
記住我



Orthopedic infection has been recognized as one of the major public health problems globally, which are usually complex and difficult to treat (Long et al., 2020; Premkumar et al., 2021; Metsemakers et al., 2023). It has a wide clinical spectrum, among which five types of bone and joint infection were usually categorized (Colston and Atkins, 2018; Kavanagh et al., 2018; Higgins et al., 2022), including septic arthritis, prosthetic joint infections, osteomyelitis, spinal infections, and diabetic foot osteomyelitis. Additionally, with the increased burden of traumatic injury (Chen et al., 2017), orthopedic infection associated with injury has drawn more and more attention, particularly fracture related infection (FRI) (Metsemakers et al., 2018; He et al., 2023).
Accurate diagnosis of orthopedic infection is critical for proper and timely patient managements, including antimicrobial treatment and surgery. The diagnostic schemes developed for orthopedic infection have been focused on both microbial etiology and host inflammatory response (Higgins et al., 2022). Culture followed by biochemical assays has been widely used as the gold standard. In combination with matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF), identification of the cultured organisms has been greatly accelerated. MALDI-TOF alone was also utilized directly on clinical specimens independent of culture, particularly for the identification of microorganisms that are not culturable, however, the performance was found lower than that with culture enrichment in some cases (Kuo et al., 2020). With the rapid development of the molecular tools, polymerase chain reaction (PCR) based detection methods have been widely used, including conventional targeted PCR, broad range PCR followed by sequencing, and real time PCR or quantitative PCR (qPCR). These molecular methods have significantly shortened the turn-around-time and eliminated the false negative results by culture due to prior antibiotic treatment (Morgenstern et al., 2018).
Host responses are often assessed through detecting the biomarkers in serum or synovial fluid, histology, or radiology (Higgins et al., 2022). The inflammatory biomarkers, such as erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), can be readily included in the laboratory tests, but caution may have to be taken when interpreting the results due to the lack of specificity for infection. Histological analysis can provide confirmation for the inflammation, but can’t be utilized as a stand-alone method to rule out infection because of its low sensitivity. More advanced imaging examination such as ultrasound, radiology, computed tomography (CT) or magnetic resonance imaging (MRI) can facilitate the diagnosis, but such technologies are not always available (Jiang et al., 2015; Wang et al., 2017).
We have previously developed and validated a wide range of qPCR assays for molecular diagnostics of infectious diseases (Liu et al., 2014, 2016a, 2016b; Moore et al., 2019). Quantitative analysis approach facilitated the understanding of the etiology and epidemiology of these diseases (Liu et al., 2016c). The current study aimed to detect multiple bacterial pathogens by quantitative PCR (qPCR) directly on clinical samples of hospitalized orthopedic patients with or without suspected infection, so as to identify the main causative pathogens for such diseases and evaluate the clinical characteristics and risk factors of orthopedic infection.
2 Materials and methods2.1 ParticipantsInpatients with complete records of demographic, clinical and laboratory information, and with at least one specimen collected were enrolled in the Department of Orthopedics, Qingdao Huangdao Traditional Chinese Medicine Hospital from January 2021 to July 2023, excluding patients with bone tuberculosis and diabetic foot. Their infection statuses were evaluated by the clinicians upon admission, which was used to divide the participants into two groups, one with clinically identified infection manifestation and the other with no sign of infection. A patient was categorized into Group A (suspected infection) with any one or more of the 9 scenarios below (Table 1).
a. Open injury with severely contaminated wound;
b. Hospital admission was more than 24 hours after the onset of open injury;
c. Skin redness, swelling, high skin temperature, pain with dermal ulcer, fistula, sinus track, or purulent exudate;
d. Joint redness, swelling, and burning pain accompanied by elevated body temperature or increased white blood cells count (WBC), neutrophils, CRP, ESR, or other inflammatory biomarkers;
e. Abnormal joint puncture fluid or purulent joint fluid;
f. Joint or limb abscess with visible pus;
g. Post orthopedic surgery, the incision was red, swollen, burning, painful, and ruptured with non-bloody exudate;
h. Blood culture was recommended when the body temperature continued to rise with no other infection and hematogenous dissemination was considered.
i. Clinical samples were collected during the operation of confirmed infection cases.
