Agenesis of the kidneys, hemivaginal obstruction, and uterus didelphys are the three features of the uncommon congenital condition known as HWWS [10, 11]. It is most commonly diagnosed in puberty due to dysmenorrhea, vaginal discharge, pelvic or abdominal pain, but more rarely, it can present in neonates or adults with primary infertility, pyometra, urinary obstruction, and ischiorectal swelling [8, 12]. Because of the low incidence of HWWS and the lack of specificity of clinical symptoms, it is easy to miss diagnose and misdiagnose, resulting in endometriosis, pelvic adhesion, infertility, and other complications [8].
Communication may exist between the obstructed and contralateral sides. In this study, communicant HWW syndrome was more common (68%) than noncommunicant HWW syndrome (32%). An ultrasound or an MRI is not very sensitive to detecting communications in the vagina, especially small holes. One study showed that MRI could identify only 20% of communications [13]. In fact, the presence, location, and quantity of communication and ectopic ureter insertion into the ipsilateral obstructed hemivagina are mainly determined by careful examination with hysteroscopy. In our study, there were 27 patients with no communication between the uterus and vagina, 38 patients with communication in the vaginal septum, 18 patients with communication in the cervix, and 2 patients with communication both between the vaginal septum and cervix. And one patient had three small holes in the vaginal septum. Earlier literature [14, 15] reported HWWS to be more common on the right than on the left, with a ratio of 2:1 [16], whereas our study found it to be 1.4:1.
Several non-specific manifestations of HWWS occur after menarche or around that time. Whether the vaginal oblique septum was completely or partially obstructed affected the clinical presentation. There was a younger onset age for noncommunicant HWW syndrome (14.2 years) than for communication (18.3 years), which was in accordance with the literature [17, 18]. Complete obstruction is characterized by dysmenorrhea shortly after menarche and hematomatre caused by the hemivagina obstruction, while incomplete obstruction is characterized by abnormal vaginal discharge, such as blood or pus. Asymptomatic conditions are more common in patients without obstruction, which may be explained by the menstrual blood discharged through communication.
In Sampson’s opinion, retrograde menstruation and implantation account for most cases of endometriosis. An earlier study found that 19% of HWWS patients had pelvic endometriosis [19] and that the rate of endometriosis was higher among patients with complete obstructions than among those with incomplete obstructions, suggesting that the obstructed hemivaginal septum was the direct cause of endometriosis. Endometriosis can be diagnosed early, especially in adolescents, to prevent further disruption of the normal anatomy and fertility loss. Endometriosis is associated with an obstructive genital anomaly found in adolescents, for which the severity depends on the delay in establishing the diagnosis. These lesions may regress spontaneously, sometimes completely, when the anomaly has been surgically treated [20].
There are some uterine malformation variants of HWWS, including the didelphys uterus, septate uterus, bicornuate uterus, and bicornuate and complete septate uterus. Most cases of HWWS were of the didelphys uterus, a classic variety of uterine deformity, according to L. Fedele et al. [9]. Our findings support and expand on earlier research. There are different surgical options for different uterine malformation variants, which may be related to conceiving or maintaining a pregnancy in the future. A didelphys uterus has not been associated with infertility or pregnancy complications, and surgical intervention is not routinely recommended [21]. In contrast, for a septate uterus, pregnancy outcomes are significantly improved after uterine septum resection [22].
Anomalies of the kidney are connected to ipsilateral obstructive Müllerian abnormalities in around 50% of cases [23]. The right side is where kidney abnormalities are more common [24, 25], which is consistent with our findings. Kidney abnormalities include renal agenesis, renal dysplasia, renal hypoplasia, duplicated kidneys, and multicystic dysplastic kidneys, according to earlier reports [25,26,27]. In our study, we discovered ipsilateral renal agenesis, ipsilateral dysplastic kidneys, and the bilateral presence of normal kidneys. Regarding the urinary system, in some HWWS cases, attention should be given not only to the renal abnormalities but also to the existence of ureteral remains. Cystoscopy is required when imaging points to the existence of ureteral remains. A case of HWWS with left renal dysplasia and a left ectopic ureter connecting with the vagina was described [28]. Adi et al. [29] described a case of HWWS with a urethrovaginal fistula. We found ectopic vaginal ureteral ending in 4 cases. It could be argued that the primary movements in the embryogenesis of this malformation is a unilateral anomaly of incorporation of the distal part of the wolffian duct within the presumptive bladder. Because of close relations between wolffian and müllerian ducts in this region, this may lead to anomalies of the unilateral müllerian duct, leading to anomalies in fusion processes of the both müllerian ducts [26, 30, 31]. Moreover, the wolffian anomaly of incorporation may also induces an anomaly in the incorporation of the ureteric bud within the presumptive bladder [30]. There is no doubt that the presentations of the urogenital malformations in HWWS are diverse.
