
記住我






Different studies have shown that the most common etiologic factor of OAF is complicated maxillary posterior tooth extraction, particularly extraction of the upper 1st molar, the upper 2nd molar, and finally the upper premolars [1, 2]. This might be due to the proximity of the maxillary roots to the thin MS floor in some cases. OAF was observed after extraction of the maxillary first molar in five patients, after extraction of the upper second molar in three patients, and after extraction of the wisdom molar in only one patient. The age range reported in this study was 31 to 44 years. Similarly, research conducted by Rasoul Gheisari et al. [29] has shown that OAF commonly occurs between the third and fourth decades of life and rarely occurs in children and adolescents. It has been suggested that the loss of teeth as individuals age could increase the possibility of OAF occurrence.
In this study, all patients suffered from unilateral odontogenic maxillary sinusitis related to the OAF. It was reported that 77.78% of patients suffered from headache and 55.56% of them had unilateral nasal obstruction. This finding agrees with a study by Georg Watzak et al. [3]. who reported unilateral maxillary sinusitis on the 4th day after sinus exposure in 60% of patients [3]. Considering the undesirable consequences of MS infection due to further penetration of bacteria and fungi into the sinus, closure of the OAF is a significant issue. A study performed by Soukaina Essaket et al. [30]. concluded that complete elimination of the fistulous tract, any pathology in MS, deteriorated polypoid mucosa, and any foreign body is mandatory for long term successful closure of the OAF and for decreasing the risk of failure [30].
Individuals who suffer from chronic sinus disease and who do not respond to conservative medical treatment need to undergo surgery, which includes the Caldwell-Luc procedure or the EMMA technique to manage sinusitis and provide adequate sinus drainage. EMMA enables the MS ostium to remain patent while meticulously preserving the mucosa, restoring normal function, and achieving efficient mucociliary clearance [7]. Recently, a one-stage approach was described to eliminate the infection completely, restore the physiological drainage of the sinus, and prevent the recurrence of maxillary sinusitis in patients who had OAF complicated by chronic sinus disease. In this study, all patients underwent a one-stage EMMA technique combined with the application of PRF membranes and were covered by an acrylic splint for more protection and prevention of contamination. With this technique, complete closure of the OAF with preservation of the vestibular sulcus depth, and successful sinus drainage were achieved in all patients without any complications. Additionally, widening of the natural MS ostium, and great resolution of sinusitis symptoms were observed with minimal postoperative pain, and edema that was verified through the results of clinical examinations and CT scans. A study performed by K. Joe Jacob et al. [6] revealed that EMMA was superior to Caldwell-Luc’s technique in regard to intraoperative and postoperative parameters such as patient comfort, pain, edema, epistaxis, bleeding, and hospital stay days for the treatment of chronic maxillary sinusitis [5, 6]. Usually, an antrostomy at the inferior meatus is created with the Caldwell-Luc procedure. A study performed by Yu Chen Huang et al. [31] and Mohamed S. Elmaradny et al. [32] suggested avoiding unphysiological inferior meatus antrostomy in diseased MS patients [31, 32].
Regarding the closure of the OAF, there are various techniques that can be used, but the choice between them is controversial. A study performed by Puria Parvini et al. [11] reported that using soft tissue flaps as buccal advancement flaps has several drawbacks, such as postoperative pain, reduction of the buccal sulcus, and edema due to mucoperiosteal flap reflection. In this study, PRF membranes and acrylic splint were used in all patients to minimize surgical trauma, and overcome complications such as flap necrosis, and the impossibility of repeating the surgical technique in case of clinical failure. Additionally, this technique preserves the height of the vestibular sulcus, which is a main concern in the planning of removable prosthodontic treatment. This finding is in accordance with that of G. Dell’Aversana et al. [12] who reported that the use of a PRF membrane alone provides excellent outcomes in the closure of oroantral communication with a low risk of complications, and promotes the development of mineralized tissue due to its osteoconductive properties [12, 33].
PRF has been used in various medical applications due to its simple preparation, as it does not require an anticoagulant [22]. It creates a dense three-dimensional fibrinous architecture matrix that can be sutured to the tissue [12]. A study by Ankit Sharma et al. [16] showed that PRF could stimulate osteogenesis and proliferation of osteoblasts, gingival fibroblasts, and periodontal ligament cells. These cell types are beneficial for bone formation and soft tissue regeneration [16, 18]. Similarly, a study by Zhanqi Wang et al. [34] showed that PRF promotes the continuous release of growth factors such as platelet- derived growth factor (PDGF), fibroblast growth factor, transforming growth factor β (TGF β-1), and vascular endothelial growth factor (VEGF), for up to 14 days. These factors promote angiogenesis and stimulate the healing process. Additionally, PRF increases vascularization, suppresses inflammation, and minimizes local pain [35, 36].
The outcomes of this study validate that the pain level was minimal, as 77.78% of the patients had no pain and 22.22% had mild discomfort on the 7th day postoperative. This finding agrees with the findings of Ahmed W [13]. and G. Dell’Aversana et al. [12] who reported that pain reduction may be due to the use of less invasive techniques and the anti-inflammatory activity of the PRF components. Additionally, research performed by Jonathan Meza et al. [37] on the effect of PRF in oral surgery has shown that PRF can minimize pain levels, and consequently decrease the need for analgesics [34, 37].