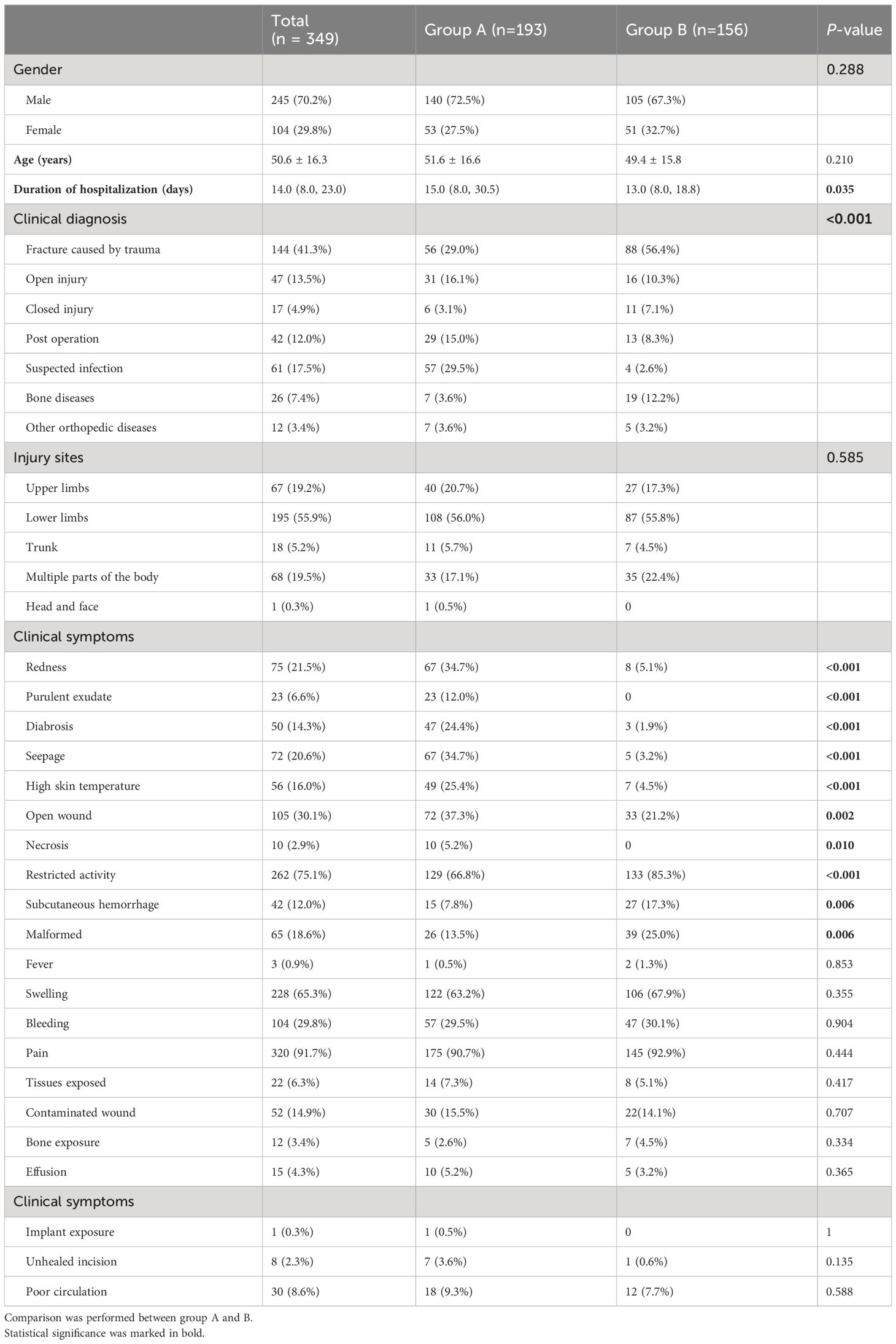
Table 1 Demographic characteristics and clinical diagnosis of patients enrolled in the current study.
The patients with the following scenarios were categorized into Group B.
a. Sampling the open wound after debridement to rule out infection;
b. Routine culture when pulling out drainage tube post orthopedic surgery;
c. Routine culture of bloody exudate post orthopedic surgery;
d. Bacterial culture was performed on turbid joint puncture fluid to rule out infection;
e. Samples of joint or limb hematoma (no obvious pus) to rule out infection.
2.2 Specimen collectionTwo swab samples (dry or in transport medium) or exudate samples were simultaneously collected from all the patients upon enrollment following the standard hygiene procedure. One sample was subjected to bacterial culture immediately, and the other stored at −80°C until qPCR testing.
2.3 Bacterial cultureBacterial culture was performed with the swab samples collected in transport medium by plating blood agar or China blue agar plates (babio, Jixian, China), and incubation at 37°C for 24 hours. Single colonies were picked and tested with VITEK® 2 COMPACT automatic microbiology analyzer for bacterial identification (bioMérieux, Marcy L’Etoile, France).
2.4 Nucleic acid extractionSwab samples were resuspended in 200μl of PBS buffer (pH 7.2). Nucleic acid was extracted using manual bacterial genomic DNA extraction Kit (centrifugal column type, BioTeke, China) or automated IndiSpin® QIAcube® HT Pathogen Kit (Leipzig, Germany). Each sample was spiked with an external control, phocine herpesvirus (PhHV) to monitor the extraction and amplification efficiency. One extraction blank was included per batch of extraction to rule out laboratory contamination.
