Neurofibromas are common benign tumors that originate from Schwann and mesenchymal cells that constitute the nerve sheath [2, 3, 8]. The head and neck are commonly involved because of the rich innervation of this area [7, 9]. Neurofibromas of the oral cavity often affect the trigeminal and upper cervical nerves, most of which appear in superficial soft tissues such as the tongue, buccal mucosa, gingiva, salivary glands, and palatal mucosa [2, 3, 8, 9]. Neurofibromas occurring in the bone are rare because the bone marrow space lacks nerve sheaths or myelinated nerves [6,7,8,9,10]. Oral intraosseous neurofibromas primarily originate from the superficial mucosa, while involvement of deeper locations resulting in bone absorption is commonly associated with subperiosteal neurofibromas [10,11,12]. Only a few cases of solitary intraosseous neurofibromas of the oral cavity have been described in the literature, with those in the mandible being the most common location owing to the presence of a major nerve bundle, namely, the inferior alveolar nerve [6,7,8,9,10,11,12]. This relative rarity of solitary intraosseous neurofibromas of the maxilla is exemplified in a review by Sharma et al., wherein of the 22 cases in their series of solitary neurofibromas involving the jawbone over the last two decades, only four were neurofibromas of the maxilla [13]. Therefore, solitary intraosseous neurofibromas of the hard palate are extremely rare, as was observed in the present case. Given its rarity, clinicians may not be familiar with intraosseous neurofibromas and therefore fail to consider it as a differential diagnosis. Herein, the reported cases of solitary intraosseous neurofibromas located in the maxilla published in the English literature until 2023 [7, 12, 14,15,16,17,18,19,20] were compiled to assist in diagnosis. The information presented in Table 1 (at the end of the document text file) is extracted from these cases.