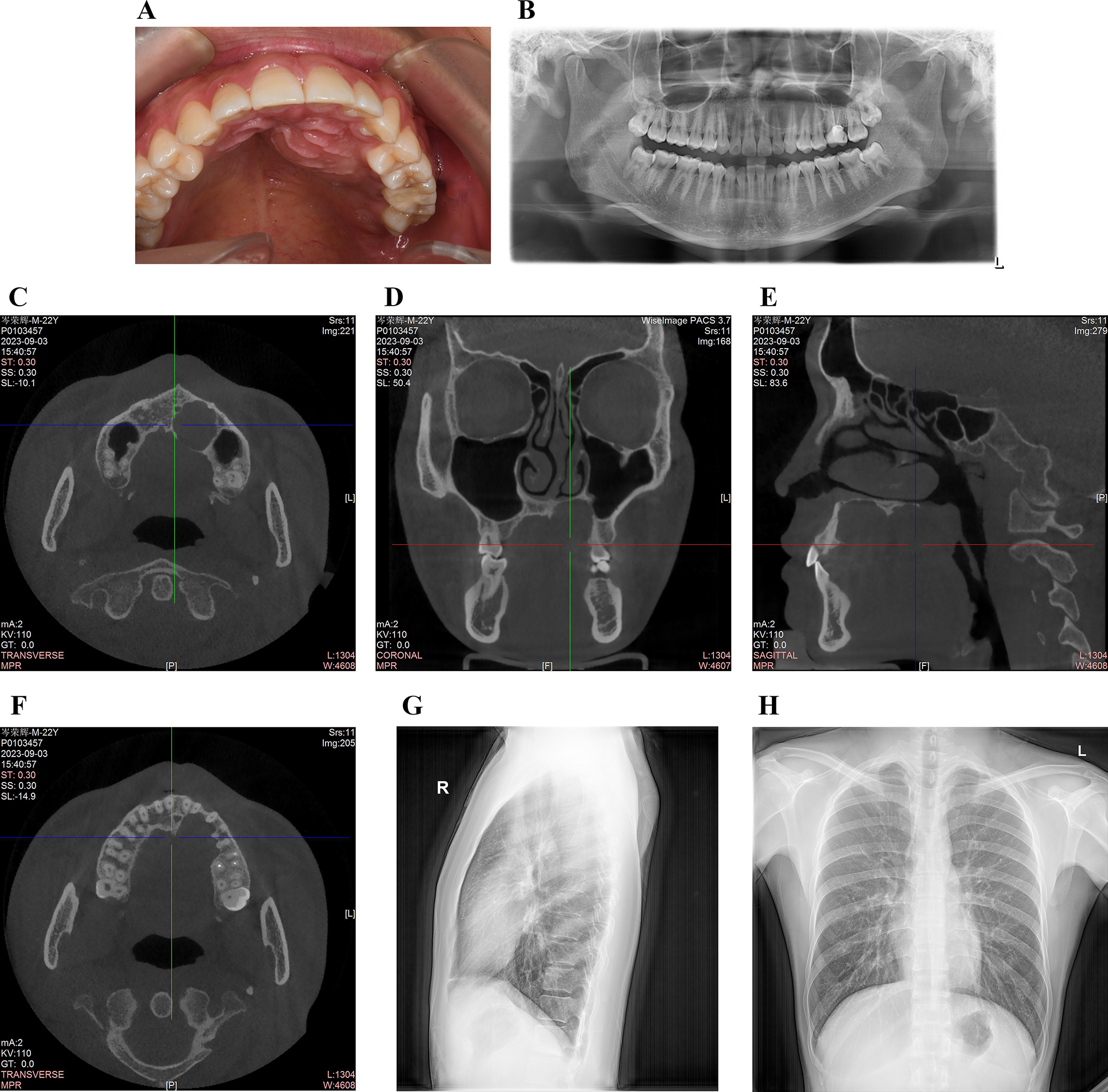
Radiographic follow-up was performed after 24 weeks postoperatively via CT scans. CT is considered the gold standard imaging technique and a reliable method for diagnosing MS pathology. It provides appropriate MS imaging due to its excellent resolution, accuracy, and ability to distinguish between soft tissue and bone [38]. A significant decrease in the size of the bone defect was found on postoperative CT compared with preoperative CT. Additionally, opacification in the ipsilateral MS cavity was observed on preoperative CT, but it disappeared completely in all patients on postoperative CT after EMMA which revealed a clear sinus with adequate drainage. (Table 6; Fig. 6) The limitation of this study is the small sample size, therefore more research is required to validate the findings. Within the limitations of this study, we achieved successful closure of the OAF, MS drainage, as all the excessive secretions were eliminated completely, and improvement in the quality of life of the patients when the EMMA technique combined with the application of PRF membranes were used.
Fig. 6
(A) Preoperative CT scan (coronal plane) showing an OAF, and discontinuity in the MS floor associated with complete opacification of the left MS. (B) Postoperative CT after 24 weeks revealed complete disappearance of the opacification at the left MS, and the fistula was obliterated
留言 (0)