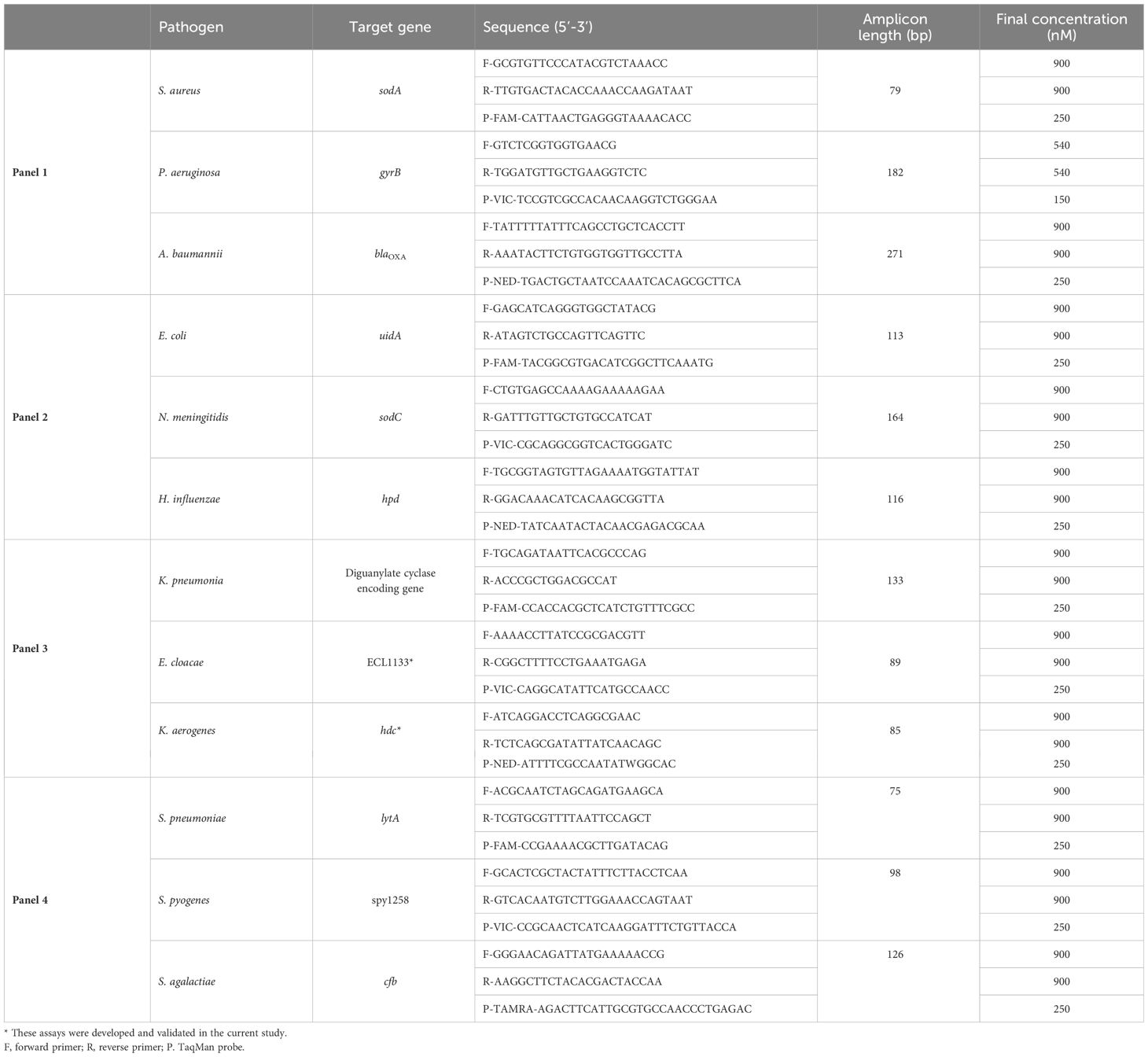
2.5 PCR testsReal-time PCR primers and probes were adapted from publications (Kodani et al., 2011; Diaz et al., 2013) or in house developed and validated, as listed in Table 2. Four 3-plex real-time PCR panels were formulated for the detection of 12 pathogens previously reported in orthopedic infection (Liebling et al., 1994; Wang et al., 2018; Xie et al., 2020; Bruun et al., 2021; Kawaguchi et al., 2022), including Staphylococcus aureus, Acinetobacter baumannii, Pseudomonas aeruginosa, Escherichia coli, Haemophilus influenzae, Neisseria meningitidis, Klebsiella pneumonia, Klebsiella aerogenes, Enterobacter cloacae, Streptococcus pneumoniae, Streptococcus pyogenes, and Streptococcus agalactiae. The panels were tested for linearity, lower limit of detection (LOD), repeatability, reproducibility, and analytical specificity as described in Supplementary Table S1. Each 10-μl multiplex PCR contained 5 μl of 2×AgPath-ID™ One-step reverse transcription PCR (RT-PCR) buffer (Life Technologies, USA), 0.4 μl of enzyme mix, primers and probes at the concentrations indicated in Table 2, and 2 μl of nucleic acid extract. Cycling conditions included 20 min of reverse transcription at 45°C, 10 min of initial denaturation at 95°C, and 45 cycles of 15 s at 95°C and 1 min at 60°C. One pooled positive control and a no template negative control were included in each run. qPCR panels were performed and analyzed with QuantStudio 7 Flex real-time PCR system with software v1.7 (Thermofisher, USA). Quantification cycle (Cq) 35 was used as the cutoff for positivity unless otherwise stated.
Table 2 Primer and probe sequences of multiplex qPCR.
2.6 Ethics statementThe study was reviewed and approved by the Ethics Committee of Qingdao University and Qingdao Huangdao Traditional Chinese Medicine Hospital. The patients provided written informed consent. All procedures were performed in accordance with the 1964 declaration of Helsinki and later amendments.
2.7 Statistical analysisThe measured data that conformed to a normal distribution were expressed in terms of the mean (X), and compared using a t-test. Measurements that fell within a skewed distribution were expressed as medians (interquartile range, IQR), and compared using a Mann-Whitney U test. A categorical variable was expressed in numbers or percentages, and proportions were compared using either Pearson’s chi-square or Fisher’s exact test. Receiver operating characteristic (ROC) analysis was used to evaluate the performance of qPCR against bacterial culture and determine the association of pathogen detection with infection status. Two-tailed P values were calculated, and values of < 0.05 were considered statistically significant. All analyses were performed using IBM SPSS Statistics version 26.
