
記住我


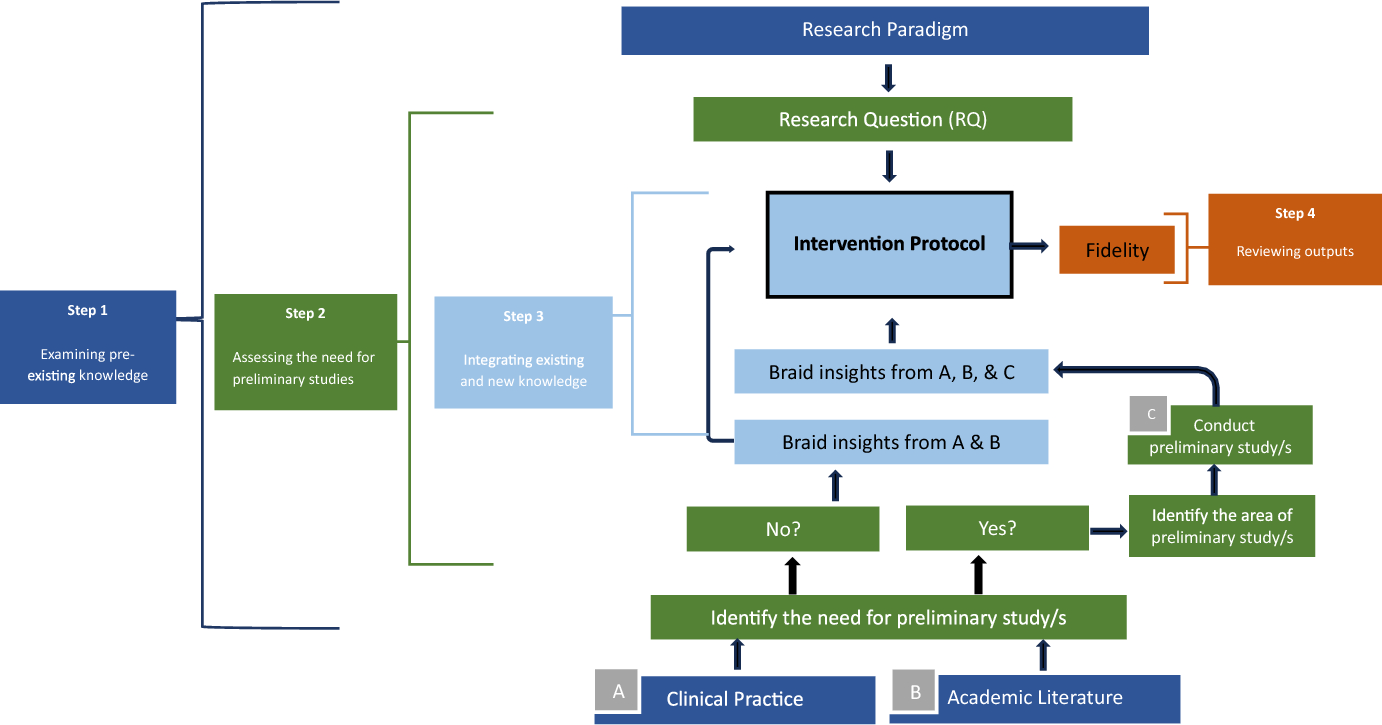





Treatment resistant depression (TRD) is a type of depression where one’s symptoms do not reduce despite intervention (Al-Harbi, 2012). Specific theoretical underpinnings of DMT, precisely that of the mind–body nexus (Berrol, 1992), embodiment, and kinesthetic empathyFootnote 1 (Barrero González, 2019; Christopher & Tamplin, 2022; Joufflineau et al., 2018) show promise for symptomatic relief if used in treating resistant depression. However, considering the vulnerability of the population (Gaynes et al., 2020), the mere theoretical potential from a few studies did not provide sufficient knowledge-based insights to help develop the intervention session plan in my research project. Additionally, the emerging literature on treatment resistant depression (TRD) emphasises a prevalence of comorbidities and possible intersections of race (Liu et al., 2021), which further marginalised potential research participants. This re-emphasised the duty of care required through the research planning process to develop an intervention session plan for a first-of-its-kind research study with DMT and TRD. I engaged in a four-step creative problem solving process to develop the intervention session plan for my project. This has been graphically represented in Fig. 1 below.
