We studied the necroptosis-related plasma markers MLKL, RIPK1, RIPK3, IL-33, and sST2 and the proinflammatory cytokines IL-6, TNF, and IL-1β with respect to the severity of acute pancreatitis (AP) in the early and late phase of the disease (< 72 h and 1 week from onset of symptoms, respectively). The results show that early sST2 and IL-6 levels predicted the development of severe AP (SAP) and were higher in both mild AP (MAP) and early and late severe AP (SAP) than in healthy controls (HC). RIPK3 levels were higher than in HC in the patients who had or would later have SAP. Further, MLKL levels were associated with the presence of organ failure (OF), particularly in the late phase, but were also higher in MAP than in HC. MLKL, RIPK3, IL-33, sST2, IL-6, TNF, and IL-1β levels were associated with at least one of the severity scores studied (APACHEII and SOFA).
sST2 and IL-33
Our finding that the levels of the IL-33 decoy receptor sST2 are associated with the development of SAP is in agreement with previously described associations between sST2 and diseases with a marked tissue damage component such as sepsis and heart failure [17, 30, 31]. In our results, sST2 levels also correlated with both disease severity scores determined, and furthermore, with hemoglobin and hematocrit, which may suggest a failure in vascular permeability. Apparently, one crucial mechanism behind the disadvantageous effects of sST2 is that by binding to IL-33 it prevents the effects mediated via the cell-surface IL-33 receptor ST2, e.g., survival and proliferation of basophils, mast cells, Tregs, and Th2 cells and secretion of Th2 cytokines (IL-4, IL-5, IL-10, IL-13). When the release of anti-inflammatory cytokines is reduced, the response is modulated in the direction of Th1 activation, including release of proinflammatory cytokines [5].
In one of the few studies conducted on sST2 in AP, the levels of sST2 were increased early during AP, correlated with parameters of severity, and decreased to near-normal range 30 days after the acute episode [19]. This seems to be in line with our current findings regarding the kinetics, as the sST2 levels were somewhat lower in late SAP than in early SAP, although not (yet) reaching the levels of HC. Interestingly, the sST2 levels of patients with early MAP were lower than in those with early SAP with persistent OF but also lower than in those who developed persistent OF only after sampling. Hence, sST2 appears to be a candidate for an early predictor of AP severity.
IL-33 levels showed broad variation among both AP patients and HC, and the levels of the patients did not significantly differ from those of HC. Considering that IL-33 is mainly produced in cells exposed to the environment, such as epithelial and endothelial cells, the possibility remains that it is continuously released by minimal surface damage, low-level inflammation, or low-level necroptosis/necrosis for various reasons also in healthy individuals. Moreover, it is noteworthy that IL-33 has been reported to be upregulated in the tumor microenvironment of pancreatic adenocarcinoma and lesions from chronic pancreatitis [32, 33]. Hence, systemic IL-33 levels in these diseases may also be more prominent than in AP.
Proinflammatory Cytokines
Interestingly, IL-6 and sST2 showed a similar pattern according to AP severity so that plasma level of either of these, determined < 72 h of symptom onset, was significantly lower in HC and MAP than in early SAP even when OF developed after blood sampling in patients with SAP. The potential of IL-6 as an early predictor of OF is well known, but the IL-6 assay has been considered expensive and complex for routine clinical practice [20]. However, nowadays an automated, rapid assay is available and has been studied for predicting complications in AP [34]. Our results also show that both IL-6 and sST2 peak in early SAP and tend to decrease towards late SAP, further emphasizing the potential of these markers in the early phase of AP. Further research aiming at developing more fluent clinical use of IL-6 and sST2 determination in the early phase of AP seems to be a rational approach for managing the disease.
Levels of sST2 were strongly correlated to those of IL-6 and IL-1β. Correlation between sST2 and IL-6 levels has been described recently in metabolic syndrome, and high circulating sST2 levels can be seen to mirror high inflammatory burden [35]. In different cell types, sST2 has been observed to enhance the secretion of IL-6 and IL-1β [36] but also to be produced in response to these [22]. Unfortunately, owing to the generally low levels of IL-1β and especially TNF in the current study, interpretation of the results concerning them is dubious.
RIPK1 and RIPK3
We observed that, as compared with HC, plasma RIPK3 levels were higher in late and early SAP also in those patients with early SAP who did not yet have persistent OF at blood sampling. The levels in MAP were a bit lower than in SAP, but the difference did not reach statistical significance. Hence, whether a significant difference between RIPK3 levels in early MAP and early SAP would emerge in larger studies, i.e., whether RIPK3 levels possess prognostic value in AP, remains to be elucidated. Recently, summarized results from several cohorts showed that RIPK3 levels in the plasma of patients admitted to intensive care for sepsis or septic shock are associated with in-hospital mortality and OF [13]. RIPK3 concentrations have also been found to be associated with the stage of acute kidney injury among critically ill trauma patients [14]. Furthermore, transcriptome analysis of leukocytes of patients with community-acquired pneumonia in intensive care revealed that higher mortality was associated with a subgroup of patients with high expression of RIPK3 (and other genes) [37]. These findings agree with our RIPK3 results, allowing us to conclude that high systemic RIPK3 levels represent a nonspecific sign of disease severity in several critical illnesses.