3 Results3.1 Clinical features of patients with suspected infectionA total of 349 inpatients were enrolled by Department of Orthopedics, and according to the clinical manifestations assessed by the clinicians upon admission, infection was clinically confirmed or suspected requiring laboratory diagnosis in 193 patients (group A) (Table 1). The rest 156 patients were classified into group B without any suspected infection, for which routine screening was performed to rule out infection. More male patients (245, 70.2%) were enrolled than females (104, 29.8%), with a male to female ratio of 2.64 in group A and 2.06 in group B (P = 0.288) (Table 1). The median age was 52 years in group A and 49 years in group B (P = 0.210). The length of hospital stay was statistically different, with a median of 15 (IQR 8.0, 30.5) days in group A and 13 (IQR 8.0, 18.8) in group B (P = 0.035). Fracture accounted for the most common diagnosis on admission (144, 41.3%), followed by suspected infection (61, 17.5%), open injury (47, 13.5%), post operation (42, 12.0%), bone diseases (26, 7.4%), closed injury (17, 4.9%), and other orthopedic diseases (12, 3.4%). Among the injured sites, the lower limbs were the most common, accounting for 55.9%. No difference in the injured sites was observed between the two groups. Table 1 showed the number of patients exhibited the clinical symptoms defining the two groups. The most common symptoms included open wound (37.3%), redness (34.7%), seepage (34.7%), high skin temperature (25.4%), diabrosis (24.4%), purulent exudate (12.0%) and necrosis (5.2%) in the infection group. Other symptoms had similar distribution in the two groups, such as fever, swelling, bleeding, pain, tissues exposed due to wound opening, etc. Majority of the patients in group B tended to have restricted activity (85.3% versus 66.8% in group A, P < 0.001). The laboratory tests (Supplementary Table S2) from a number of the patients showed elevated biomarkers for bacterial infections, such as white blood cell count (WBC, 18.4%), absolute neutrophil count (ANC, 25.4%), procalcitonin (PCT, 61.3%), ESR (68.0%), CRP (61.3%), and D-dimer (34.0%). There was no statistical difference between the two groups except high PCT in more patients of group B (P = 0.030).
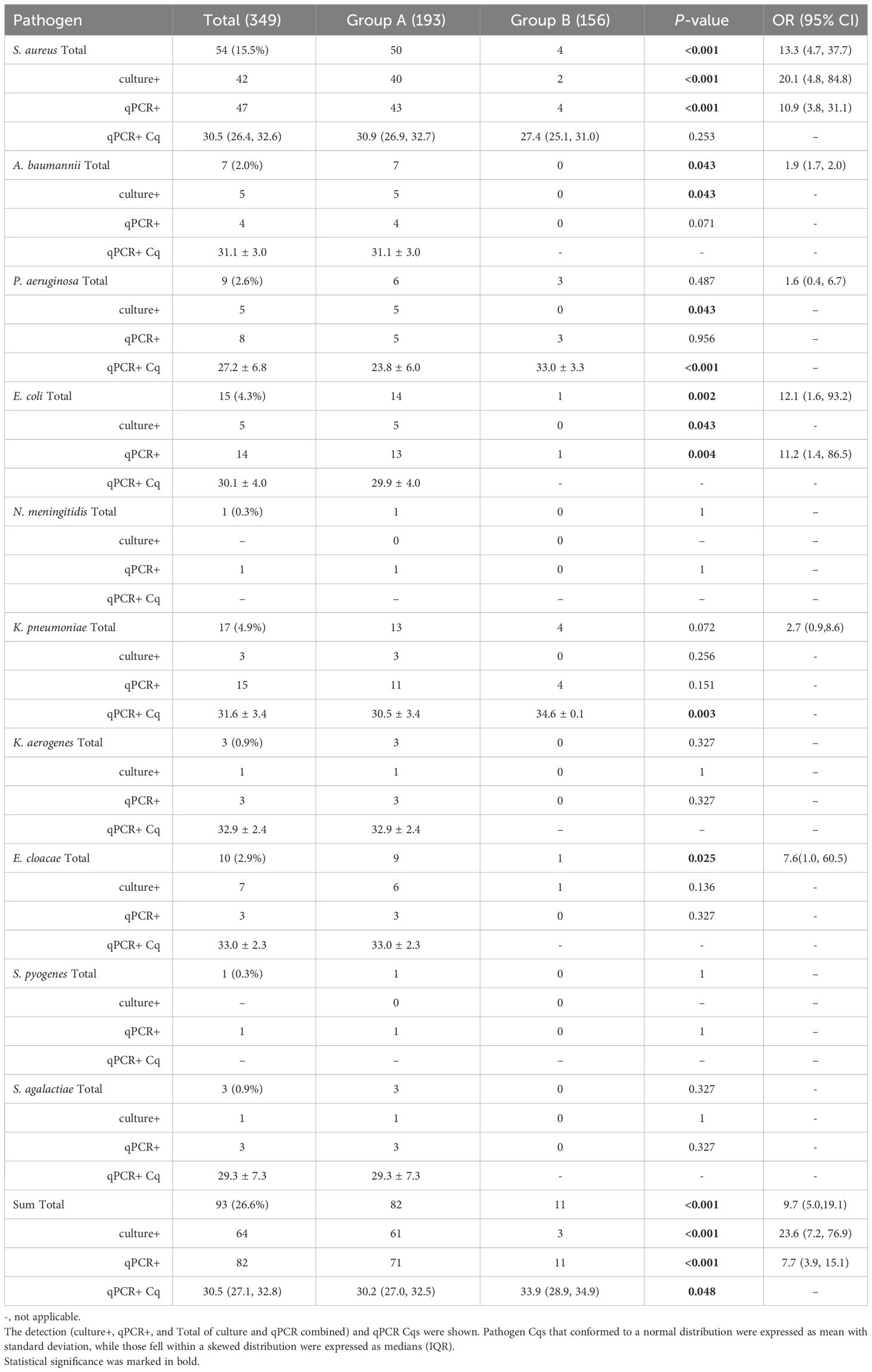
3.2 Pathogen detection by bacterial cultureAs shown in Table 3, 61 (31.6%) patients in group A were positive by culture for one of the 12 pathogens interrogated, with S. aureus predominantly detected at 20.7% (40/193), followed by E. coleacae complex (ECC) at 3.1% (6/193), and A. baumannii complex (ABC), E. coli, P. aeruginosa at 2.6% (5/193). Three (1.9%, P < 0.001) patients in group B were found positive, including 2 cases of S. aureus and one case of E. cloacae complex. Six of the ECC strains were identified as E. hormaechei, and one as E. roggenkampii through whole genome sequencing (data not shown). Similarly, three ABC strains were further identified as A. baumannii, two as A. pittii, and one as A. soli.