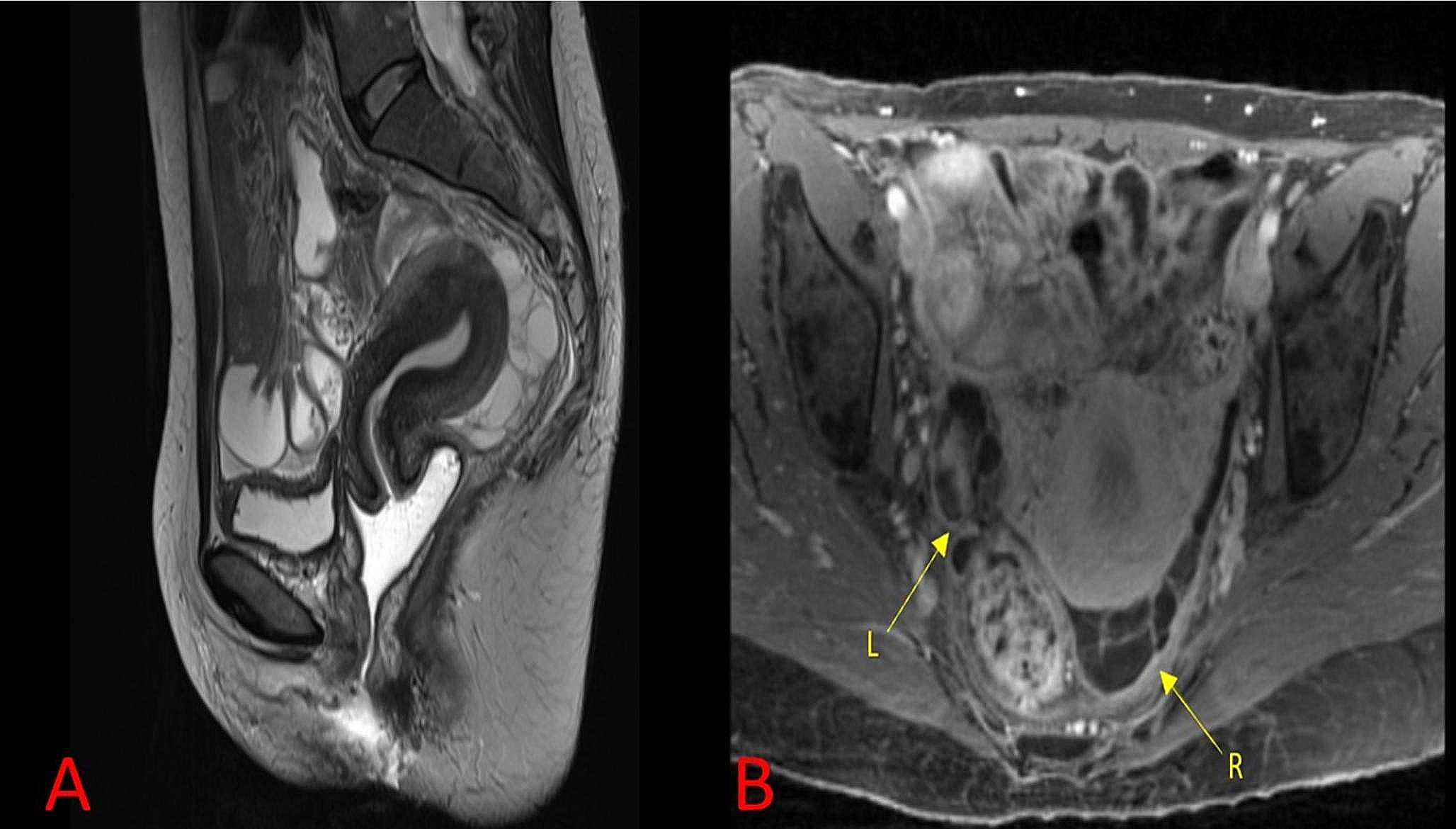
Ultrasound has traditionally been the first imaging modality chosen for the diagnosis of HWWS because it is affordable, doesn’t expose users to radiation, and provides better images of the uterus and adnexa [32]. In recent years, 3D ultrasound has become the method of choice for the diagnosis and assessment of congenital uterine anomalies [33]. MRI is currently regarded by several writers as the gold standard for HWWS diagnosis and surgical planning [34]. The goal of surgery is to remove the oblique vaginal septum, observe whether there is a fistula, and rule out any further problems. Total excision of the vaginal septum is the most important treatment for HWWS. MRI has excellent soft tissue resolution and a broad imaging field of view and is able to evaluate uterine malformations, hematocolpos, hematometra, hematosalpinx, and ovarian or pelvic endometriosis by imaging in different orientations, dimensions, and parameters, which is of great significance for early clinical diagnosis and treatment [35, 36]. Since MRI is the best imaging modality for endometriosis, the relationship between HWWS and endometriosis also favours this condition [35]. It is important to note that CT is not the first option for female pelvic examination, but it may still be utilised as an emergency examination for patients with severe lower abdomen discomfort if the ultrasound diagnosis is unclear and the MRI examination takes a long time [32].
When adolescent girls come to the emergency room with an acute abdomen, appendicitis, hymen atresia, and adnexal torsion are indeed the main causes of predisposition and diagnosis [30]. But the presence of HWWS should be considered when renal agenesis is found during systematic abdominal and gynecologic examinations completed by radiologic evaluation. In addition, we should take into account the occurrence of HWWS merging these situations. Patients who have both HWWS and hymen atresia frequently overlook HWWS because the acute obstructive symptoms brought on by hymen atresia conceal those brought on by the oblique vaginal septum, and the obstructive symptoms are much diminished following the release of hymen atresia.
