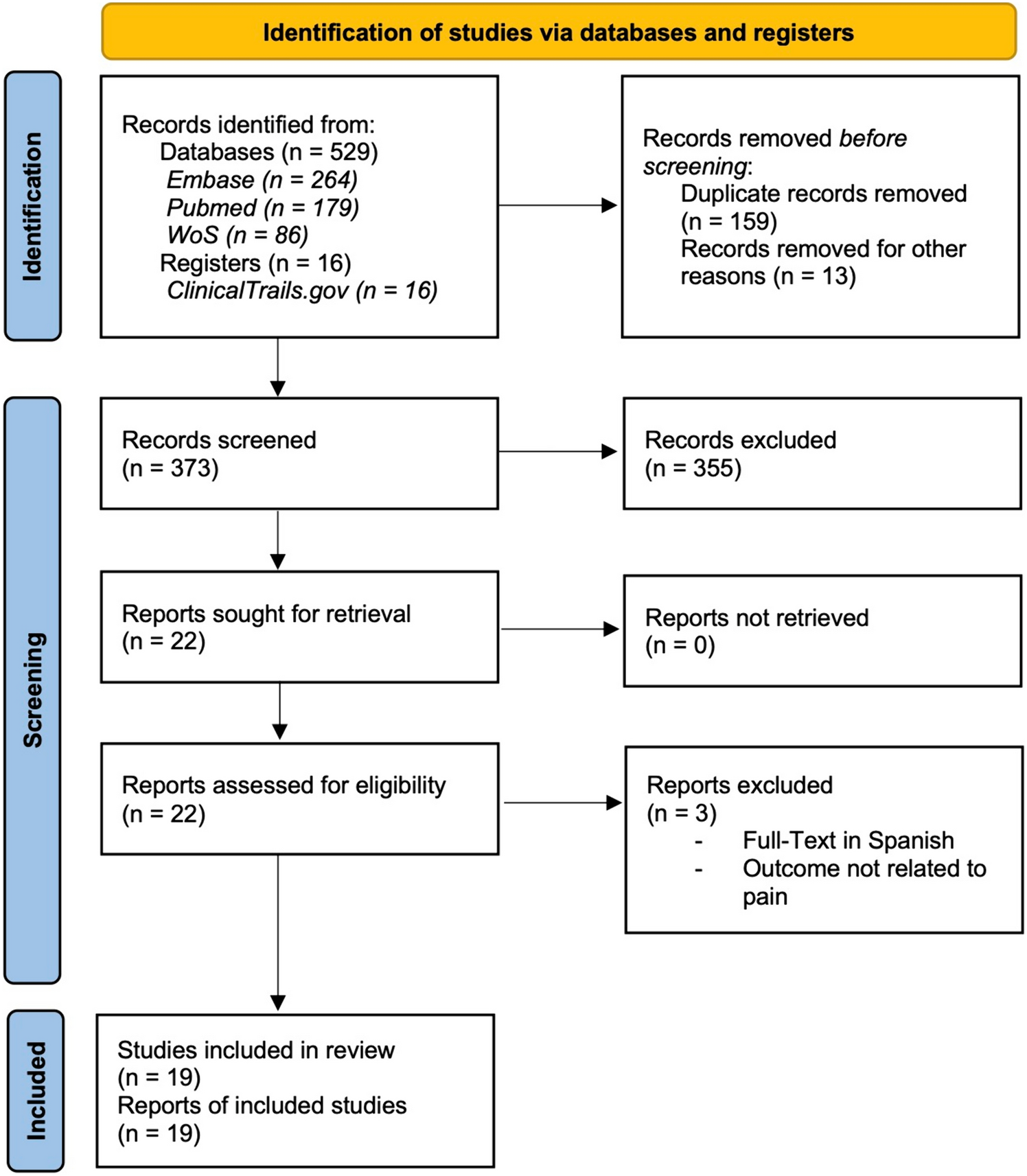
Over the past few decades, there have been significant advances in the treatment of rectal cancer ranging from administration of total neoadjuvant therapy with potential for organ preservation to development of variable operative approaches for proctectomy. These operative approaches include total mesorectal excision, transanal total mesorectal excision, and minimally invasive approaches such as laparoscopic or robotic-assisted surgery. Operative technology continues to evolve not only to enhance oncologic outcomes but also for improved patient experience and recovery. Among these approaches, robotic-assisted surgery is becoming the most rapidly accepted among surgeons, especially for complex pelvic surgery such as proctectomy with total mesorectal excision. This presumption is confirmed in our large retrospective study which demonstrates that RAS was utilized for oncologic proctectomy for only 16.6% of cases in 2013 but rose to 57.1% of cases in 2020 (e-Fig. 1).
One of the most desired outcomes for surgical management of rectal cancer is that of sphincter preservation and avoidance of a permanent colostomy. However, restoration of intestinal continuity may be quite difficult for very low rectal cancers, especially in obese patients or male patients with a narrow pelvis. In this study, we found that patients who underwent RAS had significantly greater rates of primary anastomosis with ileostomy as compared to both open and laparoscopic approaches which had rates greater than 50% for permanent colostomy creation. A common assumption is that robotic surgery helps aid deep pelvic dissection due to improved instrumental dexterity/articulation, stable camera platform, and magnified 3-dimensional imaging with enhanced depth perception.