Table 3 Comparison of the bacterial pathogen detection between culture and qPCR in the two groups.
3.3 Pathogen detection by multiplex real time qPCR panelsMultiplex qPCR panels underwent standard optimization and validation (Supplementary Table S1). Depending on the target, the qPCR efficiency ranged from 80.1% to 100.0%. The LOD was 10–20 copies per qPCR reaction, which corresponded to an averaged Cq of 38.5. These assays demonstrated excellent repeatability and reproducibility, and an overall 97.1% analytical sensitivity and 100% analytical specificity on culture isolates.
With Cq cutoff of 38.5 determined at LOD, qPCR detected all culture positives except one case of S. aureus, P. aeruginosa, K. pneumoniae, and E. coli each. The E. cloacae assay, specifically targeting E. cloacae only, didn’t detect 7 non-E. colacae ECC culture positives. A. baumannii assay, specifically targeting A. baumannii only, detected two of ABC positive by culture, which were identified as A. baumannii, but not those identified as A. pittii and A. soli. These corresponded to an overall clinical sensitivity of 93.2% (55/59). However, qPCR yielded 132 excessive pathogen detections compared to culture. PCR followed by amplicon sequencing was then performed to confirm these results. Using the sequencing results as reference, ROC analysis showed that the results with Cq < 35 were reliably confirmed (data not shown). Cq cutoff of 35, which yielded a moderate consistency between qPCR and culture (Kappa = 0.712, P < 0.001), was used for further analysis. As shown in Table 3, 36.8% (71/193) of the patients in group A were tested positive for any of the 12 pathogens, with 15 (7.8%) for more than one pathogen. S. aureus was present in 40% of the mixed infections. Although there was no apparent infection, 11 (7.1%, P < 0.001) patients in group B were positive for S. aureus (4), P. aeruginosa (3), E. coli (1), and K. pneumoniae (4). The overall Cq values of group A (median 30.2, IQR (27.0, 32.5)) were significantly lower than those of group B (33.9, IQR (28.9, 34.9), P = 0.048), particularly for P. aeruginosa and K. pneumoniae. ROC analysis showed that Cq 28.7 and 34.4 served better separation of infection and non-infection groups for P. aeruginosa and K. pneumoniae, respectively. Consistent with the culture results, S. aureus was also the most prevalent pathogens by PCR (43, 22.3%). No positive was detected for H. influenzae and S. pneumoniae by either culture or qPCR. Combining the culture and PCR results, the detection of S. aureus, E. coli, E. cloacae, A. baumannii, K. pneumonia, and P. aeruginosa was significantly different between the two groups (Table 3).
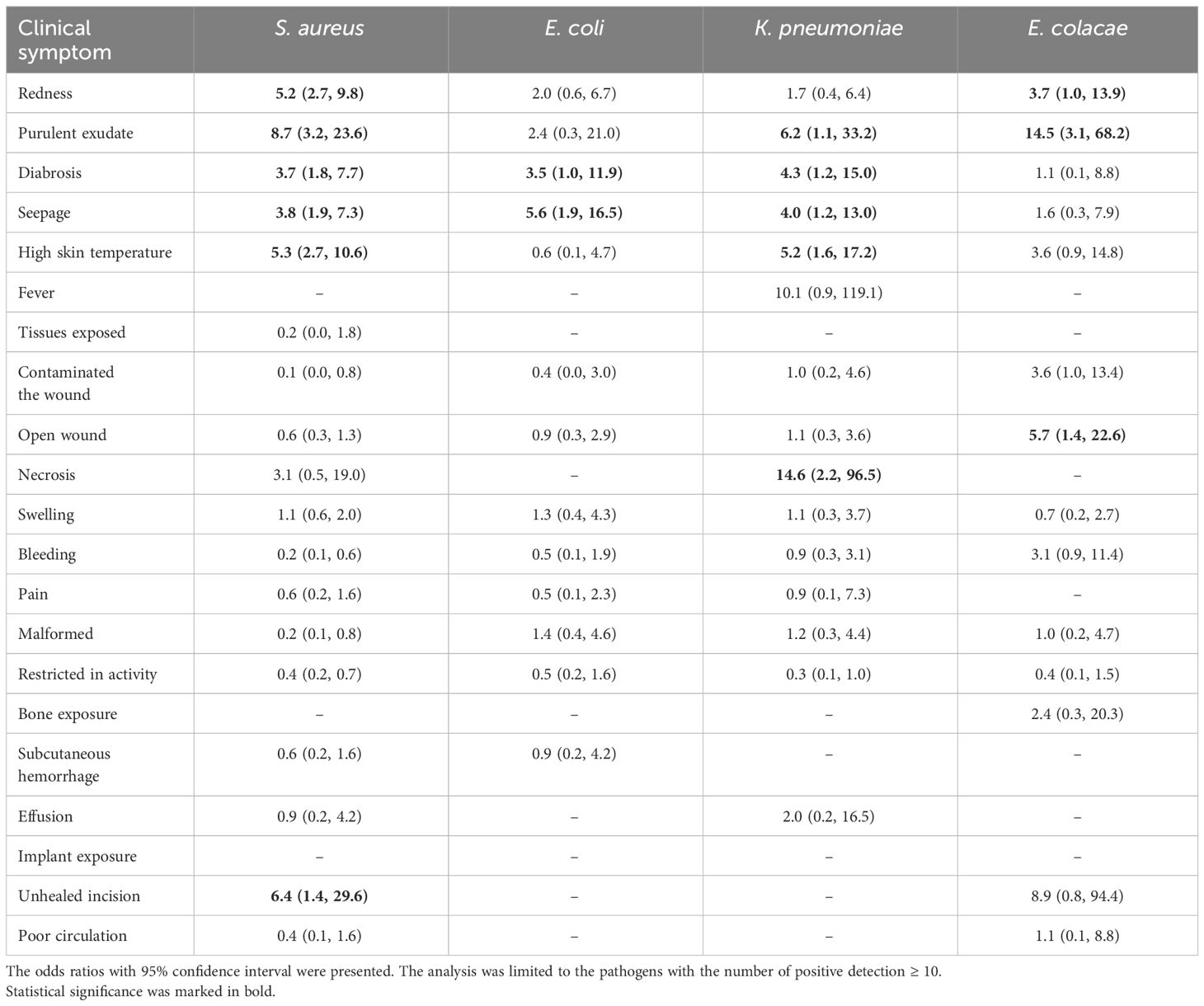
3.4 Clinical presentations related to bacterial pathogensComparing the clinical information of the patients with detection of any of the 12 pathogens by either culture or PCR (n = 81) with those without any of the pathogens detected (n = 95), statistically significant difference was observed in gender, clinical manifestations such as seepage and higher skin temperature, and surgery history (Supplementary Table S3). Bleeding, poor circulation, and tissues exposed seemed to be more common in the