
記住我
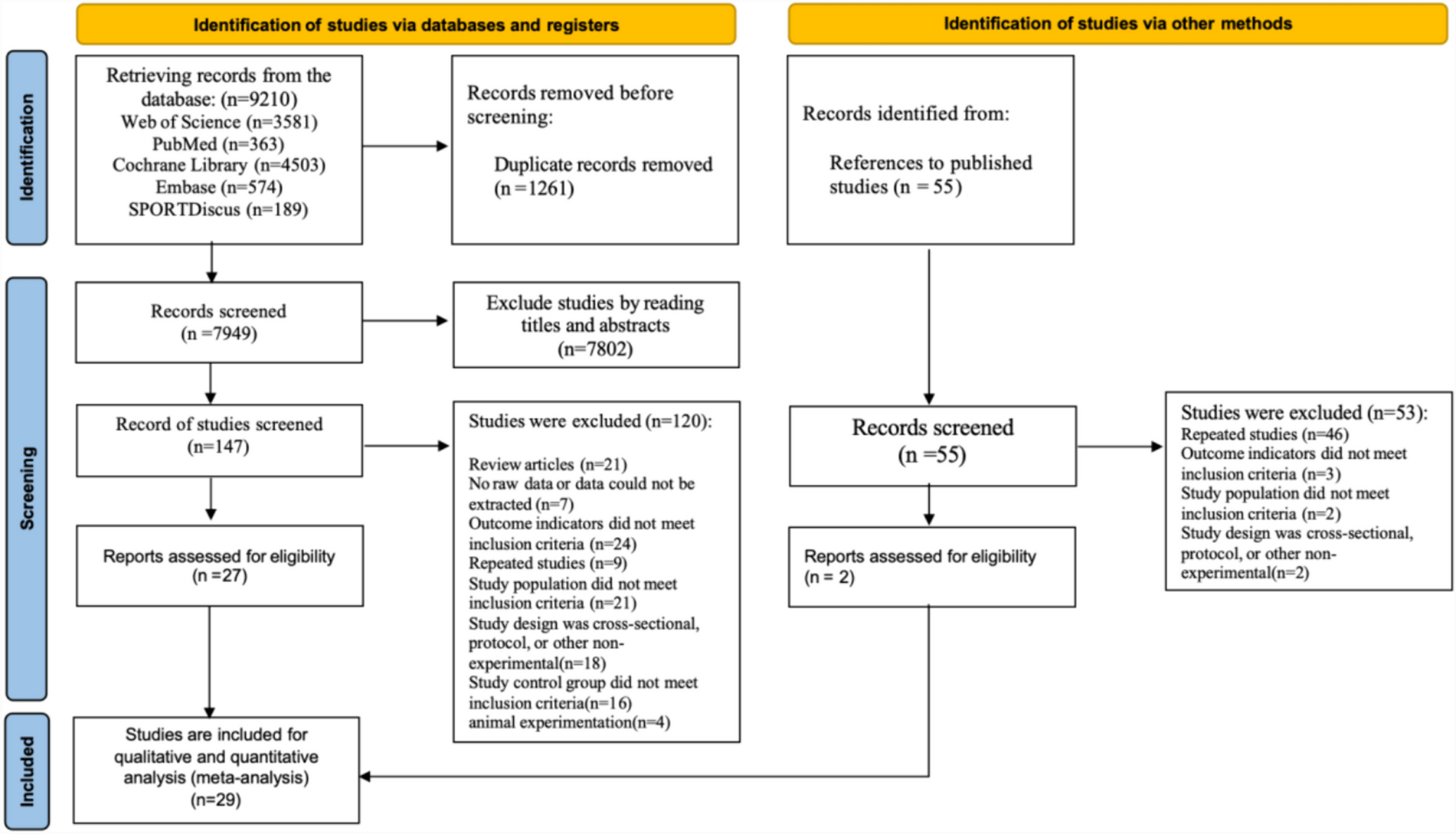
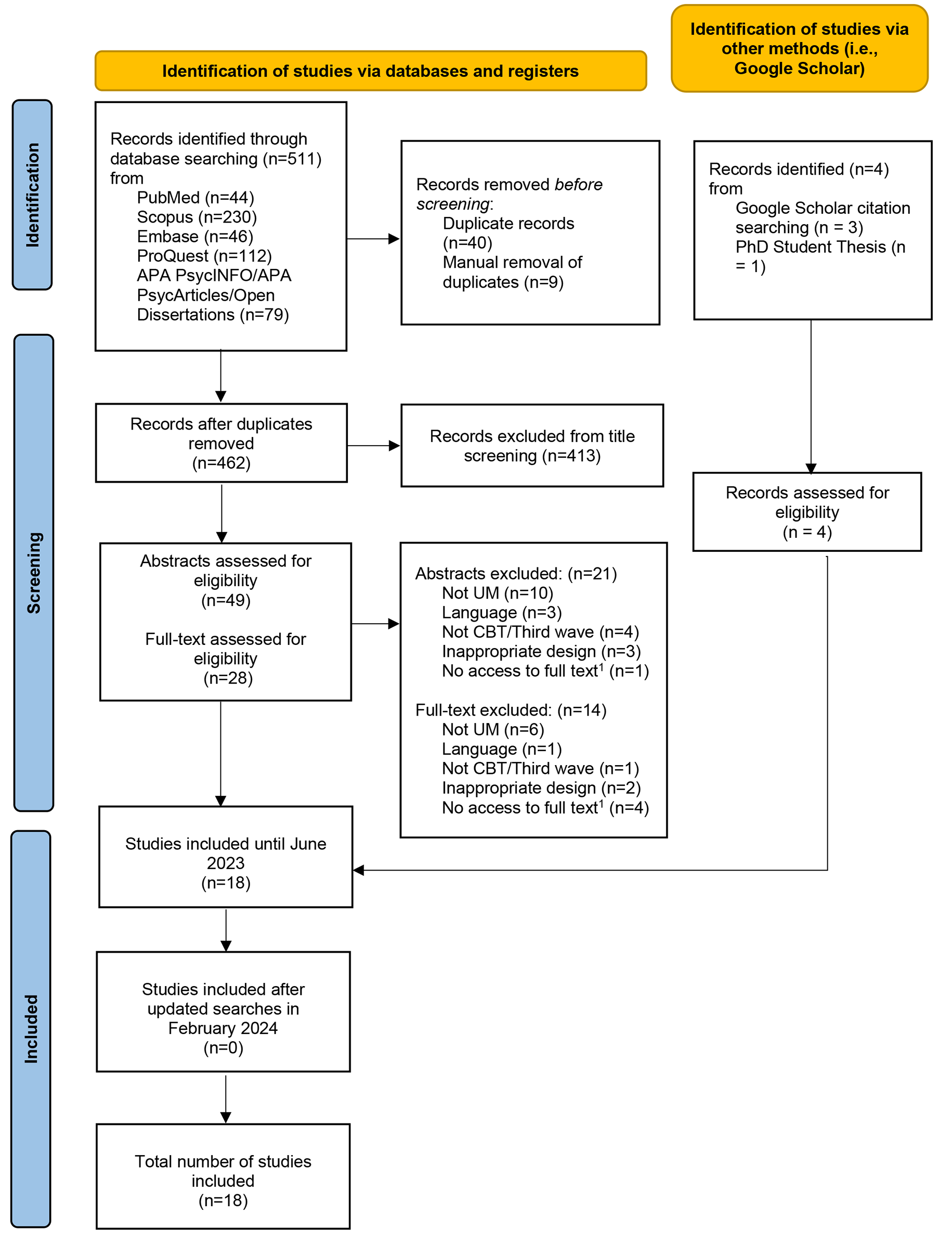
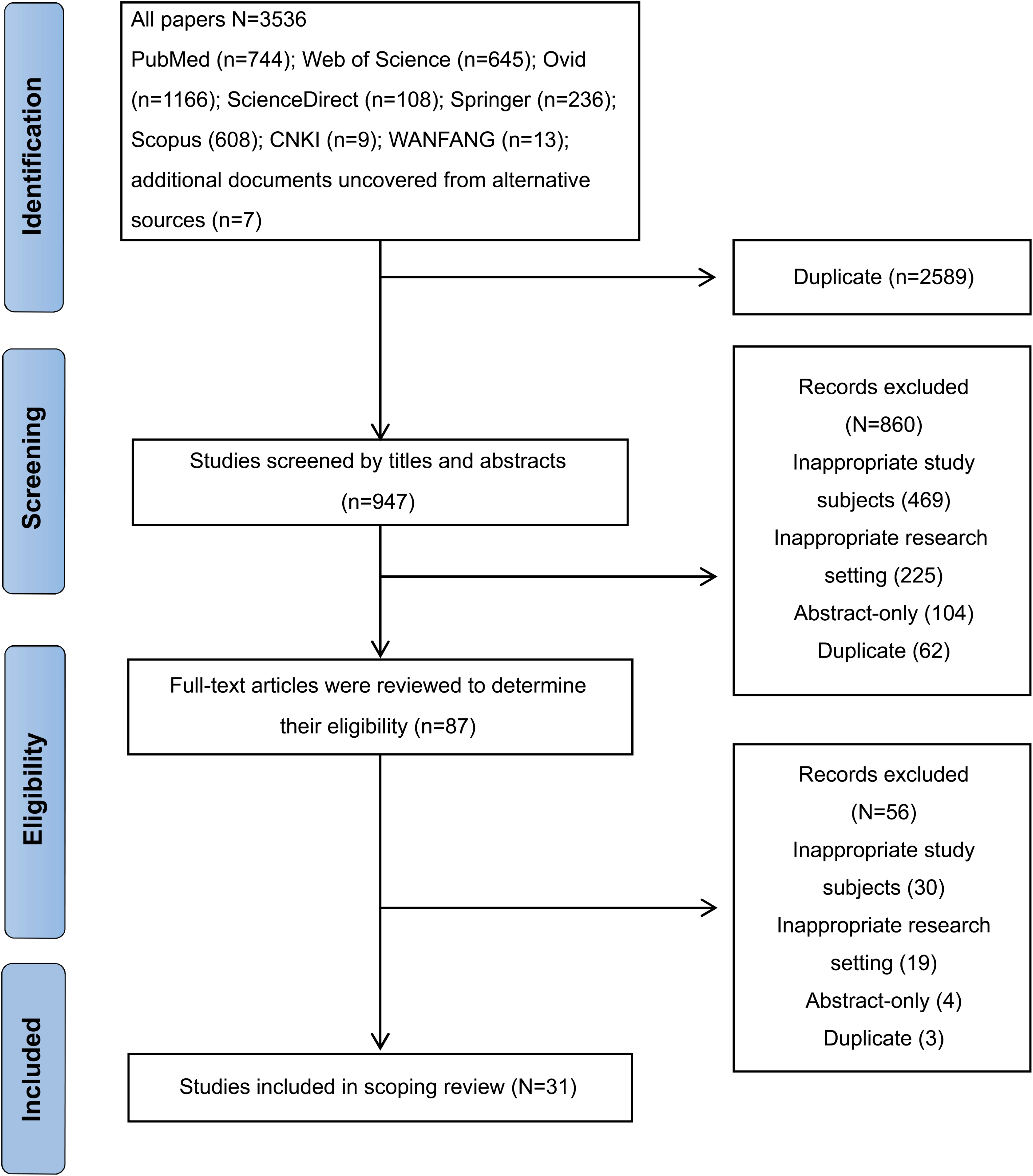

Searches identified a total of 511 records. After the removal 483 records (462 duplicates, 21 abstracts excluded), the full texts of 28 studies were assessed for full-text screening with 18 finally included (See Fig. 1). Studies included varied in methodology adopted: most studies were quantitative (n = 12, 66.7%), followed by mixed methods (n = 5, 27.8%), and qualitative (n = 1, 5.6%). Two studies were published in 2005 (n = 2, 11.1%) and the rest were published between 2015 and 2023 (n = 16, 88.9%) All studies were carried out in developed countries with most being conducted in Germany (n = 6, 33.3%). Almost half of the included studies implemented a cohort study design (n = 8, 44.4%) and most were carried out in community or outpatient settings (n = 11, 61.1%). Most studies included UM that originated from different countries (n = 15, 83.3%). Sample sizes ranged from one participant to 147 (Mean = 34.6). Although most studies included female UM in their sample (n = 14, 77.8%), from a total of 670 participants, females were greatly underrepresented (n = 142, 21.2%). The age of participants ranged from 4 to 20 years old (Mean = 16.22, SD = 1.29).