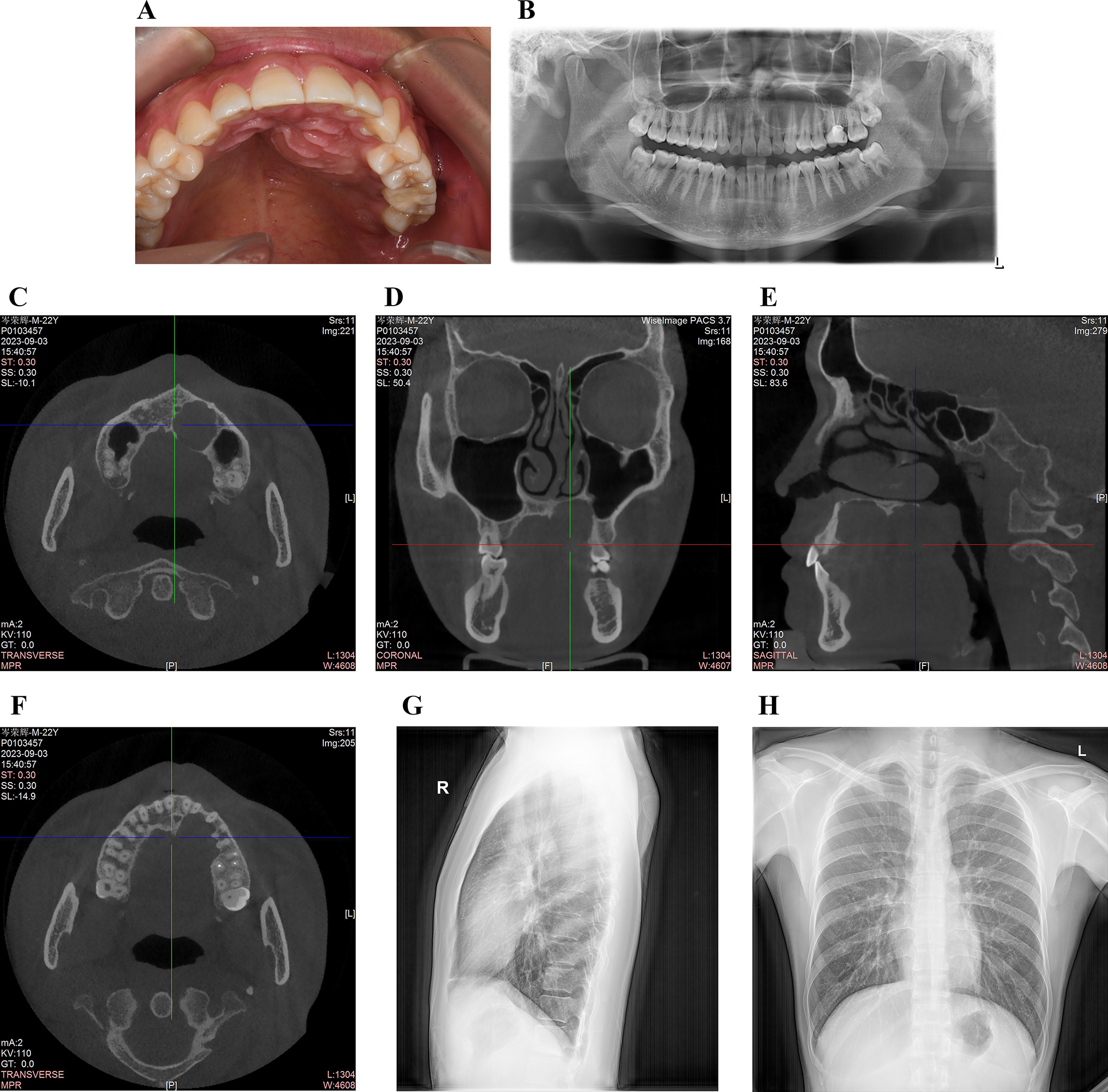
Table 1 Summary of reports of solitary intraosseous neurofibromas in the maxillaOnly nine cases of solitary intraosseous neurofibroma in the maxilla have been previously reported, with the patients having an average age of 22.2 years. Similar to most cases that show a slight male predominance, the present case was male. Clinically, solitary neurofibromas typically occur as asymptomatic painless lesions in the initial stages. The current patient was asymptomatic and did not show any pain or neurological disturbances, similar to previously reported cases [12, 15,16,17,18,19]. On radiography, cortical expansion, cortical perforation, tooth displacement, and root resorption are observed in most cases [7, 12, 14,15,16, 20]. Cortical expansion and perforation were observed in the present case; however, displacement of the tooth or root resorption was not observed. Some studies have reported a well-defined unilocular radiographic appearance of the lesion, which was also observed in the current case [7, 14, 20].
However, a definitive diagnosis is challenging for clinicians because of nonspecific clinical and radiographic symptoms and the variety of differential diagnoses, including odontogenic cysts, odontogenic keratocysts, unicystic ameloblastoma, vascular anomalies, salivary gland tumors and other benign soft tissue tumors. Odontogenic cysts, which commonly occur as periapical cysts, are associated with infected pulpal tissues. Odontogenic keratocysts, often seen in the mandible, exhibit severe resorption of the adjacent tooth roots.