patients without any pathogen detected. Men are more susceptible to these causative agents, more than twice as likely to be infected as women (P = 0.027). Interestingly, sialic acid (SA) was significantly increased in the patients with pathogens identified (OR 2.4, P = 0.006), dominant by S. aureus (65%, 26/40; OR 3.1, P < 0.001). As the most prevalent pathogen (n = 54), S. aureus showed association with redness (odds ratio, OR 5.2, P < 0.001), purulent exudate (OR 8.7, P < 0.001), diabrosis (OR 3.7, P < 0.001), seepage (OR 3.8, P < 0.001), high skin temperature (OR 5.3, P < 0.001) and unhealed incision (OR 6.4, P = 0.027). E. coli (n = 15) likely caused diabrosis (OR 3.5, P = 0.034) and seepage (OR 5.6, P = 0.002). K. pneumoniae (n = 13) showed unique association with necrosis (OR 14.6, P = 0.022) while E. cloacae strongly associated with purulent exudate (OR 14.5, P = 0.005) (Table 4).
Table 4 The association of bacterial pathogens with clinical symptoms.
4 DiscussionIn this study, we enrolled 349 hospitalized patients from Orthopedics Department in a rural hospital with its patient population being mostly of relatively low socioeconomic status. Their initial clinical diagnosis upon admission were diverse, but with majority related to traumatic injury or operation (72.7%, 250/349). With further evaluation based on their clinical presentations, 55.3% (193/349) of these patients were diagnosed as suspected infection. Twelve bacterial pathogens were tested by both culture and qPCR on the wound samples, including commonly reported S. aureus, E. coli, K. pneumoniae, P. aeruginosa, A. baumannii, and E. cloacae, and less common bacteria such as H. influenzae, N. meningitidis, K. aerogenes, S. pneumoniae, S. pyogenes, and S. agalactiae. The two methods exhibited good correlation. With a conserved qPCR Cq cutoff at 35, where the positive results could be reproducibly confirmed with amplicon sequencing, pathogens were detected in 36.8% of patients with suspected infection. S. aureus accounted for 22.3% as the main cause, followed by other common pathogens, which was consistent with the findings on fracture associated infection in various regions in China (Wang et al., 2021a). Additionally, four of the less common pathogens, i.e. S. agalactiae, N. meningitidis, K. aerogenes, and S. pyogenes were detected. Further surveillance on these bacteria and beyond may be important to evaluate their clinical significance.
Worth clarifying is that the qPCR assay used for the detection of E. cloacae was species specific while bacterial culture identifies Enterobacter cloacae complex without further discrimination, which composes of E. cloacae, E. asburiae, E. kobei, E. hormaechei, E. roggenkampii, E. ludwigii, and E. bugandensis. Whole genome sequencing results showed that ECC isolates identified by culture in the current study were all non E. cloacae species, i.e. E. hormaechei and E. roggenkampii, indicating the needs of assays inclusive for ECC or specific for the major species with clinical relevance in the future surveillance. There may be a similar requirement for Acinetobacter baumannii complex, but likely to a less extent, as A. baumannii was found to be the predominant species.