Fig. 1
An illustrative depiction of a four-step creative problem solving process used to help develop a DMT intervention session plan over 2.5 years
STEP 1: Examining Pre-existing KnowledgeKnowledge is perceived and understood differently across the world. To me, knowledge is best described as the oral or visual understanding that enables us to comprehend the world around us (Cameron, 2020). While examining pre-existing knowledge in step 1 of my problem solving process, I retained this description of knowledge. I consciously considered both formal and informal forms of knowledge, as seen in the questions I sought answers to in this step:
What do I already know about this topic from my clinical experience?
What does the literature say about this topic? and,
How does the ‘self’Footnote 2 of the researcher play a role in influencing the research interests?
In addition to a traditional literature review process, I reflected on the inception of my research interests, which were birthed from my clinical practice.
Clinical PracticeIn the early years of my career, I worked as a dance/movement therapist with older adults living with severe and persistent mental health conditions at an outpatient clinic. During this time, I worked with Dina.Footnote 3
Dina was a 66-year-old African-American woman admitted to an outpatient clinic directly after her discharge from an adult in-patient psychiatry ward. She enjoyed the music of Johnny Cash and grooving to disco. Dina was diagnosed with depression and had a history of psychosis and interpersonal conflict. The clinic offered various services, including dance/movement therapy, cognitive behavioural therapy, support groups, housing support, psychopharmacology, and recreational groups. Most of which Dina proactively used/participated in five days a week. Dina roughly participated in two group DMT sessions a week and one individual DMT session every two weeks, amounting to monthly direct contact hours of 7.5 hours with me across 18 months. My work required robust documentation on the client’s experience of sessions. Some of her feedback that struck me includes, “I feel good”, “I enjoy it. You don’t get to do things you enjoy when you get to my age”, “It is so lovely to dance with you”, “Dancing with you is different” and, “these sessions help me get my stress out sometimes”. Dina often reported experiencing significant stress in her life, including a fear of homelessness and loss of health insurance. Although Dina continued to take her medications as prescribed by the psychiatrist, participate in therapy sessions, and attend services offered at the clinic regularly- she still expressed dissatisfaction with her mood. She reported not feeling the benefits of the various interventions despite active participation.
Revisiting Dina’s story helped me reconnect with my curiosity about kinesthetic empathy and the therapeutic movement relationship in DMT. I was also keenly aware that the process of DMT juxtaposed the treatment resistance she experienced at the clinic. Concurrently, I reconnected with my somatic cues of frustration that stemmed from a dissonance between my value of justice-based equitable care that evolved with clients’ needs and structural limitations of support in the outpatient healthcare system in the USA.
The Self of the Researcher and Research ParadigmThe ‘self’ of the researcher is an undeniable part of research planning and warrants similar reflexive exploration as aspects of the research paradigm (as mentioned on p. 1). Here, I refer to ‘self’ as the paradoxical being which is both the essence and the totality of one’s personality, as Jung (1875–1961) described it (McGehee et al., 2017).
AxiologyFootnote 4: Our values play a significant role in justifying our rationale in research. Further, our choices are “influenced by the type of person we are, our experiences, culture, background, social, and economic status” (Roots, 2007, p. 20). Understanding our values from an embodied lens can help clarify research interests and inform the study design and intervention protocol. For instance, awareness and curiosity of my embodied cues (of discomfort and tension) while witnessing the dysregulation my clients experienced due to sub-optimal intervention effects clarified the scope of my research and the focus of the intervention protocol. They were (i) generating systematic knowledge on DMT and TRD and (ii) focusing on emotional regulation in the intervention designed for TRD, respectively. Another example of the influence of my axiology is seen in my use of interviews in data collection and active inclusion of storytelling, meaning-making, and dance stories in the DMT session plan, which stem from the personal value I place on multiple perspectives and oral narratives.
EpistemologyFootnote 5: Another core aspect of identifying a research paradigm is to clarify the researcher’s understanding of knowledge and its creation. By recognizing my embodied response of feeling energised at the thought of combining scientific inquiry with my research participants’ lived experiences, I discovered the importance I laid on knowledge being congruent with social realities (Park et al., 2020). I gained further clarity that my perception of knowledge is “relative to particular social and historical arrangements” (Scott, 2007, p. 5), amounting to epistemic relativism. Like my axiology, these insights also influenced my research’s design and data collection method.
