
記住我




Malakoplakia is an exceedingly rare inflammatory disorder of unknown incidence with approximately 700 cases identified in the literature. It can present with genitourinary, gastrointestinal, or cutaneous manifestations [1]. With renal involvement, patients often have E. coli pyelonephritis and acute kidney injury [2]. While E. coli is frequently associated with malakoplakia, other gram-negative, gram-positive, and mycobacterial organisms have also been isolated [3]. Malakoplakia occurs most often in patients with weakened immune systems secondary to diabetes, neoplastic disease, autoimmune disease, organ transplant, immunosuppressive therapies, or alcohol use [1, 4]. It is believed to result from a defect in macrophage phagocytic function leading to a diminished bactericidal response [5]. When bacteria are phagocytosed, they are not fully “digested” by macrophages which leads to accumulation of intracellular debris. This in turn triggers a granulomatous reaction [4]. Histologically, this appears as macrophage infiltrates with cytoplasmic inclusions known as Michaelis-Gutmann bodies, the pathognomonic finding in malakoplakia [1, 5]. CD68 and CD163 immunostains confirm the histiocyte lineage, and kidney biopsy typically shows interstitial inflammation with fibrosis and tubular atrophy [6, 7]. Treatment consists of a prolonged course of antibiotics with high intracellular penetration; if medical management is unsuccessful, surgical resection may be required.
ObjectiveTo highlight malakoplakia as showcased in a young immunocompetent patient, to discuss the pathological findings indicative of malakoplakia, and to review available therapies.
Case reportA 32-year-old woman with history of recurrent urinary tract infections, Raynaud’s phenomenon, and prior COVID-19 infection presented to the emergency department with lower extremity weakness and 2 days of dyspnea. One week prior, she had experienced symptoms consistent with a UTI but did not pursue testing or treatment. On presentation, she reported nausea, vomiting, fatigue, difficulty walking, and ascending paresthesia in her distal legs. She was afebrile with blood pressure 62/38 mmHg, heart rate 106, and respiratory rate 24. Abdominal