While majority of the detection took place in group A, pathogens were identified, mostly by qPCR due to its high sensitivity, in 11 cases without apparent infection (group B). There was significant difference in pathogen quantities between group A and B. Furthermore, through ROC analysis, cutoffs of Cq 28.7 and Cq 34.4 perfectly separated the distribution of P. aeruginosa and K. pneumoniae in the two groups, respectively. This might indicate that pathogen quantity played an important role in infection severity and disease progression. The elucidation of the importance of such “subclinical infection” may require further investigation. Worth noting is that a big portion of samples (n = 132) yielded Cq values between 35 and 38.5 for at least one of the 12 pathogens. As the previous study ruled out the possibility of “false positive” resultant from dead bacteria in the infected wound (Kaplan et al., 2018), another possible source of such low level detections could be skin contamination during sample collection although standard hygiene procedure was applied. qPCR has the advantage of modulating the detection sensitivity and stringency for different purposes, most importantly clinical relevance, such as in childhood diarrhea and pneumonia (Liu et al., 2016c; Pneumonia Etiology Research for Child Health (PERCH) Study Group, 2019). Further longitudinal sampling combined with qPCR quantification might help resolve whether these results could reveal any meaningful implication on subclinical progression.
Gender was a risk factor for bacterial pathogens detection, with OR of 2.2 for male. Most patients with detected pathogens had a previous history of orthopedic surgery (OR 2.8, P = 0.038). Almost any of the bacteria that colonize at the anatomic sites can become an opportunistic pathogen causing infection (Garcia et al., 2019). The distribution of normal skin microbiota varies by individual. In general, surgical site infection (SSI) is greatly underreported, especially post discharge. For example, the rates of SSI in arthroplasties have been reported between 1% and 5%. However, post-discharge follow-up revealed an increase of 450% for SSI (Carneiro et al., 2014). In the current study, 11 of 13 cases with pathogen detected in the patients with no symptomatic infection (group B) were associated with surgery. This strongly suggested the necessity of pathogen screening post-surgery even without any apparent infection sign. Repeatedly, highly sensitive but modulable detection would be preferred.
The main clinical manifestations of patients in the pathogen positive group were exudation and high skin temperature while the top pathogens demonstrated distinct association with the clinical symptoms. The criteria used by the clinicians in the current study seemed to perform well to differentiate infection purely based on clinical manifestations, although they were admittedly subjective. In the patients with suspected infection, several biomarkers (Supplementary Table S2) that were previously reported to be relevant with orthopedic infection showed significant difference from those without apparent infection, such as increased absolute value of immature granulocytes (Wu et al., 2019), platelet count (Liu et al., 2022a), alanine aminotransferase (Talsnes et al., 2012; Huang et al., 2023), globulin (α1 and α2) (Ye et al., 2020), γ-glutamyl transpeptidase (Fisher et al., 2015), total cholesterol (Li et al., 2023), sialic acid (SA) (Cui et al., 2014), and decreased albumin (Fisher et al., 2015), Ratio of albumin to globulin (Wang et al., 2021b), prealbumin (Liu et al., 2022b), high-density lipoprotein cholesterol (Zhang et al., 2021). However, in the current study, none of the laboratory tests was found to be associated with infection, such as CRP, ESR, and PCT. The lack of specificity of these biomarkers has been recognized as the major obstacle for wide practical use. Interestingly, patients in the pathogen positive group had higher sialic acid (P < 0.05), and the OR value suggested that the risk of high sialic acid in patients infected with pathogens was 2.4 times higher than that in no pathogen detection group. Sialic acid has recently been found to play an important role in S. aureus airway infection by triggering virulence reprogramming (Ding et al., 2023). Whether these could be use as the guidance or biomarker for clinical diagnosis would require extensive verification.
The limitations of this study included, firstly, the study focused on hospitalized patients with orthopedic infections from a single center, which might introduce bias if the results were different from those of the outpatients and of other facilities. However, this study proved that clinical symptom based grouping criteria were mostly accurate for infection determination, and quantification brought more power to the analysis, although external validation of the quantitative findings is needed. Secondly, the sample size of this study was relatively small, particularly for the less common pathogens, which requires larger population for more comprehensive evaluation. Increased sample size from the continuation of such surveillance would also enable discrimination of etiology for orthopedic infection of specific mechanisms, such as fracture related infection, periprosthetic joint infection, osteomyelitis, etc. Meanwhile, continuous surveillance will allow us to track the temporal variation and evaluate the potential impact of SARS-CoV-2 pandemic during the research period of this study. Lastly, only twelve bacterial pathogens were analyzed in the current study, and about 30% of the samples from the patients with suspected infection were negative for all the pathogens even with Cq cutoff at 40.
Multiplex qPCR enabled faster, more sensitive and specific detection and quantification of the pathogens in orthopedic infection. Quantitative analysis improved the discrimination of symptomatic infection, potentially subclinical infection without any symptom, and no infection. This method could be utilized in combination with culture in such settings to guide antimicrobial therapy. It might be particularly useful for tracking the progression of infection during treatment. More extensive screening for various microorganisms, such as other bacteria, fungi, and viruses may be needed to comprehensively understand the etiology of orthopedic infection and their association with clinical features.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors upon request, without undue reservation.
Ethics statementThe studies involving humans were approved by Qingdao University, Qingdao Huangdao Traditional Chinese Medicine Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributionsYNW: Writing – review & editing, Writing – original draft, Validation, Methodology, Investigation, Formal analysis, Data curation. WX: Writing – review & editing, Resources, Methodology, Investigation. YW: Writing – review & editing, Project administration, Methodology, Investigation, Data curation. YC: Writing – review & editing, Resources, Methodology, Investigation. LY: Data curation, Writing – review & editing, Investigation. CL: Writing – review & editing, Investigation, Data curation. DZ: Writing – review & editing, Investigation, Data curation. XG: Resources, Writing – review & editing, Investigation. YDW: Writing – review & editing, Investigation, Data curation. SW: Writing – review & editing, Investigation. JLi: Writing – review & editing, Investigation, Funding acquisition. YL: Writing – review & editing, Methodology, Investigation. JH: Writing – review & editing, Resources, Methodology, Investigation. JLiu: Writing – review & editing, Writing – original draft, Supervision, Methodology, Funding acquisition, Conceptualization.