Ontology5: Growing up in a mixed-caste family in India, I was exposed to differences and diversity at a young age. This helped me recognise how social, economic, and cultural factors can affect the perception of one’s reality. My ontological stance is that of a critical realist stance, where one’s perception of reality is affected by their social reality and context (Alele & Malau-Aduli, 2023). For me, my ontological stance was crystalised through my interoceptive awareness. While reviewing different ontological stances, I noticed my body ‘tense up’, namely in my breath, gut, and diaphragm. As I educated myself on the critical realist stance, I noticed these functions to be restored to their natural state. I also noticed that I was no longer clenching the inner muscles of my chest and that my diaphragm had eased back into its resting state. In this way, interoceptive awareness (Khalsa et al., 2009) helped me confirm my ontological stance and create an embodied link between the ‘self’ of the researcher and key steps in research planning.
Methodology: To me, the mind–body nexus inherently symbolises the convergence of two forms of knowledge. Just as DMT embraces both cognitive and somatic processes, similarly, I noticed myself being intuitively drawn to converging two types of data sets by adopting a mixed methodology. From a philosophical perspective, a mixed methodology is rooted in the complexity of reality and seeks to lay a necessary emphasis on different vantage points on a given topic (Watson, 2020). Thus, a mixed methodology could embrace the complexity of TRD and the need for various data sets due to the novelty of this study. Here, I noticed and relied on my embodied felt sense of discerning between ‘alignment vs. fragmentation’ to ensure a clear, logical link between my chosen research paradigm, research interests and the ‘self’ of the researcher. An equally important consideration is the relevance of the intended methodology with the research question; however, I do not reflect on this in this manuscript, as this is commonly discussed in the literature (Tashakkori & Creswell, 2007).
STEP 2: Assessing the Need for Preliminary StudiesTypical of any research endeavour, I first formulated my research question using insights from step one (above), as suggested by McFerran and Silverman (2018). At this stage, my research question was, ‘How can a 12-week group dance/movement therapy intervention support stress management and emotional regulation in adults living with treatment resistant depression?’ Evidently, the research question had a cascading effect on the rest of the research planning process. Next, I revisited the literature reviewed in step one from the lens of the research question. This aimed to ascertain if I had access to enough literature or oral knowledge to develop a session plan that would directly answer the research question. Here, oral knowledge can be best understood as a broad term covering varied lived experiences and stories. Here, the following questions contributed to my successfully navigating this step:
How can I develop an intervention session plan based on existing information (of varied forms)? or
Do I need to generate more knowledge on these topics before I can develop an intervention session plan that can answer the research question?
These questions helped me determine the need for preliminary studies to develop an intervention session plan based on adequate evidence. Once the need for preliminary studies was established, I identified the area of focus of these studies, which was directly informed by the gaps in the literature. Upon identifying the missing links in the literature, I recognised the need to conduct two preliminary studies. The first was a systematic review and meta-analysis on using DMT to treat common symptom clusters in TRD (Christopher et al., under review). The second was a survey study collating practice-based knowledge on how dance movement therapists practiced with their clients with TRD (Christopher & Tamplin, 2022). While the availability of funding and human resources may directly affect the type of preliminary studies that can be carried out, it is unlikely that preliminary studies can be avoided altogether in novel research areas.
STEP 3: Integrating Existing and New KnowledgeIntegration is the central action in this third step of creative problem solving. Here, I asked myself the following questions:
How can I integrate new and existing information on this topic? and
How does the integrated information inform the intervention session plan?
Using the study by Shim et al. (2021) as a guide, I integrated the findings of both my preliminary studies and my clinical practice experience using Watson’s (2020) technique of braiding (the findings have been schematically shown in Fig. 2). Braiding was a suitable option as it can combine more than just quantitative or qualitative data. Instead, braiding draws on visual, temporal, and sensorial integrations and is not bound to any one step in the research (Watson, 2020). Although braiding is typically used when two or more methods are sequentially employed across different research phases, I adapted this technique. I used it across different studies to suit my research needs. Watson (2020) also recommends a creative review process that usually has an exegetical output. This process can also be understood from the lens of arts-based research. Here, the words of Hervey (2004) stating “the phenomena of the arts must be allowed to speak for themselves within their unique environments (p. x)” perfectly encapsulated my rationale for the engaging in dance as my creative exegesis, which I termed ‘dancing with the data’ in my research. Through this artistic process, I processed and reviewed the insights from the preliminary studies on a somatic level. I involved the participation of another dance/movement therapist (one of my PhD supervisors, Dr Ella Dumaresq) in this step, who is referred to as the observer below. My rationale for inviting another DMT into this artistic process was similar to what (McNiff) recognises about artistic inquiry being both, subjective but also needing external perspective and potential objectivity (2008). In my case of ‘dancing with the data’, the DMT played the role of the observer bringing to my attention new considerations for movement explorations based on their observations.