Fig. 1
PRISMA flow diagram
Note.1 An attempt was made to retrieve the full-text by conducting the corresponding author of the article but failed
The type of intervention predominantly used was TF-CBT (n = 10, 55.6%), with group therapy being the most common treatment modality (n = 11, 61.1%). For group therapy studies, the duration of intervention ranged from 4 to 35 weeks (Mean = 9.2 weeks) with each group lasting between 60 and 120 min. Studies of individual sessions intervention ranged from 1 to 48 sessions (Mean = 12.2 sessions), with sessions lasting between 60 and 100 min. From the included studies, less than half had follow-up assessments ranging from one to six months (n = 7, 38.9%). With regards to inclusion and exclusion criteria, some studies required participants to have PTSD symptoms to be included (n = 10, 55.6%), a PTSD diagnosis (n = 4, 22.2%), or were excluded if they presented with severe mental illness such as psychosis or acute suicidality (n = 7, 38.9%). With regards to language, either interpreters were used (n = 6, 33.3%), intercultural mediators (n = 3, 16.7%), bilingual therapists/research assistants (n = 2, 11.1%), or UM were excluded due to not speaking the language of host country (n = 5, 27.8%). The characteristics of included studies can be found in Table 1.
Table 1 Characteristics of included studiesQuality assessmentAn overview of the quality assessment can be seen in Table 2. The assessment of the quantitative studies (n = 17, 94.4%) with the EPHPP tool resulted studies attaining the following scores: “weak” score (n = 10, 58.8%), followed by “moderate” (n = 5, 29.4%), and strong (n = 2, 11.8%). Weak studies scored poorly for blinding, controlling for confounders and selection bias. The assessment of the qualitative component of included studies (n = 5, 31.6%) using the CASP tool resulted in studies attaining the following scores: “weak” score (n = 1, 20%), “moderate” score (n = 2, 40%), “strong” score (n = 2, 40%). Weak and moderate qualitative studies did not clarify the theoretical underpinnings (e.g., ontological and epistemological assumptions) of the study; did not clearly explain how data was collected; did not adequately consider the relationship between researcher and participants; did not provide an in-depth description of the analysis to justify that the data analysis is sufficiently rigorous; did not present a clear statement of findings with evidence both for and against the researchers’ arguments; and finally the researchers did not demonstrate how they examined the credibility of their findings (e.g., triangulation, respondent validation, multiple analysts). A more detailed depiction of the EPHPP and CASP appraisals can be found in Online Resource 3 and Online Resource 4.
Table 2 Study quality appraisalQuantitative resultsImprovement in QoLOf the 18 studies, only two (11.1%) used quantitative measures for assessing QoL [60, 61]. Both studies used the Cantril Ladder [62] to assess life satisfaction. Authors reported that TF-CBT seems to significantly increase life satisfaction, but only for UM whose asylum application had not been rejected or who were still awaiting a decision [61]. In another study, authors did not undertake statistical testing as the scope of their study was feasibility rather than effectiveness. Nonetheless, the authors reported improvement in mean scores on the Cantril Ladder following TRT, at post-intervention and at 18-weeks follow up [60].
Improvement in psychopathology symptomsCognitive behavior therapy (CBT)Three studies (16.7%) examined CBT in UM [63,64,65]. Group CBT appeared to result in a significant decrease in overall PTSD symptoms severity and intrusive PTSD symptoms. UM also appeared to improve with regards to behavior and emotional difficulties [63]. Unfortunately, these improvements were not maintained at 2-month follow-up [63]. In a case study, the author reported that after sixteen sessions of individual CBT, the UM had moved from a severe PTSD score to minor symptoms although this was not considered a clinically significant reduction [64].
Trauma-focused cognitive behavior therapy (TF-CBT)Ten studies (55.6%) examined TF-CBT in UM. TF-CBT appeared to reduce PTSD symptoms in most studies (n = 7) [66,67,68,69,70,71,72] with medium to large effect sizes [68,69,70] and improvements were maintained at two weeks to 6-months follow-up [61, 67, 68, 73]. Improvements were mostly observed in the domains of re-experiencing and avoidance, as well as alterations in cognitions and mood [69]. TF-CBT also appeared to reduce depression symptoms with medium [70] to large effect sizes and maintained at 6-months-follow-up [67, 68, 71]. Reductions in anxiety symptoms [67] and improvements in emotional difficulties [72] were also noted.
