
記住我

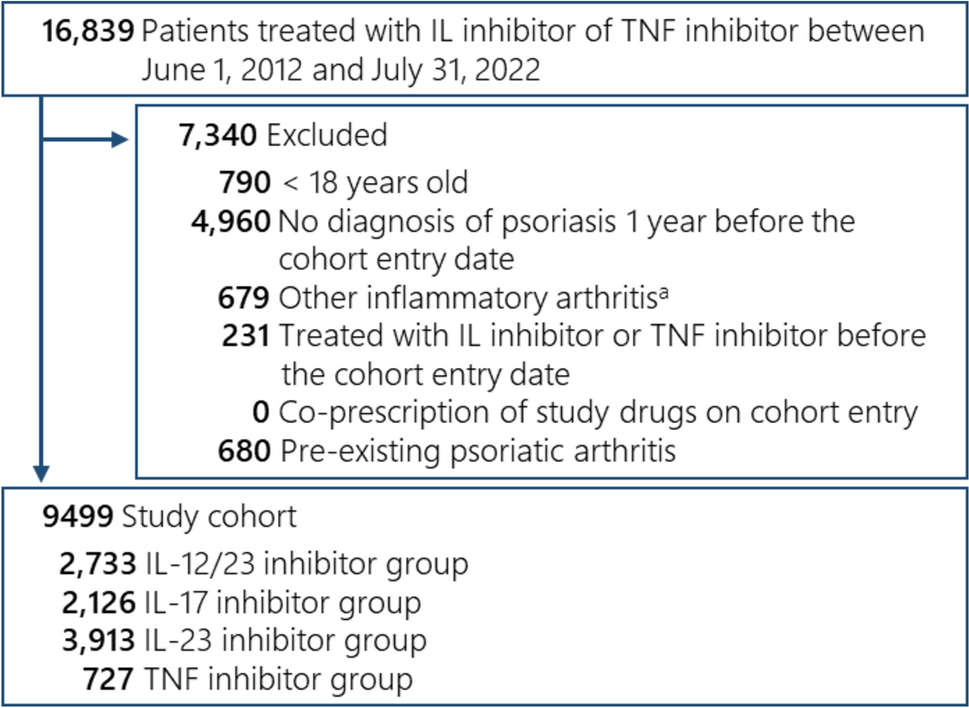



The search of the five databases resulted in identification of 11,541 studies, of which 1867 were duplicates. This resulted in 9674 studies remaining. A further 9399 studies were removed based on the author’s judgement of relevance of the title and abstract, and with 31 of the 275 remaining studies not available for retrieval, 244 articles were retrieved for full review. During the full review, 150 studies were excluded for the following reasons: (a) duplicates: 2 studies, (b) wrong study outcomes: 15 studies, (c) wrong study design: 95 studies, (d) non-primary research: 17 studies, (e) insufficient detail: 3 studies, (f) not available in English: 1 study, (g) outdated study: 17 studies (publication prior to 2016). This resulted in 94 studies being included in the final review. A PRISMA flowchart [22] is displayed in Fig. 1 outlining the inclusion and exclusion process for studies reviewed as part of this systematic review.
Fig. 1
Flow diagram of the study selection process
3.2 Characteristics of Included StudiesThe characteristics of the 94 studies included in this systematic review are displayed in Supplementary Table 1 (see ESM). The included studies ranged in year of publication from 2017 to June 2023. There were 12 studies included from 2017 to 2018, while there were 58 studies included from 2019 to 2021. Of the 94 studies included, 59 were cross-sectional studies, 20 were qualitative research studies, 12 were cohort studies, and three were economic evaluations. There was an even split of six retrospective studies and six prospective studies within this category, with seven of these studies involving patients, two considering the actions or decisions of health professionals, while three examined decisions or actions by decision makers or others (payers, insurance providers) (Supplementary Table 1). These were either mixed methods or quantitative studies, with each of them looking at either experts, decision makers, or patient characteristics (Supplementary Table 1, see ESM).