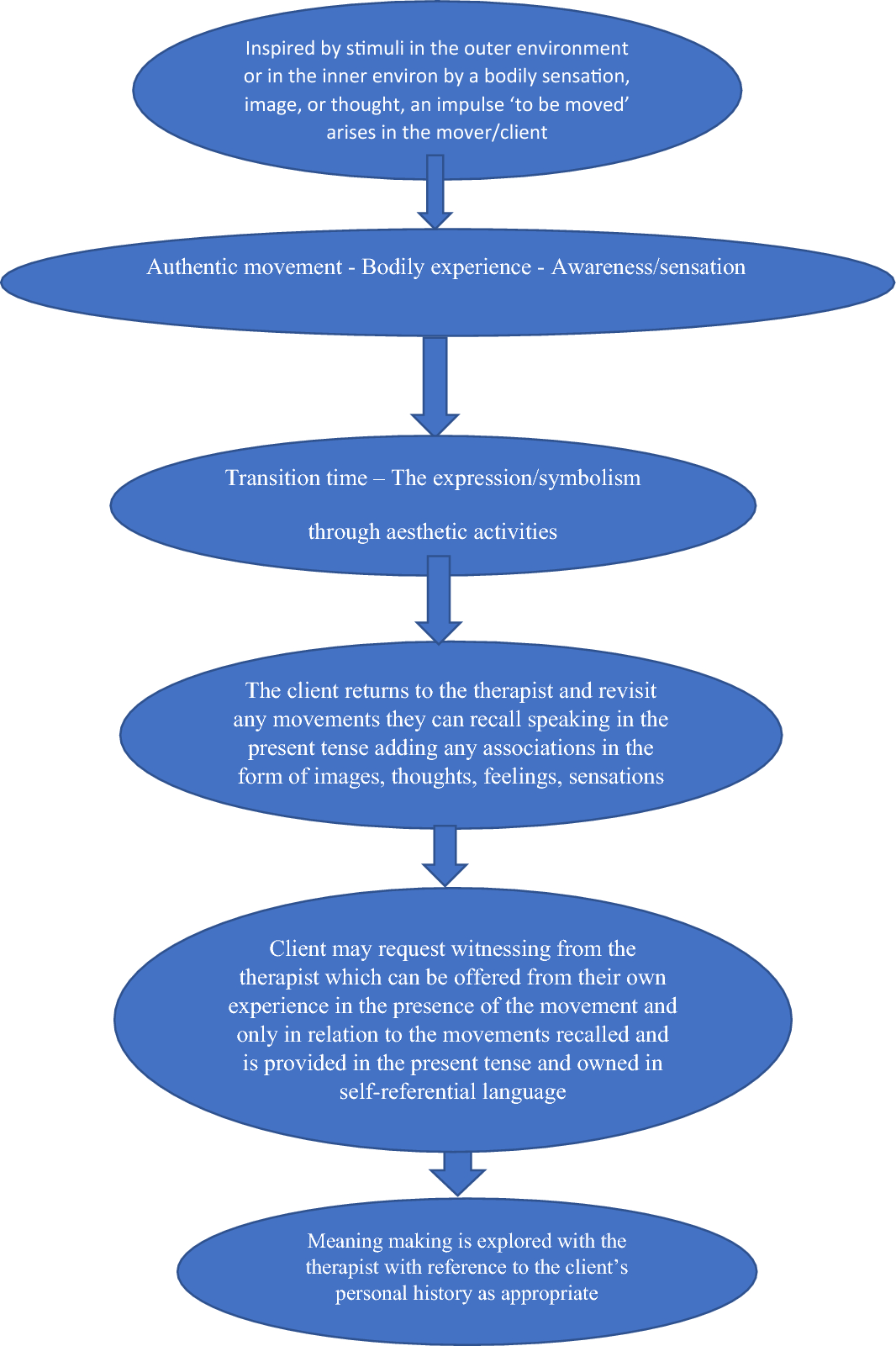
Fig. 2
The braiding process contributing to the development of the intervention session plan. As stated, the figure begins at the bottom and is designed to be reviewed vertically (bottom-to-top)
Steps:
1.I reviewed the findings of the systematic review (the first preliminary study in this research project), after which I:
(i)Noted down the words that described or alluded to different dance/movement therapy techniques from the systematic review findings. (E.g. improvisation, active choice-making, collaboration, props, etc.).
(ii)Wrote down all words that warranted consideration regarding study design (e.g., standard care, 12 weeks, 16 weeks, attrition, etc.).