examination was notable for hepatomegaly and masses attributed to nephromegaly. A diffuse petechial rash was present, and neurologic exam noted 4/5 strength in the bilateral lower extremities with absent deep tendon reflexes throughout. Although fully alert and oriented on presentation, she became progressively altered. Labs were notable for leukocytosis (WBC 22.22 K/UL), anemia (Hgb 8.0 g/dL), thrombocytopenia (PLT 18 K/UL), elevated inflammatory markers, and kidney failure (creatinine 6.4 mg/dl) with profound hyponatremia and hypokalemia. Blood and urine cultures grew Escherichia coli.
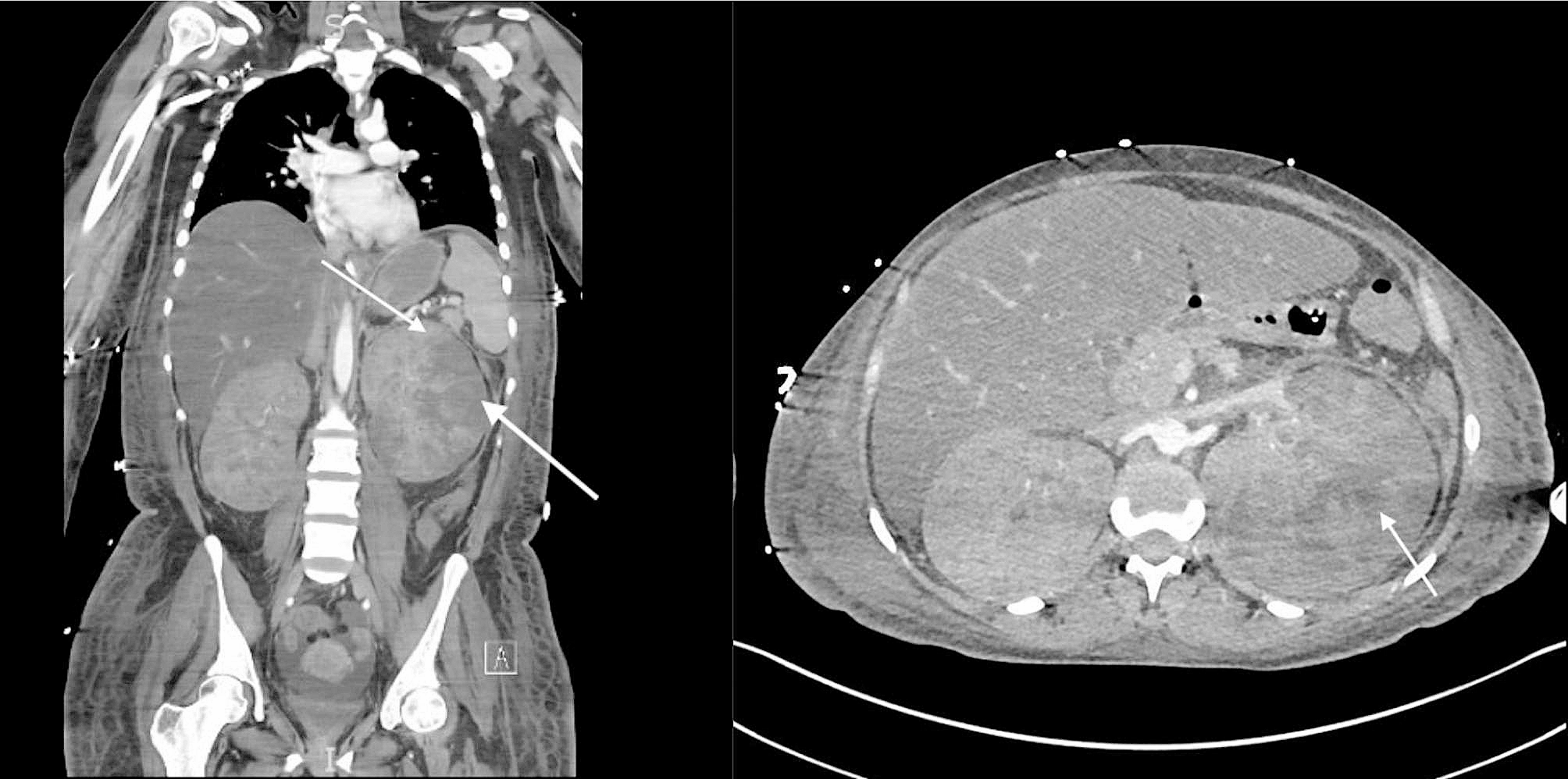
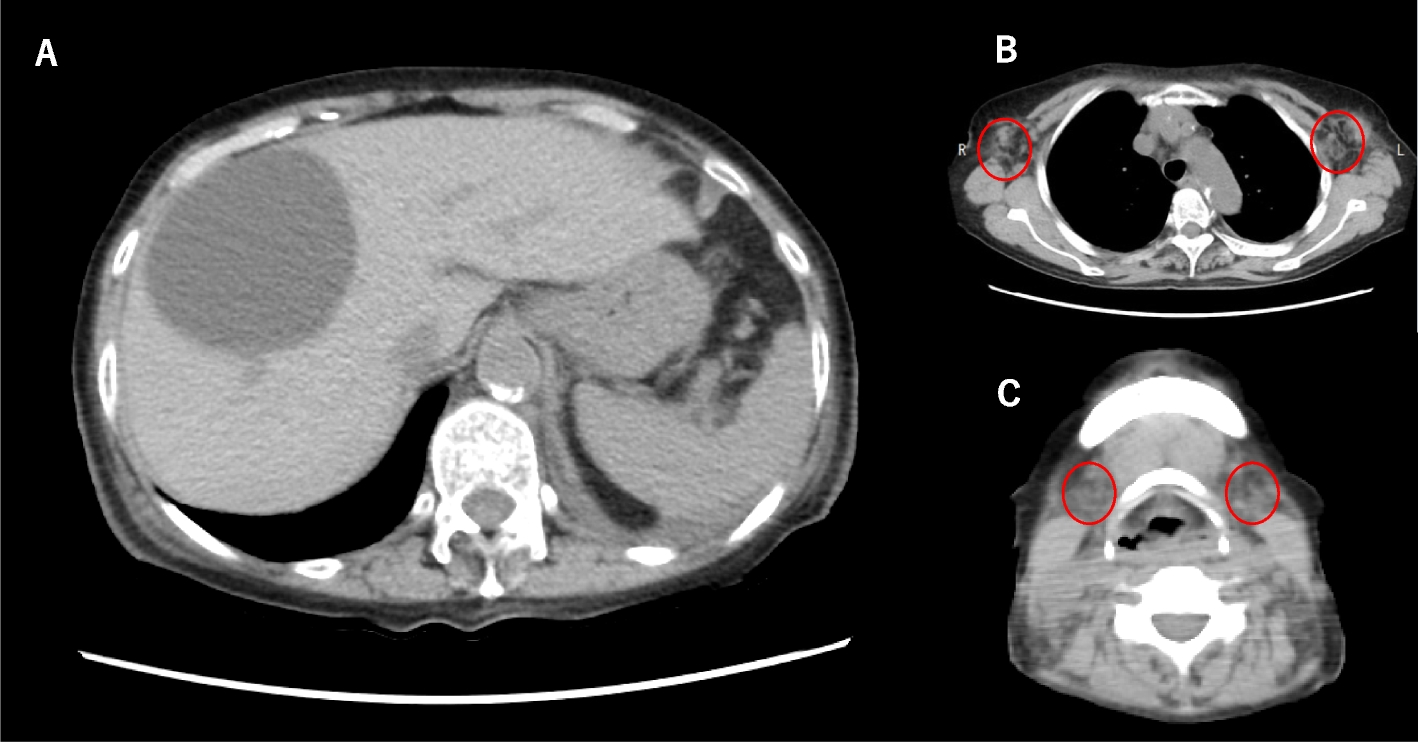
Computed tomography scan of the abdomen/pelvis with intravenous contrast revealed massive bilateral kidney enlargement without nephrolithiasis, as well as hepatomegaly (Fig. 1). Initial imaging noted concern for renal vein thrombosis, but no thrombus was seen on subsequent duplex ultrasound. MRI brain and lumbar puncture were performed due to altered mental status and were normal. Despite broad-spectrum antibiotics, her clinical condition rapidly deteriorated, requiring escalating vasopressor support, intubation, and initiation of continuous venovenous hemodialysis (CVVHD).
Fig. 1
Computed tomography scan of the abdomen/pelvis with intravenous contrast. Massive nephromegaly is present with areas of hypoperfusion and/or infarct (arrows)
Given the patient’s worsening clinical trajectory and renal function, she underwent percutaneous kidney biopsy. Histopathological analysis demonstrated pyelonephritis with focal micro-abscesses alongside a diffuse histiocytic infiltrate. On light microscopy, only a single ischemic glomerulus was observed, and few tubules were recognizable. Arteries were not identified. Diffusely positive cortical immunohistochemical staining for CD163 confirmed the presence of macrophage/histiocytes, and von Kossa stain was positive in small round formations within the histiocytic infiltrate (Michaelis-Gutman bodies), consistent with a diagnosis of renal malakoplakia (Fig. 2).
Fig. 2
Von Kossa stain of kidney biopsy. Brown cytoplasmic inclusions (arrowhead) within histiocytes (arrow) represent Michaelis-Gutmann bodies, characteristic of malakoplakia