RIPK1 levels fell below the smallest standard concentration in almost all samples studied. Unfortunately, and for reasons unknown to us, the manufacturer changed the range of the RIPK1 ELISA kit from 15.6–1000 pg/ml (comparable to that of RIPK3 kit) to 0.156–10 ng/ml after our order was already placed. Therefore, it is not possible to make conclusions about the biomarker potential of plasma RIPK1 based on the current study, and reassessment with a more sensitive assay remains a topic for further research.
MLKL
Plasma MLKL levels were associated with the presence of OF and were at their highest in late SAP. The result is parallel to the finding that serum MLKL correlates with surrogate markers of OF such as serum lactate levels [15]. Our results also reinforce the view obtained from an animal model that OF, or multiple organ dysfunction syndrome, is characterized by necroptosis rather than apoptosis [12]. As the MLKL levels in MAP and early SAP before the development of persistent OF were very similar in our results, it seems unlikely that MLKL could serve as a marker predicting AP severity. It is also noteworthy that MLKL levels in early MAP were slightly but nevertheless significantly higher than in HC, which may reflect ongoing necroptosis in the pancreas also in the mild disease form.
To interpret the differences between the results concerning RIPK3 and MLKL, it should be noted that RIPK3 acts on other pathways besides necroptosis. RIPK3 can promote caspase-8-dependent apoptosis independent of its kinase function. Also, RIPK3 is a cell type-specific NF-κB activator, and it functions in mitochondrial production of reactive oxygen species, inflammasome activation, and subsequent release of IL-1β [38]. Hence, it can be expected that high systemic RIPK3 levels reflect a vigorous proinflammatory phase of systemic inflammation, whereas MLKL, as the terminal mediator of necroptosis, confirms the occurrence of necroptosis.
Importantly, in a rodent model of SAP, inhibition of necroptosis with the RIPK1-specific inhibitor necrostatin-1 (Nec-1) could reduce disease severity even when administrated after the establishment of SAP, thus making necroptosis a potential therapeutic target in AP [6]. Also, inhibition of necroptosis using the MLKL inhibitor necrosulfonamide (NSA) has been reported to alleviate, for instance, lung ischemia–reperfusion injury in mice [27]. In view of necrotizing pancreatitis being associated with increased sST2 levels [19] and infection of necrotized pancreas being quite common [4], it is also notable that IL-33 promotes neutrophil migration to the infectious site, which is crucial for host defence. For example, septic mice that were given an IL-33 injection showed significantly reduced mortality [30]. However, chronic pancreatitis has recently been described as an IL-33-dependent inflammation [33]. Hence, it is dubious whether targeting the IL-33/sST2 axis could be as promising as necroptosis inhibition as a future treatment option for AP.
Intravenous fluid resuscitation is the cornerstone of therapy strategies for SAP, but it is probable that aggressive fluid resuscitation (AFR) will aggravate other organ injuries while rapidly correcting the shock state. Interestingly, a recent study on rats showed that Nec-1, when administered before AFR, could reduce iatrogenic gut injuries, suggesting that necroptosis is an important mechanism in AFR-related intestinal barrier injury [39]. NSA was also able to protect against damage of intestinal epithelial cells in a mouse model [26]. Based on these results, it is conceivable that inhibiting necroptosis would be advantageous not only for reducing AP severity but also for counteracting treatment-associated damage.
