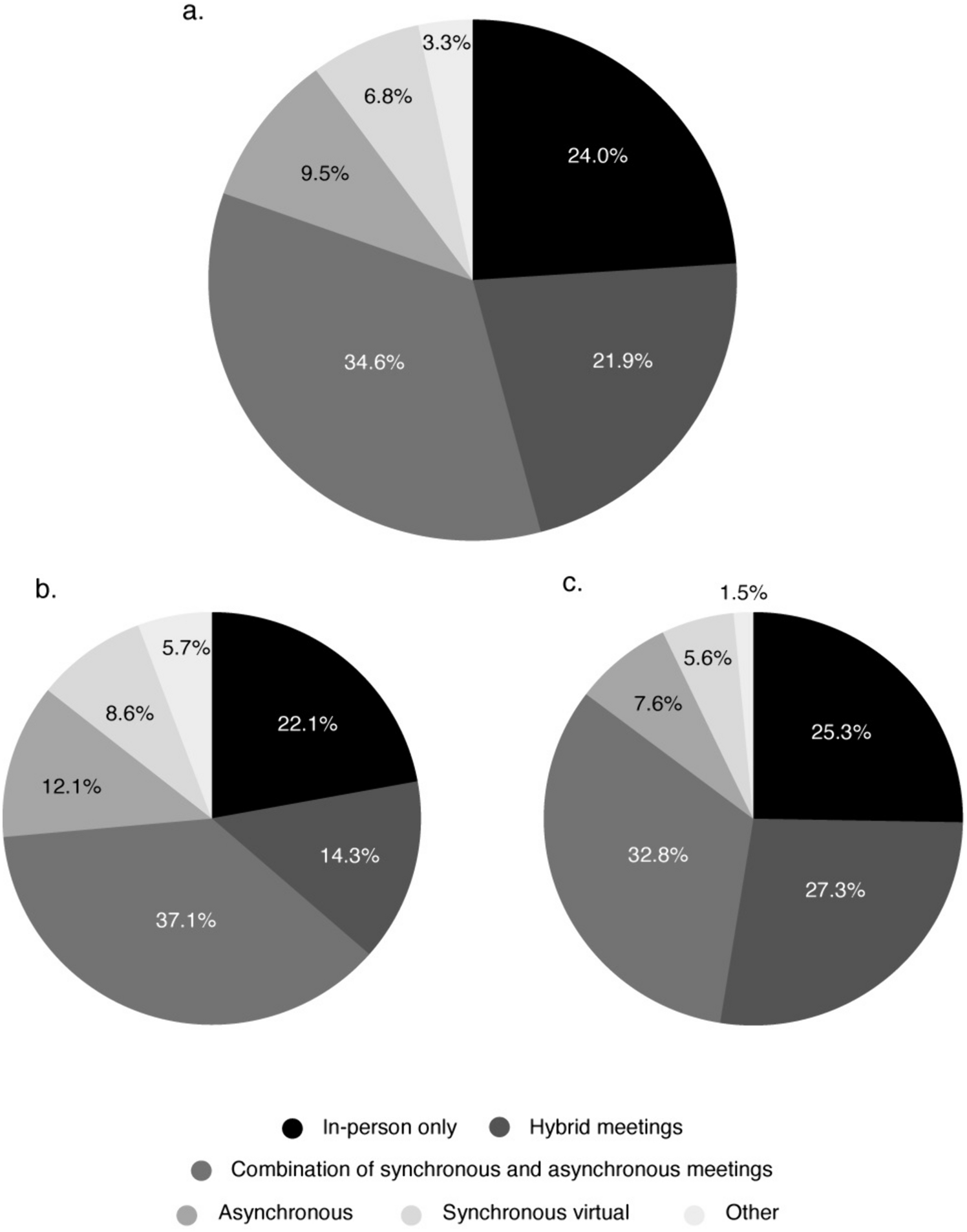


The finding that 76% of the surveyed HCPs prefer virtual or hybrid pharmaceutical meetings over in-person–only meetings is in line with other recent reports on medical and scientific conferences. For example, Laohawetwanit et al. found that, among 562 pathologists from 79 countries, 80.1% (n = 450) preferred hybrid or virtual over in-person meetings [4]. Kays et al. likewise reported that 87% of 70 surveyed women physicians wanted an option for virtual attendance at conferences [5]. Our short survey showed that the preference for hybrid meetings among HCPs almost doubled between 2022 and 2023, while the preference for in-person–only meetings remained relatively flat. This adds to the existing evidence and suggests that HCPs still enjoy meeting in person but now expect the convenience of virtual.