Clinicians are not fully aware of HWWS since it is rare and has unusual clinical presentations. Some patients with HWWS delay seeking medical attention, and HWWS is discovered only when infertility occurs. Such patients are vulnerable to misdiagnosis and missed diagnosis because they ignore their own clinical signs. Even after menstruation, HWWS is frequently misdiagnosed. Several reasons may justify the delayed symptoms: first, the vagina can accommodate a large volume of blood due to its distention properties; second, some of the blood is absorbed between menses [32]; third, oral contraceptives and anti-inflammatory drugs are generally recommended to relieve dysmenorrhea [37, 38]; and finally, some patients who present with isolated vaginal discharge are mistakenly treated with long-term antibiotics.
Herlyn-Werner-Wunderlich syndrome is an exceedingly uncommon conglomeration of congenital anomalies. Timely and efficacious surgical intervention will undeniably enhance quality of life, avert complications, and maintain long-term fertility. A comprehensive preoperative evaluation of obstruction is pivotal in determining the most advantageous surgical methodology. A robust association is evident between the existence of complete obstruction and symptoms, age at symptom onset, and diagnosis. Additionally, careful consideration should be given to the height of communication in the hemivagina, with symptoms manifesting at an earlier stage when the obstruction is higher, as menstrual blood drainage from a high communication is not as smooth as from a low one. Further work is needed to determine whether the level of communication will affect the onset and seriousness of clinical manifestations.
Limitation
There were some limitations in our study. Our study was a single-center retrospective study in which a relatively small number of patients were included. In addition, Some cases were diagnosed and treated many years ago. Therefore, a surgical approach could vary not only due to anatomical differences, but also due to medical advances and the possibility of delayed diagnosis. Further studies are required to avoid selection and observational bias, and long-term prospective or randomized control trials are necessary to provide optimal clinical evidence to better manage this disorder.








留言 (0)