(iii)Read the written words and used these as a prompt for an initial dance exploration, ‘Dancing with the Data-1’ while being witnessed by another dance/movement therapist.
2.Repeated steps (i), (ii), and (iii) with a second dance exploration, which I termed ‘Dancing with the Data-2’ after reviewing the findings of the survey study (the second preliminary study in this research project).
3.The observer shared verbal feedback on any repetitive or striking movement patterns they saw in steps 1 and 2.
4.I then danced in response to the verbal feedback from the observer. This was termed ‘Dancing with the Data-3’.
5.Lastly, after my final movement exploration (which I termed ‘Dancing with the Data-3) was complete, I reflected on ‘Dancing with the Data 1, 2, and 3’ and made a note of the following:
(i)Any movement-based need I noticed in myself (that may be a consideration for the dance therapy session plan within the broader protocol).
(ii)Any standard DMT techniques I noticed across ‘Dancing with the Data 1, 2, and 3.’
In this novel research, the benefit of using braiding and creative exegesis was that it helped centralise multiple research outputs (Watson, 2020, p. 77). The multiple research outputs obtained from step 5 (as mentioned above) were then ‘braided’ to form the outline of the intervention session plan. This has been schematically depicted below (Fig. 2).
STEP 4: Reviewing OutputsMaintaining the fidelity of an intervention is part of the ethical duty of care. Since this manner of session plan development involves integration between varied facets, such as the researcher’s self, research paradigm, existing knowledge, and findings from preliminary studies, it was necessary to check my implicit biases that may have clouded my four-step process. I did this by asking the following questions:
Does this session plan directly answer the research question? and,
Is there a clear rationale for each component of the intervention?
If yes, Can I ascertain the links between the preliminary studies, existing literature, and my intervention session plan?
If not, What changes do I need to make to ensure the intervention is built on practice knowledge, new knowledge, and principles of DMT?
A fidelity check may also help maintain the internal validity of the intervention. Here, I sought a ‘content fidelity check’ by one of my supervisors, who read the intervention session plan and provided narrative feedback on the following: (i) any concerns regarding biased use of language and misalignment between the planned intervention session plan and research question of the project, (ii) DMT recommendations in the context of emergent literature on related topics, and, (iii) any further recommendations to enrich research integrity and reduce confirmation or publication biases, if relevant. In some instances, developing an implementation fidelity checklist may also be relevant. In my research, I developed an implementation fidelity checklist adopted from Rolvsjord et al. (2005) framework for research rigour in music therapy, which included four main categories: (i) Essential and Unique, (ii) Essential and Not Unique (iii) Acceptable but not Essential and (iv) Unacceptable. I designed this checklist to be completed after each intervention session of the research project. This also served as a documentation format for any patterns of deviation that emerged during implementation. Any patterns in deviation may also be considered formal inclusions in a second iteration of the intervention session plan if there is one.
Engaging in the aforementioned steps re-emphasised the need for resourceful problem solving while developing a novel intervention session plan, particularly the importance of drawing on multi-faceted resources and forms of knowledge beyond academic literature. Further, recognizing my clients’ lived experiences and insights from clinical practice as core forms of knowledge is also symbolic of the mindset of integration. This was seen in the process of braiding (Watson, 2020) which enabled me to interweave multiple facets of information (cognitive, emotional, sensorial, etc.) that helped me obtain the outline of the intervention. This four-step process helped me navigate the muddy waters of novel research by prioritizing research integrity and personal reflexivity. Having discussed this process, I will present the DMT session plan from the 12-week intervention session plan developed through the abovementioned processes. The following session plan was implemented with one group of five adults with treatment resistant depression (n = 5) between the ages of 20 and 30 with two individuals who dropped at week 6 and 9. All individuals volunteered to participate in a research study, with results to be published in an upcoming companion paper. Individuals were eligible to participate if they fulfilled all the following criteria: (i) have a diagnosis of clinical depression that has either lasted at least 18 months or have been identified to have ‘treatment resistance’ by a medical professional (ii) lived independently (not in an assisted facility) (iii) were between 21 and 50 years of age (iv) did not experienced a significant reduction in symptoms despite engaging in treatment for at least 6 weeks (i.e., antidepressants, or 1:/group psychotherapy) (v) did not have any other illness that requires urgent and persistent medical care (vi) were willing to participate in a 16-week group DMT study (vii) were comfortable with communicating in English (writing, reading, and comprehension) (viii) were not at risk of active self-harm. Further details like exclusion criteria, additional demographic details etc. will be published in an upcoming companion paper.
留言 (0)