In terms of the optimal meeting frequency, most respondents suggested 2–3 times per year, followed by quarterly, every 2 months, and monthly. Very few respondents wanted longer durations between meetings (i.e., every 9–12 months). As such, while the optimal meeting frequency and timing will vary on a case-by-case basis, organizers should consider engaging their KOLs and HCP stakeholders at least three times a year to cater to the majority.
The usefulness of regular and ongoing advisory board meetings is further supported by the finding that the vast majority of advisors (88.2%) would like to receive updates from the pharmaceutical team sponsoring the meeting on how the insights collected are being used. This indicates that HCPs and KOLs strongly prefer—or even expect—ongoing collaboration and communication from pharma.
4.2 Benefits of Virtual Pharmaceutical Meetings4.2.1 Convenience and FlexibilityConvenience has been previously reported as a key benefit of virtual/hybrid meetings and conferences [4]. With the majority of US health care workers in 2022 belonging to the 25- to 34- and 35- to 44-year age groups [6], one can speculate that many have young children and/or older relatives requiring caregiving. Caregiving responsibilities often fall on women; 85.3% of women physicians participating in the pilot study by Kays et al. reported experiencing challenges with attending conferences in person. The most commonly cited challenges included childcare difficulties (66.7%) and work-life balance issues (65.1%) [5]. In addition, many HCPs work in busy clinics and may be dealing with long backlogs of appointments or surgeries stemming from the COVID-19 pandemic (see for example [7, 8]). As a result, once they have experienced alternative ways of participating in advisory boards and other pharma-sponsored events, they may be less willing to travel long distances and stay in a hotel for one or more nights to attend an all-day in-person meeting.
Based on the above, offering participants the option to attend in-person meetings remotely (virtually) should be made standard across the industry, at a minimum whenever traveling is involved. Depending on the HCP advisors’ preferences, meeting organizers may want to consider a mix of live (hybrid or synchronous virtual) and asynchronous meetings over time to maximize flexibility and allow HCPs to contribute on their own time.
4.2.2 Environmental ImpactSarabipour et al. reported that flying to attend scientific meetings can produce air-travel-related CO2 emissions comparable to, or higher than, the annual per capita emissions in many countries [9]. However, in-person meetings come with a substantial environmental footprint from not only flights and ground transportation but also the accommodation and meeting venue, catering and food transportation, audiovisual equipment, printed materials, and waste generation. Skiles et al. conducted a quantitative analysis comparing in-person and virtual conferences before and after the COVID-19 pandemic; the authors found that the cumulative carbon footprint of the total attendees to three virtual conferences in 2020 (1.07 t CO2e for >7000 participants) was comparable to the average footprint of a single attendee at an in-person conference the year before [10]. In 2013, Achten et al. [11] found that conference attendance was responsible for 35% of scientists’ carbon footprint and that virtual meeting technologies such as videoconferencing tools could reduce their climate change impact by up to 44%. Likewise, Tao et al. [12] reported that transitioning from in-person to virtual conferencing can substantially reduce the carbon footprint and energy use of the meeting by 94% and 90%, respectively. These results are corroborated by a recent study by Gattrell et al. [13], who reported that travel accounts for 91–96% of total emissions of in-person medical conferences, mainly through long-distance and business-class air travel. In comparison, the authors found that the carbon emissions associated with virtual attendance represent only 0.3–1.1% of in-person attendance emissions. In fact, the carbon cost of attending an entire virtual congress was found to be lower than taking taxis to and from the airport and between the hotel and the congress venue [13].
At a time when climate change is no longer a distant threat but an everyday reality impacting numerous aspects of our lives, including both our physical and mental health [14], the environmental impact of meetings must be a key consideration for organizers when choosing the format. If going virtual is not an option, hosting in-person advisory board meetings in conjunction with large conferences that the advisors are already scheduled to attend, opting for regional and/or hybrid meetings, and introducing “carbon budgets” [13] are some strategies that may help reduce the associated carbon footprint.
Another factor to consider when choosing between virtual, hybrid, and in-person meetings is the effects of climate change in terms of more frequent extreme weather events; these events are known to be unpredictable and cause flight and transport disruptions with little to no notice [15]. Thus, if a meeting requires participants to fly or drive long distances, organizers need to always have a contingency plan in place. To this end, making live meetings hybrid by default provides a backup plan while providing superior flexibility and convenience for those who prefer to attend virtually.
