Hereditary angioedema (HAE) is a rare, debilitating, and potentially life-threatening autosomal dominant disease [1, 2]. The majority of patients with HAE have either a deficiency in C1-esterase inhibitor (type I) or dysfunctional C1-esterase inhibitor (type II), resulting in dysregulation of the kallikrein–kinin pathway and overproduction of bradykinin, which leads to unpredictable episodes of increased vascular permeability, extravasation, and subsequent angioedema attacks [2,3,4]. These intermittent attacks involve cutaneous and mucosal swellings that may affect the extremities, face, larynx, gastrointestinal tract, or genitourinary area [2]. Abdominal symptoms including pain, nausea, diarrhea, and vomiting occur frequently [1]. Laryngeal swelling occurs infrequently but makes asphyxiation an omnipresent risk for patients with HAE [5, 6].
The disease burden extends beyond the frequency and severity of attacks, as a result of interference with activities of daily living, emotional disturbance, and the need for lifestyle modification. Physical functioning may be limited during attacks, restricting participation in work and social activities [7]. Anxiety and depression are common between attacks, due to fear of the next attack and uncertainty regarding the severity of future attacks [8]. Thus, HAE interferes with health-related quality of life (HRQoL) both during and between attacks [7]. Several recent publications have noted the overall disease burden and adverse effects on quality of life associated with HAE and the unmet need for more effective treatment [9, 10].
According to international (World Allergy Organization/European Academy of Allergy and Clinical Immunology) guidelines, the goals of treatment of HAE include achieving complete control of the disease, which for patients means absence of all attacks and normalization of quality of life; the guidelines stipulate that this can only be realized with long-term prophylaxis (LTP) [11]. Hence, LTP is a critical part of pharmacological care for patients with HAE [2, 11]. Treatment guidelines from the US Hereditary Angioedema Association (HAEA) advisory board also recognize that further advancements with novel long-term prophylactic treatment options for HAE (namely C1-esterase inhibitor SC [human], lanadelumab, and berotralstat) have led to a shift in the paradigm of care, with the ability to achieve the realistic treatment targets of reducing the frequency and severity of attacks [2].
C1-esterase inhibitor SC (human), a plasma-derived concentrate of C1-esterase inhibitor (human) for subcutaneous administration twice weekly [12]; lanadelumab, a human monoclonal antibody inhibitor of plasma kallikrein administered subcutaneously once every 2 or 4 weeks [13]; and berotralstat, an oral plasma kallikrein inhibitor administered once daily [14], are currently recommended as first-line LTP in the international guidelines [11]. All three agents provide protection from HAE attacks versus placebo in randomized controlled trials, with sustained long-term prophylactic effects [13, 15,16,17]. By comparison, LTP available prior to the introduction of these agents mainly consisted of attenuated androgens and intravenous C1 inhibitor concentrate administered twice weekly. Although androgens do prevent HAE attacks, they are commonly associated with side effects including virilization, menstrual disorders, and amenorrhea in women, as well as weight gain, headaches, myalgia, depression, and drug interactions [11, 18]. Treatment with intravenous C1 inhibitor concentrate was burdensome and often led to vein fatigue [19]. Patients with HAE not taking LTP have typically relied on on-demand therapy when an HAE attack occurs [2, 11].
In Phase 3 clinical studies of these novel agents, the reported reduction in HAE attacks and the proportion of HAE patients who were attack free were different for different agents, which might be due to differences in study designs, patient populations, and durations of follow-up. There was a 95.1% median reduction in HAE attacks compared with placebo over 16 weeks in the Phase 3 study for C1-esterase inhibitor SC (human) based on the recommended dose of 60 IU, with 40% attack free during this time [16]. In the 26-week pivotal Phase 3 lanadelumab study, the mean reductions in HAE attacks were 87% or 73% compared with placebo for the recommended 300 mg dose given every 2 or 4 weeks, respectively. Approximately 44% or 31% of patients on the 300 mg dose given every 2 or 4 weeks, respectively, were attack free during the 26-week treatment period, compared with 2.4% of placebo-treated patients [20]. For berotralstat, in the pivotal Phase 3 study at the recommended dose of 150 mg daily, the mean reduction in HAE attacks compared with placebo was 44.2% over 24 weeks [17]. The proportions of patients attack free over the 24-week treatment period were no different in the berotralstat- and placebo-treated groups [17]. A recent real-world study found that use of novel LTP was associated with a 77% reduction in the number of attacks each year compared with those who used only on-demand treatment [1].
Older agents such as attenuated androgens and antifibrinolytic agents are recommended as second-line LTP, for use only when first-line medications are not available. With the availability of novel LTP with greater efficacy and fewer adverse effects compared with androgen therapy, guidelines are focused on reducing the burden of illness due to HAE, which can be achieved by further reducing the frequency of HAE attacks and enabling patients with HAE to experience the same HRQoL as people without this condition [2, 11].