Of the 59 cross-sectional studies, 55 used surveys as their primary research instrument, while three of these studies employed interviews, and two used statistical analysis of data. Of the 20 qualitative research studies, 16 of these studies using interviews as their primary study instrument. The remaining four used focus groups. Of the 12 cohort studies, six were prospective in nature, while the other six were retrospective. The economic evaluations were each designed to measure specific economic outcomes focused on biosimilar uptake and/or generated savings.
Of the 94 studies included, 42 were published in Europe, with 32 in North America, ten in Asia, four in Australia/New Zealand, and two for each of South America, Africa, and the Middle East. The country delivering the most publications was the United States of America (USA), with 31 of the included studies. The second largest contributor of studies was Belgium with ten (see Supplementary Table 2 in the ESM).
Within the systematic review, as detailed in Supplementary Table 1, 13 of the included studies were qualitative research, with 11 of these studies using interviews as their primary study instrument. The remaining two used focus groups. Most of the qualitative research involved multiple stakeholders (patients, health professionals, carers, experts, decision makers, or others), with seven of these studies involving experts or decision makers, while eight involved health professionals, six involved patients, two involved others (payers etc), and one involved carers.
3.3 Quality AppraisalApplying the JBI framework, 89 of the 94 studies were rated as high according to the accepted scoring criteria. All 59 cross-sectional studies were rated as high with a scoring range of 6/8 to 8/8, while 18 of 19 qualitative research studies were rated as high, with one study rating as medium. The scoring range for qualitative research studies was 5/10 to 10/10, while nine of the 12 cohort studies rated as high, with the remaining three rating as medium. The scoring range for cohort studies was 5/11 to 11/11. All three of the included economic evaluations rated as high, with a scoring range of 8/11 to 11/11.
Most studies set out clear criteria for inclusion and exposure was measured in a valid way. However, where confounding factors were identified, there were often poor, or no strategies stated to deal with these (57 of 60 cross-sectional studies). Additionally, four of the 12 cohort studies did not clearly identify strategies for dealing with confounding factors (Supplementary Table 1, see ESM).
Notably, 13 of the 19 qualitative research studies did not clearly identify the researcher culturally or theoretically within the context of the research. Additionally, two of the three economic evaluations included did not adjust costs and outcomes for differential timing (Supplementary Table 1, see ESM).
3.4 Summary of FindingsThe findings of the 94 studies included in this systematic review are included in Supplementary Table 1 (see ESM). This table includes details of the seven aspects considered in this review, including (1) year of publication, (2) country of publication, (3) approach (qualitative, quantitative, mixed methods), (4) primary study instrument, (5) target population, (6) type of study, and (7) raw quality assessment score.
3.4.1 Target Populations of Included StudiesThis systematic review found that most (46) studies (48.9%) included were focused on HCP-centric barriers or enablers, with systemic and patient-centric barriers and enablers holding a relatively equal share of the remainder at 28 studies (29.7%) and 33 studies (35.1%), respectively (Supplementary Table 1, see ESM). Within this systematic review, 51 of the studies included HCPs as targets of their studies, and the second most frequent study population being patients at 35 studies including patient populations (Supplementary Table 1, see ESM).
Of the 51 studies specifically examining HCP populations, 38 were cross-sectional studies and 11 were qualitative research. Of the 51 studies that examined HCPs as a target population, the literature points to specialist clinicians being the primary focus of research on enablers and barriers affecting biosimilars on health professionals, with 47 of these 51 studies focused on specialists, while 13 studies included pharmacists, and six included nurses (Supplementary Table 1, see ESM).
As outlined in Supplementary Table 1, the second most frequently studied population was patients and/or their carers, with 35 of the 94 studies including patients and/or carers within their study populations. The primary instruments applied to studying these patient or carer populations were surveys, with 17 of the 35 studies utilising surveys and another 12 studies applying interviews (Supplementary Table 1, see ESM). The primary aims of studies of patients were to examine their perceptions/attitudes and/or knowledge and/or understanding of biosimilar medicines, with 13 of the included studies examining these areas, and another ten studies examining patient perspectives about non-medical or mandated switches to biosimilar medications (see ESM [18]).