Moreover, many pharmaceutical companies have set ambitious carbon-neutral or negative goals, and virtual meetings are one important tool in their toolbox to help them achieve these goals.
4.2.3 Diversity, Equity, and InclusionVirtual meetings, particularly if they contain an asynchronous component, promote DEI in a variety of ways. They effectively overcome geographical and cost barriers, and allow participants from remote, underserved, or low-income communities to participate more easily [9, 10, 16,17,18]. Time zone differences can be an obstacle to inclusive international meetings if real-time attendance is expected. By leveraging asynchronous meeting tools, differences in time zones and scheduling conflicts become non-issues [18]. Further, the virtual format closes the gender gap in terms of attendance rates. In the analysis by Skiles et al., attendance by women increased between 60 and 260% when conferences previously held in person turned virtual at the start of the COVID-19 pandemic [10].
In the context of pharmaceutical advisory boards, the virtual format facilitates multidisciplinary input by extending the reach beyond KOLs and specialist physicians to include other health care stakeholders such as nurses, pharmacists, community and allied health care providers, and even patients. In an asynchronous environment, advisors who may be hesitant to speak up in live settings, including junior HCPs, neurodivergent individuals, introverts, or people who speak English as a second language, are able to contribute equally to their counterparts, resulting in more representative insights.
4.3 Potential Downsides of Virtual MeetingsDespite the overwhelming advantages of virtual and hybrid meetings, there are potential issues that should be mentioned and considered when choosing between meeting formats (Fig. 4). These include a lack of face-to-face networking opportunities, lack of reliable internet connections in remote areas or low-income communities, and the risk of videoconferencing fatigue (“Zoom fatigue”) [4, 19, 20]. Of note, our survey results suggest that synchronous virtual (web meeting) is the least popular meeting format among HCPs when used as the only meeting format (i.e., without an asynchronous component) (Fig. 1). This supports the theory of videoconferencing fatigue and underscores the importance of moving away from one-size-fits-all cookie-cutter web meetings. Moreover, for hybrid meetings, there is a risk of virtual attendees receiving an inferior experience compared to in-person attendees.
Fig. 4
Suggested advantages and disadvantages of in-person, hybrid, synchronous virtual, and asynchronous pharmaceutical advisory board meetings. Advantages (pros) are shown on the left, with disadvantages (cons) on the right. Each meeting format has unique pros and cons, with a decreasing number of disadvantages seen when moving from in-person and hybrid meetings to synchronous virtual and asynchronous activities
To counter the above challenges, Doran et al. [20] highlighted the need for proactive discussion (e.g., between organizers and supporting vendors) and consideration of accessibility during the pre-event, event, and post-event planning stages. That is to say, there are ways to mitigate these issues, including by strategically using a mix of hybrid, synchronous virtual, and asynchronous meetings designed to offer “the best of both worlds.” For hybrid meetings, careful planning is required to ensure that virtual attendees receive a comparable experience to those attending in person. This should include innovative ways of having remote and on-site participants interact with each other during workshops, along with behind-the-scenes support for, and monitoring of, virtual attendees to ensure that they are continuously engaged and able to share their thoughts.
4.4 Study LimitationsThe current study has a number of limitations. First, it is based on preliminary data from a relatively small sample (n = 443). Second, all HCPs surveyed were participants in asynchronous meetings. Their recent experiences with this format may have skewed the data, and surveys for HCPs participating in synchronous virtual, hybrid, and in-person–only meetings should also be conducted. Third, we did not ask questions about the downsides of the various meeting formats or the benefits of in-person/hybrid meetings; the discussion around these was based solely on the published literature. Future studies featuring more specific survey questions, including questions on the downsides of different meeting formats and comparing different meeting durations, would be informative. Fourth, while rare, some participants selected ‘other’ but did not specify what exactly ‘other’ meant to them; in future surveys, providing an explanation if this option is selected should be made mandatory. Fifth, if an HCP participated in more than one asynchronous activity during the study period, it is possible that they answered the same question more than once, although most pharmaceutical organizers chose to include different questions each time. Last, we did not collect demographic data. In the future, it would be interesting to conduct a similar study assessing whether the responses differ between meeting participants from different geographies and according to age, sex, or race.
留言 (0)