In this study, we identified significant intraoperative and postoperative advantages for RAS proctectomy compared to both open and laparoscopic proctectomy. The most discussed and studied intraoperative impact of RAS proctectomy for the management of rectal cancer as compared to laparoscopic surgery is need for conversion to open surgery. A large meta-analysis completed by Simillis et al. in 2019 found no significant difference in rate of conversion to open surgery among these approaches [11]. However, it may be difficult to generalize the results of the study given the heterogeneity of the trials included in the analysis. In contrast, meta-analyses of 6 randomized controlled trials and 5 propensity score-matched case-matched (PSM) studies completed in the same year by Phan et al. found significantly lower rates of conversion to open surgery with robotic surgery as compared to laparoscopic surgery, in a pooled analysis (OR 0.38, 95% CI 0.30–0.46) as well as in separate analyses of the RCT studies (OR 0.28, 95% CI 0.00–0.57) and PSM studies (OR 0.39, 95% CI 0.30–0.47) [12]. Similarly, a meta-analysis of 5 RCTs completed by Prete et al. concluded that RAS was associated with lower rates of conversion to open surgery as compared to laparoscopic surgery (RR = 0.58, 95% 0.34–0.97) [13]. Our study shows a significant reduction in the likelihood of conversion to open surgery for RAS proctectomy compared to laparoscopic among patients who received a colostomy or ileostomy. This finding is important as it included larger sample size than the prior mentioned studies and may be more representative of the diverse surgical practice in the USA given the database employed.
Other commonly questioned outcomes in the evaluation of operative approaches are those of postoperative morbidity. In our study, we identified that RAS proctectomy with either ileostomy formation or creation of permanent colostomy had a significantly lower likelihood of postoperative ileus and bleeding when compared to laparoscopic surgery, as well as a significantly lower likelihood of postoperative anastomotic leak, bleeding, and blood transfusion when compared to open approaches. Although intraoperative blood loss estimates can be quite skewed and subjective, these results coincide with those from prior smaller studies [11, 14, 15]. Reduction in risk of blood loss and need for transfusion is particularly important in the treatment of cancer, as perioperative blood transfusion has been associated with negative oncologic outcomes including increased risk of tumor recurrence and reduced survival [16, 17].
Additionally, we identified that RAS proctectomy had a significantly reduced likelihood of postoperative ileus and length of hospital stay when compared to laparoscopic and open approaches. These results correspond to results from the largest meta-analysis completed in 2019 by Simillis et al. While minimally invasive surgery has been consistently associated with faster recovery and decreased hospital length of stay compared to open surgery for numerous different operations, it remains unclear why RAS proctectomy has lower length of stay and reduced risk of ileus as compared to laparoscopic. We may surmise that this may be due to decreased analgesic requirements for RAS as shown by Christoffersen et al. [18] and Donlon et al. [19] as well as decreased rates of conversion to open surgery. Regardless of the reasons for this finding, the data are generalizable to the population as a whole.
Interestingly, our analyses also demonstrated that RAS proctectomy with permanent colostomy was associated with a significantly greater likelihood of discharge to home compared to both laparoscopic and open approaches. This is of great importance not only with regards to patient comfort, but also with respect to healthcare expenditure. Our group and others have previously demonstrated that postacute care services and hospital length of stay both strongly impact cost of care [20,21,22]. Furthermore, prolonged hospital stay while awaiting discharge to skilled nursing facilities or rehabilitation centers can significantly hinder hospital bed availability, which remains a constant burden on large healthcare facilities in urban settings in the post-COVID pandemic.
This study has several limitations related to retrospective analyses. First, the study uses administrative data which lack many of the important medical record details that might reveal whether each variable was coded properly. For example, obese/overweight status is likely to be underestimated in administrative databases, although we do not expect this to be differently assessed between surgical exposures and hence unlikely to change our findings. Additionally, there are many differences in the patient characteristics between each study arm. However, this was corrected for as best possible with the multivariable logistic regression models and IPTW to adjust for the difference between groups and minimize selection bias. Finally, our database did not include oncologic characteristics including tumor size, stage, or use of neoadjuvant therapy which may impact operative approach utilized and postoperative outcomes.
Despite these study limitations, these real-world data which account for approximately 25% of US in-patient admissions per year are more likely representative of current clinical practice and outcomes than that of the previously conducted clinical trials. Clinical trials are typically performed by surgeons with vast laparoscopic or robotic experience which will not reflect actual population-based results which we have identified here. In addition, we included surgeon volume as a covariate in our analysis to control for surgeon learning effect. Our data reveal that for the general population, robotic-assisted surgery may facilitate sphincter preservation and improved total mesorectal excision with lower risk of conversion to an open operation and improved postoperative outcomes/recovery.

留言 (0)