Third wave cognitive behavioral interventionsThree studies (16.7%) were classified as third wave CBT interventions [74,75,76]. A third wave group intervention (i.e., CBT, ACT, DBT, CFT) with UM (n = 14), seemed to observe significant improvement in behavioral difficulties but not in PTSD symptoms [74]. Researchers conducting an MBI group intervention (n = 9), appeared to significantly reduce negative affect of UM with a medium effect size [75]. An ACT group intervention with UM (n = 12), seemed to result in significant reduction in PTSD and depression symptoms in the intervention group compared to the control group (no intervention) and authors noted increases in psychological flexibility and mindfulness with very large effect size [76].
Multimodal approachesTwo studies (11.1%) reported on programs that provided a range of strategies to improve MH in UM [77, 78]. A multimodal trauma-focused treatment approach, (n = 41) appeared to result in significant decreases in PTSD symptoms with a very large effect size [77]. An overview of the reported outcomes of included studies can be found in Online Resource 5.
Qualitative resultsOf the 18 studies included, only five (27.8%) investigated treatment acceptability of the intervention. Characteristics of the included studies can be found in Online Resource 6. The QRS resulted in the development of two core categories (see Table 3). The category “Treatment components” contains three themes and describes various aspects of the treatment such as tools and coping strategies used by participants, the adaptability of the treatments and how acceptable the interventions were perceived to be. The “Treatment outcomes” category contains two themes and reflects what participants reported gaining from the interventions. Outcomes included an abatement of emotional symptoms and additional benefits observed by participants such as the sense of belonging. These themes are situated within an overarching concept “Creating safety and cultivating togetherness”. The distribution of themes across included papers are presented in Table 4. All quotations are taken from the study participants, therapists, or stakeholders, unless specified as an author comment.
Table 3 Categories, themes, and overarching conceptTable 4 Distribution of themes across qualitative studiesTreatment componentsThis category includes three themes: the tools and strategies that participants found useful, adaptability of therapists and interventions used, and how acceptable participants perceived the interventions to be.
Tools and strategiesThis theme depicts feedback of UM on the tools and strategies learned from CBT and third wave interventions. The exercises were considered valuable, and UM incorporated them into their daily lives. In four studies, UM assimilated new tools learned with previously established helpful strategies, whereas other UM seemed to replace maladaptive coping mechanisms with more adaptive methods.
“These exercises help me a lot to handle my fear and anxiety. I get these attacks every night and I think if I had not done these exercises I would have been even worse.” [71].
“When I can’t concentrate at school or when I go to sleep at night, I do an exercise. It helps.” [75].
“The mindfulness exercises are helpful when I can’t concentrate with school or when I have a lot of stress. I do some exercises. At night I prefer to pray.” [75].
“After doing exercises I’ve learned here, I’ve reduced sleeping pills.” [71].
Although four studies reported that some UM found the tools learned indispensable, it was also noticed by three studies that it is not always easy to change already established coping mechanisms.
“To practice the exercises was quite difficult to do because I barely did it on my own so. It was just something that didn’t cross my mind. I didn’t think about practicing.” [75].
In one study authors reported that “other useful strategies mentioned were distraction, such as listening to music, or activation, such as hanging out with friends or talking to someone they trusted.” In other cases however, “one of the young people stated that nothing can be done about the situation except to endure” [71]. Furthermore, a therapist in another study reported that “despite lively discussion about the trauma narrative, in the end, they mostly felt, it’s still probably good to avoid things” [65].
AdaptabilityThis theme illustrates the ways in which therapists adapted the intervention protocols to meet the needs of UM. Clinicians in a study reported that they would improvise to engage young people and use exercises from other training they had attended or that “had been shared informally by colleagues”. Some therapists felt it “was not productive to push them to talk about their worst experiences if they were not ready”. For instance, facilitators would emphasize “coping skills and address acculturation stress over disclosure of trauma”. Furthermore, one therapist “found herself moving away from CBT and using an intervention from her own culture” [65].
“Like the skills, you really have to twist how you present or how you teach them because for me… it has been more effective to sit with a group of students from Guatemala and burn sage than talk about the CBT triangle.” [65].
Furthermore, adaptability also concerned the measures that the research team took to engage participants. For instance, in another study reported that UM “appreciated the outreach work as five participants stated they would not have participated if they had to travel to a mental health institution” [78]. The dedication shown from clinicians was an important factor in participant engagement.