Several disease-specific and generic patient-reported outcome tools are available to evaluate HRQoL for HAE. The Angioedema Quality of Life Questionnaire (AE-QoL) [21, 22] was the disease-specific patient-reported outcome measure included in the development programs for all three novel LTP therapies [8, 23,24,25]. Although not specific for HAE, it has been validated as a reliable instrument for measuring HRQoL in adult patients with HAE [26]. Reductions in HAE attacks mean that patients may be attack free for more time, which has the potential to improve their HRQoL. A survey of 737 patients with HAE who were members of the US HAEA, conducted by Castaldo et al. [1], showed that median AE-QoL scores for those who had been attack free for 3 months were better than for those who were attack free for only 1 month before completing the AE-QoL. Those on any LTP experienced better QoL than those using only on-demand treatment. In the clinical development programs for the novel prophylactic agents, the relationship between AE-QoL scores and time attack free was not reported in any of the studies apart for an open-label extension study for lanadelumab [20], which showed that most of the improvements in AE-QoL scores were observed during the early follow-up period (day 0 to day 56) and then reached a plateau; the scores were maintained during subsequent visits.
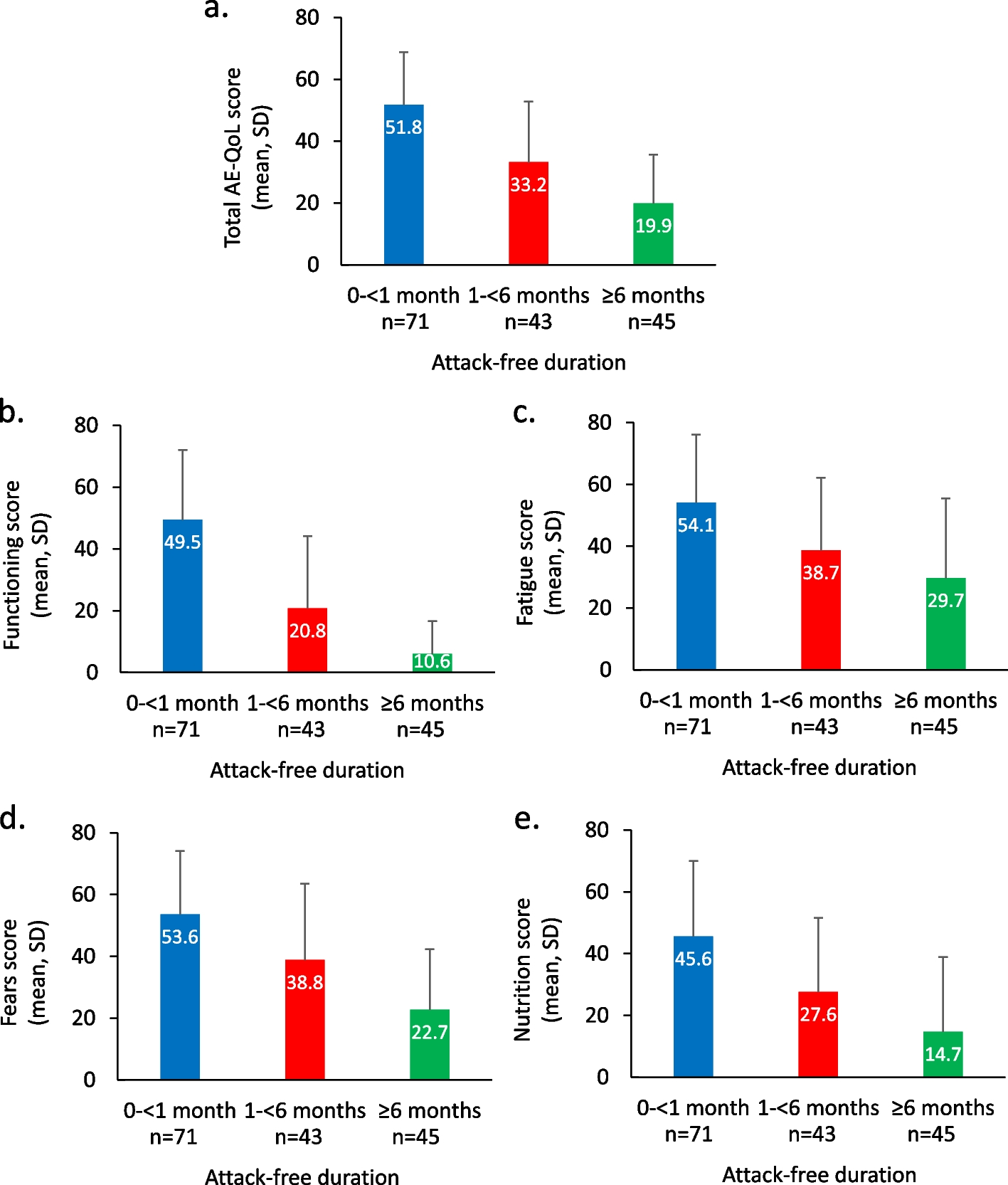
Here, we sought to further build on the earlier research of Castaldo et al. [1] and evaluate the real-world benefits of LTP over a longer time period. Jean-Baptiste et al. have recently evaluated the symptom experience of HAE patients and concluded that more research is needed on the effect of longer attack-free durations on HRQoL [27]. Using data drawn from a wide-ranging survey of members of the US HAEA and Hereditary Angioedema International (HAEi), we examined the relationship between duration of time attack free, and HRQoL, exploring the possibility that there is an association between observed improvement in HRQoL and attack-free duration.

留言 (0)