Unicystic ameloblastoma is a variant of ameloblastoma that presents as a cyst and shares clinical and radiological features with odontogenic cysts. They appear as well-circumscribed unilocular radiolucencies that often surround the crown of an impacted tooth [10]. In the present case, the teeth that were in direct contact with the neoplasm did not exhibit pulpitis, remarkable root resorption, impaction or other specific abnormalities, which is not in favor of an odontogenic cyst, odontogenic keratocyst or unicystic ameloblastoma. Vascular anomalies involving the facial skeleton are relatively uncommon. They often exhibit characteristic features, such as a sunburst, radiating spoke wheel, or reticular or soap bubble appearance in radiology [21]. Besides, a previous study indicated that the imaging characteristics of diffuse and plexiform neurofibromas can be easily confused with those of vascular anomalies, potentially leading to an incorrect diagnosis [22]. Three types of neurofibroma have been described: localized, diffuse, and plexiform [2, 22]. The solitary neurofibroma analyzed in this study appeared as a localized mass of hard palate with well-defined borders, which is not in favor of vascular anomalies. However, the possibility of salivary glands and other benign soft tissue tumors cannot be excluded. Ultrasound and magnetic resonance imaging (MRI) are valuable tools for identifying a soft-tissue mass, classifying lesions and determining the extent of the lesions [22]. Therefore, the use of MRI or oral ultrasound can help diagnose this solitary neurofibroma. In cases of persistent uncertainty, local organizational biopsy or fine-needle aspiration cytology is preferable to achieve an accurate preoperative diagnosis, with a definitive diagnosis relying on histopathological and immunohistochemical findings [12, 19]. Preoperative biopsy or fine-needle aspiration cytology were not performed for this patient since the present neoplasm appeared more likely to be benign based on preoperative clinical examination and radiographic findings.
In the present case, the lesion was successfully removed without any obvious complications. Complete surgical excision of this lesion could mainly be attributed to the presence of a complete capsule, which indicates that setting the resection margin is easier compared with most solitary non-encapsulated neurofibromas [3,4,5,6, 10, 13, 14]. Previous studies have reported that gross specimens of neurofibroma tissue appear to have a doughy consistency with a whitish and shiny surface [4, 19], which were observed in the current case. Microscopically, spindle-shaped cells with elongated, thin nuclei and scant cytoplasm surrounded by a collagenous matrix were appeared in this specimen sections. There was no salivary gland or salivary canal. These microscopic examinations can be excluded from many other diseases, especially salivary gland tumors, but differential diagnosis remains difficult to make with some soft tumors such as schwannomas. In addition to above cell arrangements, immunohistochemical findings revealed spindle-shaped cells were positive for S-100 and CD34. The S-100 protein is a useful marker for indicating a neural origin tumor [3, 4, 12]. CD34 located in the cell membrane and cytoplasm is expressed in neurofibromas but not schwannomas [3, 10].
The clinical behavior of neurofibromas is characterized by a benign course with a low frequency of recurrence after surgical excision, primarily because of the absence of a complete capsule [2,3,4,5,6, 23]. The local recurrence rate of this condition may be lower due to the appearance of an intact envelope. Furthermore, the risk of malignant transformation of neurofibromas is between 5 and 10%, especially for NF-1 [2, 3, 6, 10, 18]. In the present case, the tumor was an isolated intraosseous entity that was not associated with any systemic pathology and seldom changed into a malignant form. However, it is important to consider that solitary intraosseous neurofibroma may be an initial manifestation of NF-1 [8, 12] with no family history, but it can be caused by a spontaneous mutation [23, 24]. There are no distinctive features between solitary and multiple forms apart from systemic and hereditary factors; if possible, genetic studies to rule out common autosomal genetic disorders are recommended [19, 24]. Fortunately, Ki-67 staining, indicating the potential for aggressiveness and malignant transformation [3, 25], was found to be weak upon immunohistochemical analysis, and it showed no clinical features of invasion owing to the presence of an intact capsule. However, sufficient follow-up and tracking is required. We conducted clinical follow-up for the past 9 months; there were no signs of malignant transformation, recurrence or clinical manifestations of NF-1 in the present patient.
In conclusion, the present case of a single neurofibroma involving the maxillary bone with a complete envelope is extremely uncommon. The preoperative diagnosis of a solitary intraosseous neurofibroma is challenging because of its rare location and nonspecific radiographic and clinical characteristics. Histopathological analyses supported by immunohistochemistry are essential for the correct diagnosis of these rare entities. Genetic studies are required to rule out genetically inherited diseases, when possible. A longer follow-up period is required because of the potential for local recurrence and malignant transformation of these tumors.








留言 (0)