Based on prior case reports describing successful treatment of malakoplakia, the infectious disease team recommended changing antibiotics to agents with high intracellular penetration. As the E. coli was resistant to fluoroquinolones, trimethoprim, and tetracycline, the patient was started on tigecycline and aztreonam; two weeks later this was changed to minocycline monotherapy. To improve lysosomal function and phagocytosis she was started on ascorbic acid 500 mg daily and bethanechol 10 mg three times daily [6]. Given hepatomegaly, the patient underwent a liver biopsy demonstrating steatohepatitis with moderate macro-vesicular steatosis and abundant Mallory Denk bodies but no evidence of hepatic malakoplakia.
With treatment the patient’s hemodynamics and kidney function improved. Dialysis was discontinued 31 days after initial presentation. Despite overall clinical improvement, leukocytosis and fevers persisted. Repeat imaging demonstrated enlarging left renal abscesses. A renal mercaptuacetyltriglycine scan on day 45 revealed right and left split kidney function of 75% and 25%, respectively. Given reduced left-sided kidney function with ongoing evidence of infection, a radical left nephrectomy was performed on day 82 (Fig. 3). The patient’s leukocytosis resolved, and she was discharged from the hospital 89 days after initial presentation. Three months after discharge her serum creatinine was 1.2 (eGFR 61 ml/min/1.73m2). She completed a 12 month course of oral minocycline, ascorbic acid and bethanechol after repeat MRI demonstrated stable appearance of the right kidney (Fig. 4).
Fig. 3
Gross pathology of left kidney and surrounding perinephric soft tissue (overall 13.1 × 10.1 × 8.9 cm), comprised of kidney (8.6 × 6.4 × 8.5 cm) and ureter (not pictured, 5.1 cm in length x 0.4 cm in diameter). The specimen was notable for the extent of inflammation and scarring, as well as tan-yellow nodules with purulent exudate characteristic of malakoplakia
Fig. 4
MRI abdomen with and without intravenous contrast performed after 1 year of antibiotic therapy. Imaging is notable for absent left kidney and improvement in right kidney morphology
留言 (0)