Importantly, the least frequently examined general population was decision makers, with 15 of the studies including decision makers within their target populations (Supplementary Table 1, see ESM). Decision makers can be broadly classified in this context as administrators and officials within healthcare institutions, government officials, or policy makers. The most applied instrument studying decision makers was interviews, with eight of the 15 studies utilising this method. Other instruments included surveys, cohort studies, literature reviews, cross-sectional studies, and economic analyses. Generally, the focus of these studies was to understand what has transpired to affect biosimilar uptake, and to understand what may be limiting, or what may drive increased uptake of biosimilars.
3.4.2 Barrier and Enabler Classification FrameworkIn reviewing the literature, three categories of barriers and enablers have emerged: barriers or enablers of patient acceptance or uptake, barriers or enablers of HCP acceptance and usage, and systemic enablers or barriers, including pricing, education, regulation, quotas, amongst others [12]. This categorisation of enablers and barriers assists in simplifying the view of the effect on uptake of biosimilars. Importantly, in orienting us to these classifications, systemic barriers and enablers can be viewed as foundational to both HCP and patient barriers and enablers. We will further explore the relationships between these classifications later in this review. Both enablers and barriers will be examined in detail, considering the most significant factors affecting uptake of biosimilar medications in each of the patient, HCP, and systemic categories. This examination will start with a consideration of enablers.
Table 2 provides a visual representation of the barrier and enabler classifications, with the vertical columns displaying the three classifications (systemic, HCP, and patient) and each of barriers and enablers. The horizontal rows represent the specific barriers or enablers detailed or discussed in the included articles and the frequency of occurrence (number of articles). Table 3 provides a visual representation of the roles played by the actors (HCPs, patients, systemic actors) through the lens of ANT, specifically mediators, with broad, narrow, or mixed degree of agency.
Table 2 Frequency of occurrence of roles played by actors (enablers or barriers to uptake of biosimilar medicines) within the included studiesTable 3 Roles of actors (mediators) within studies (broad, narrow, or mixed degree of agency)3.4.3 Enablers Facilitating Uptake of Biosimilar MedicinesWithin this review, 29 of the 94 articles addressed or included systemic enablers. Of these 29 articles addressing systemic enablers, the most frequently cited type of enabler was policies and guidelines (25 articles). Further to this, policies and guidelines are the most cited group of enablers. However, as indicated earlier in this review, only 15 of the articles focused specifically on decision makers as a target population, instead looking at these systemic enablers through the lens of either the health care provider and/or the patient. In reviewing specific types of policies addressed, eight of the studies specifically considered mandatory or non-medical switching, while six of the studies considered incentives or gainshare arrangements (Table 2).
Financial capacity and cost savings were the other significant enablers in both the systemic and HCP categories, but interestingly, not the patient category. Financial capacity and cost savings were considered as systemic enablers in 14 studies, and HCP enablers in 12 studies (Table 2). Moorkens et al. [23] indicated that qualitative results of their study demonstrate that the price difference between biosimilar and originator products is an important factor in making it worthwhile to switch the patient. Further to this, Moorkens et al. [24] indicated in their 2019 study that relative difference in discounted price between the biosimilar and the originator product is a key driver of biosimilar medicines. The savings generated by utilising the lower cost biosimilar can be distributed through gain share agreements with key stakeholders.
In the patient category, the most frequently discussed enabler is utilisation of a medical interview, or positive framing of the switch to or start of a biosimilar medication, mentioned or discussed in six of the 24 studies involving patient populations (Table 2). Pouillon et al. [25] stated that the patient–health care provider relationship is a key driver of acceptance of biosimilars and limits risk of negative bias, going on to say that education about biosimilars should be tailored to the individual patient, taking into account nocebo effect risk profile. Further to this effect, Gasteiger et al. [26] indicated that positive framing by a clinician increased willingness to switch from 46 to 67%, while positive framing also increased perception of effectiveness of the biosimilar.