“They come back, and again, they don’t give up. Sometimes I was tired and wanted to sleep and did not want to talk, but they came back and helped me and little by little, I started talking.” [78].
Another adaptation when working with this population may be individual attention to some UM in addition to group treatments. Authors reported that some UM “would have liked more individual conversations with the group facilitators” [71]. Other authors observed that “one youth stated he preferred to talk about some issues alone with the therapist” [65].
AcceptabilityFindings related to acceptability were mixed throughout three studies. Whilst in one study authors reported that “most participants found the treatment helpful and would recommend it to others” [78], clinicians in another study expressed that the intervention “didn’t quite land” for the young people [65].
“It is boring. If something is not interesting you don’t want to stay, you want to go. For me it was difficult to concentrate and nothing changed between the first and second session.” [75].
“I went to one session, I see the exercise and it was kind of interesting. We had to think and this was good. It was not difficult but I don’t need it. This is just not for me.” [78].
Furthermore, authors reported that in their study “participants mentioned how the language of the MBI program has hampered an adequate participation” [75]. Nonetheless, authors mentioned that “both participants mention how this language barrier seemed to be slightly reduced by the possibility to interact with the trainer. Furthermore, this interaction made it possible for the participants to obtain additional information about the concepts and attitudes of the practice of mindfulness, which they experienced as helpful.”
Treatment outcomesThis category includes two themes: the decrease of internal private events (i.e., emotions, thoughts), and additional benefits that UM observed from the interventions.
Emotional symptomsThe abatement of emotional symptoms is a theme that was apparent throughout all included studies. Participants expressed noticing a decrease in anxiety, stress, and sadness. UM also mentioned an improvement in concentration and a feeling of calmness. Moreover, researchers noted that participants “reported having been helped with sleeping difficulties, intrusive memories, depressed thoughts, fear, and irritation” [71].
‘Before I came to the group I felt very sad and worried, since coming here I have opened up and I feel relaxed’ [74].
“The calmness you felt after doing these exercises, it was great to be able to feel this calm.” [71].
“For me the most important thing was that when you are down or you are in a mental crisis, how to get yourself out of it, how to save yourself somehow.” [71].
“Before I wasn’t interested, I didn’t feel like doing anything. I didn’t want to go to school. Or didn’t go to appointments. Sleeping was also difficult. After and during the treatment, I feel like I’m more keen, I go to school and to the appointments.” [78].
Throughout the studies however, there was also an overwhelming need for UM to learn how to control their internal private events.
“When I came to this group I had no control of myself, because everything I had been through affected me and was controlling me. The group helped me to gain control over myself.” [71].
“I can control stress and I can control my fear, I can control that I cannot sleep, but I have difculty controlling my anger. That’s really difficult to control.” [71].
Additional benefitsThis theme included other benefits that participants felt they had gained from the treatments. Authors in one study reported that participants could “address difficult topics with loves ones and experienced an improved relationship with friends and family. Other benefits included feeling proud of themselves and improved self-care” [78].
“I learn to appreciate things, and they taught me how to give advice to other people.” [65].
“Now I have a chance to see all different parts of my life, the good and the bad. This offers me balance.” [78].
Moreover, some UM also conveyed a feeling of having developed a new identity following the treatment. Authors explained that UM were able to assimilate their previous experiences into their present identity, by discussing issues with peers and considering themselves in relation to the culture of the host country. Importantly, UM also experienced a sense of belonging following the treatment they received [71].
“From the first time I came to Sweden, I feel that I am a newborn, now I belong to this world as well.” [71].
However, despite improvements in emotional symptoms and other benefits, authors reported that “many of the boys expressed dejection and described how incidents in the home country affected them” [71]. The impact of current stressors was also evident and had a negative impact on treatment benefits. Authors reported that most UM “spoke about the daily stressors they continued to experience, including worries about the future, anxiety concerning family reunification, troubles with peers, and worries about the lives and wellbeing of family members.” [78].
Overarching concept: creating safety and cultivating togethernessThe two core categories are nested within an overarching concept of creating safety and cultivating togetherness. UM expressed feeling less alone through the process of sharing life narratives. UM felt support by peers and therapists, and they reported that the groups created a sense of safety. Authors reported that UM “described a trust in the group and the fact that it felt safe to open up” [71]. In another s
留言 (0)