Limitations of the Study
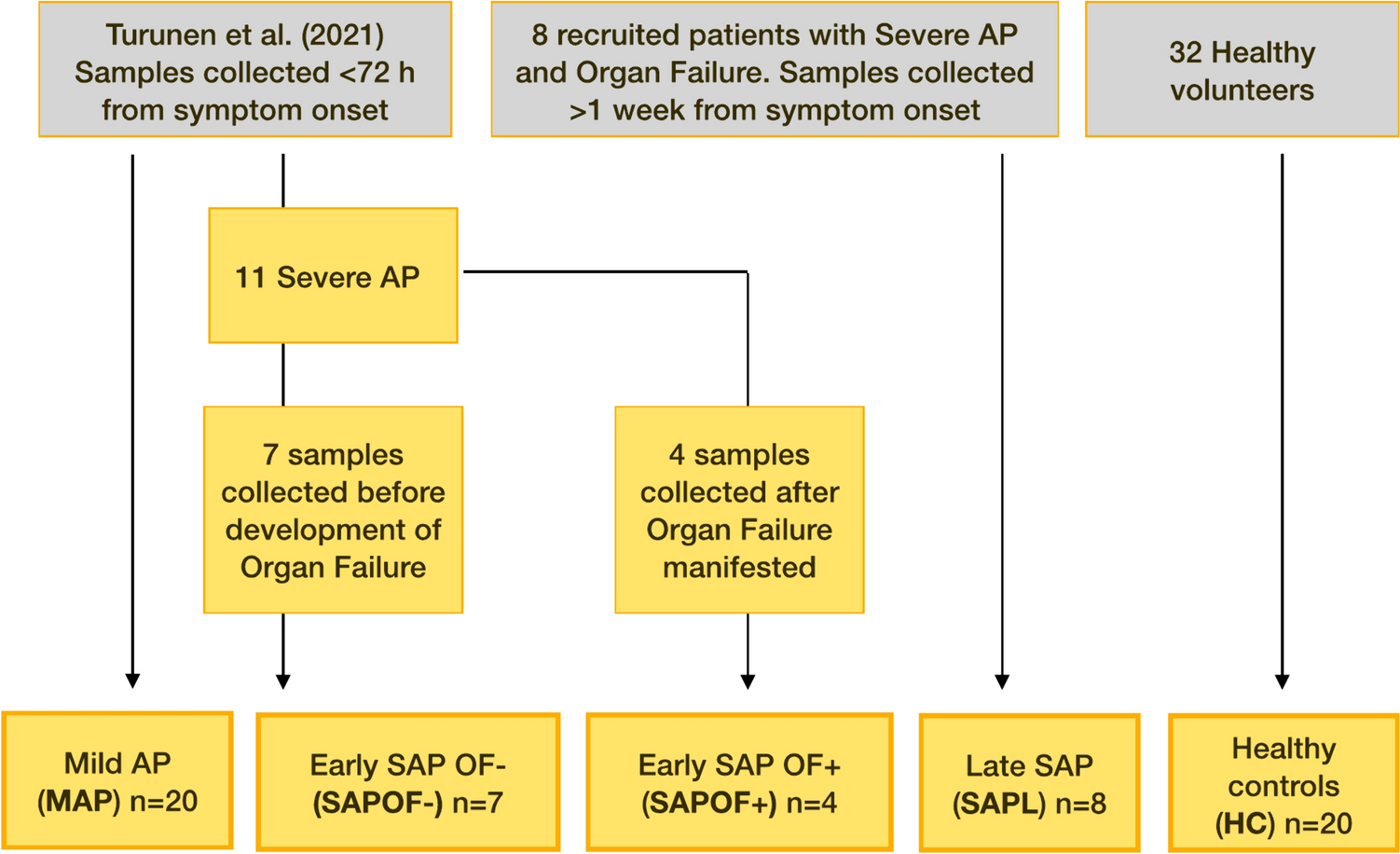
The present study was designed as a pilot study to test the feasibility of measuring circulating necroptosis markers in AP. Thus, the number of samples studied was relatively low in order to limit cost. Also, patients with severe AP are overrepresented as only a random sample of mild AP patients was included and those with moderately severe AP were totally omitted. Thus, the results should be considered preliminary as they are hampered by low sample size and distribution of AP severity not completely representing the clinical setting. The findings need to be validated in a larger cohort of AP patients. This would also allow analysis of necroptosis markers with respect to a more diverse array of clinical outcomes, such as mortality, pancreatic necrosis, and other complications.
Another limitation is that the levels of TNF and IL-1β turned out to be very low in the majority of samples making their interpretation difficult. This, however, emphasizes that as these crucial proinflammatory mediators are unsteady and purged rapidly from the circulation, novel and more suitable prognostic biomarkers are needed. Also, among limitations is that the study setting did not allow tracing the origin of the necroptosis-related plasma markers. However, in a mouse model of AP, dramatic increase in MLKL expression was observed specifically in the pancreas [7]. Furthermore, accumulating evidence suggest that RIPK and MLKL levels in the blood reflect the severity or activity of diseases in which pathogenetic necroptosis takes place in the affected organ [9,10,11]. As yet another limitation, we recognize that drawing direct conclusions about necroptosis inhibition as a near-future treatment option in AP and the related OF is premature. Instead, much research is required for defining the ultimate cell type- and tissue-specific effects and outcomes associated with necroptosis inhibitors, as well as effective and safe dosage and timing of inhibitor administration.
Conclusions
To conclude, the results of this pilot study show that plasma levels of sST2, the soluble receptor of the necroptotic alarmin IL-33, and the inflammatory cytokine IL-6, are able to predict the development of SAP. Levels of RIPK3, a kinase with necroptotic and non-necroptotic inflammatory functions, appear to be associated with SAP. Elevated levels of the necroptosis executor MLKL are seen in MAP patients and even more prominently in patients with persistent OF. While still requiring more research, the results support the idea that reversing necroptosis may be an appealing option to optimize AP treatment.






留言 (0)