It has been observed through review of the literature that there are strong linkages or dependencies between the enablers. For instance, while a substitution policy may drive uptake of biosimilars, patient outcomes are somewhat dependent on patient–health care provider relationships [27]. Importantly, the confidence of the clinician or pharmacist in sharing information with the patient is dependent on their education and confidence in the efficacy and safety of the biosimilar medicines [28].
3.4.4 Barriers Inhibiting Uptake of Biosimilar MedicinesThe perceived efficacy of biosimilar medicines is the most frequently discussed barrier to biosimilar acceptance by both HCPs and patients in the literature, with 22 articles discussing concerns about safety, efficacy, or limited knowledge of biosimilars by HCPs, and ten articles discussing efficacy or safety concerns by patients (Table 2). Edgar et al. [29] indicated in a 2021 study that one of the three hurdles to biosimilar adoption was the lack of confidence in biosimilar interchangeability and a need for education about biosimilars. From the patient perspective, a study by Teeple et al. [30] found that 85% of patients were concerned that biosimilars would not treat their disease as well.
Interestingly, a clear distinction has been observed in the literature between starting new patients on biosimilars and switching currently treated patients to a biosimilar. To highlight this, four articles indicated a higher comfort level in clinicians starting treatment-naïve patients on biosimilars, relative to switching. In a 2022 study, Demirkan et al. [31] found that nearly half (45%) of the paediatric rheumatologists surveyed preferred to prescribe biosimilars in the treatment of biologic-naïve cases.
In examining the systemic barriers to biosimilar use or acceptance, the most frequently discussed issue was lack of effective policies or guidelines (11 studies), followed by lack of financial or cost-saving incentives (six studies) (Table 2). Druedahl et al. [32], in a 2022 study of expert views, found that almost all participants saw no need for additional scientific data to support substitution, and urged greater policy debate on biosimilar substitution, urging European and UK policy makers and regulators to clarify their visions for biosimilar substitution. To expand on this, there is a distinction in the literature between demand- and supply-side policies. A study by Kim et al. [33] found that demand-side policies used in the UK and France have been more effective than the supply-side price linking policy used alongside few demand-side policies, where the volume of the originator brand of infliximab actually increased. A study by Barcina Lacosta et al. [34] lists the existence of policy frameworks that do not necessarily support the initiation of switching protocols as one of four key barriers to biosimilar uptake.
Several studies included in this review also mentioned the issue of the originator being advantaged through rebates or arrangements with insurance providers, limiting the use of biosimilars (Table 2). For instance, Herndon et al. [35] found, in a 2021 study, that rebate increases of reference biologics were rated as the highest (85%) barrier to health system adoption of biosimilars. While there are several types of barriers to the use of biosimilars, the literature has clearly identified that the most significant barriers are HCP and patient concerns about safety and efficacy, and their lack of general knowledge about biosimilars. From a systemic perspective, the most significant barriers are the lack of effective policies and guidelines, such that there are concerns about whether the promised cost savings of biosimilars can be achieved (Table 2).
3.4.5 Classification of Network Actors Within the Included StudiesNotably, only four of the studies (seven total scenarios) positioned the HCP as exclusively a mediator with a narrow degree of agency, or effectively a limited-decision maker within the network, while in all others the HCP functioned as a mediator with broad degree of agency (Table 3).
Interestingly, in each of these studies, the positioning of the HCP as a mediator with narrow degree of agency was the result of an insurance payer or institutional decision requiring patients to use biosimilar medications, effectively displacing the decision-making role from the clinician or pharmacist assemblage with the patient and shifting the balance of agency across the spectrum to the policy actor. An example of this was in Sullivan et al. [36], where patients were required to switch to biosimilar medications but were reluctant to accept biosimilar medications, highlighting the importance of patient and physician communication.
In contrast to the positioning of the HCP as a mediator with broad degree of agency, the patient or carer actor is most often positioned as a mediator with limited degree of agency in their assemblages with such actors as HCPs, insurance payers, and the medicines themselves within their network(s). In 13 of the included studies (22 total scenarios), the patient was positioned as an actor with narrow degree of agency, whereas the patient is positioned exclusively as a mediator with broad degree of agency in only eight of the studies (15 total scenarios) (Table 3).
留言 (0)