FundingThe author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was funded by Department of Science and Technology of Shandong Province, China (to JLiu).
AcknowledgmentsWe thank the staff of Qingdao Huangdao Traditional Chinese Medicine Hospital, China for their technical support to this project.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcimb.2024.1394352/full#supplementary-material
ReferencesBruun, T., Rath, E., Madsen, M. B., Oppegaard, O., Nekludov, M., Arnell, P., et al. (2021). Risk factors and predictors of mortality in streptococcal necrotizing soft-tissue infections: A multicenter prospective study. Clin. Infect. Dis. 72, 293–300. doi: 10.1093/cid/ciaa027
PubMed Abstract | CrossRef Full Text | Google Scholar
Carneiro, M., Krummenauer, E. C., Alves MaChado, J. A., Adam, M. S., de Souza, J. G., Gonçalves, R. A. (2014). Incidence of infection in orthopedic surgeries: do we actually know it? Am. J. Infect. Control 42, 461–462. doi: 10.1016/j.ajic.2013.12.007
PubMed Abstract | CrossRef Full Text | Google Scholar
Chen, W., Lv, H., Liu, S., Liu, B., Zhu, Y., Chen, X., et al. (2017). National incidence of traumatic fractures in China: a retrospective survey of 512 187 individuals. Lancet Glob Health 5, e807–e817. doi: 10.1016/S2214-109X(17)30222-X
PubMed Abstract | CrossRef Full Text | Google Scholar
Cui, Z., Liu, K., Wang, A., Liu, S., Wang, F., Li, J. (2014). Correlation between sialic acid levels in the synovial fluid and the radiographic severity of knee osteoarthritis. Exp. Ther. Med. 8, 255–259. doi: 10.3892/etm.2014.1679
PubMed Abstract | CrossRef Full Text | Google Scholar
Diaz, M. H., Waller, J. L., Napoliello, R. A., Islam, M. S., Wolff, B. J., Burken, D. J., et al. (2013). Optimization of multiple pathogen detection using the TaqMan array card: application for a population-based study of neonatal infection. PloS One 8, e66183. doi: 10.1371/journal.pone.0066183
PubMed Abstract | CrossRef Full Text | Google Scholar
Ding, X., Robbe-Masselot, C., Fu, X., Léonard, R., Marsac, B., Dauriat, C. J. G., et al. (2023). Airway environment drives the selection of quorum sensing mutants and promote Staphylococcus aureus chronic lifestyle. Nat. Commun. 14, 8135. doi: 10.1038/s41467-023-43863-2
PubMed Abstract | CrossRef Full Text | Google Scholar
Fisher, L., Srikusalanukul, W., Fisher, A., Smith, P. (2015). Liver function parameters in hip fracture patients: relations to age, adipokines, comorbidities and outcomes. Int. J. Med. Sci. 12, 100–115. doi: 10.7150/ijms.10696
PubMed Abstract | CrossRef Full Text | Google Scholar
Garcia, D. R., Deckey, D., Haglin, J. M., Emanuel, T., Mayfield, C., Eltorai, A. E. M., et al. (2019). Commonly encountered skin biome-derived pathogens after orthopedic surgery. Surg. Infect. (Larchmt) 20, 341–350. doi: 10.1089/sur.2018.161
PubMed Abstract | CrossRef Full Text | Google Scholar
Huang, G., Li, W., Zhong, Y., Liao, W., Zhang, Z. (2023). Mendelian randomization to evaluate the causal relationship between liver enzymes and the risk of six specific bone and joint-related diseases. Front. Immunol. 14. doi: 10.3389/fimmu.2023.1195553
CrossRef Full Text | Google Scholar
Jiang, N., Ma, Y.-F., Jiang, Y., Zhao, X.-Q., Xie, G.-P., Hu, Y.-J., et al. (2015). Clinical characteristics and treatment of extremity chronic osteomyelitis in southern China: A retrospective analysis of 394 consecutive patients. Med. (Baltimore) 94, e1874. doi: 10.1097/MD.0000000000001874
CrossRef Full Text | Google Scholar
Kaplan, H. B., Miranda, J. A., Gogola, G. R., Gomez, K., Ambrose, C. G. (2018). Persistence of bacterial DNA in orthopedic infections. Diagn. Microbiol. Infect. Dis. 91, 136–140. doi: 10.1016/j.diagmicrobio.2018.01.009
PubMed Abstract | CrossRef Full Text | Google Scholar
Kavanagh, N., Ryan, E. J., Widaa, A., Sexton, G., Fennell, J., O’Rourke, S., et al. (2018). Staphylococcal osteomyelitis: disease progression, treatment challenges, and future directions. Clin. Microbiol. Rev. 31, e00084–e00017. doi: 10.1128/CMR.00084-17
PubMed Abstract | CrossRef Full Text | Google Scholar
Kawaguchi, K., Nakamura, T., Wada, A., Takamura, K., Yanagida, H., Yamaguchi, T. (2022). The recent bacterial etiology of childhood osteoarticular infections focusing on the vaccine initiation for Streptococcus pneumoniae and Haemophilus influenzae: A single-center retrospective analysis in Japan. J. Orthop 31, 6–12. doi: 10.1016/j.jor.2022.03.001
PubMed Abstract | CrossRef Full Text | Google Scholar
Kodani, M., Yang, G., Conklin, L. M., Travis, T. C., Whitney, C. G., Anderson, L. J., et al. (2011). Application of TaqMan low-density arrays for simultaneous detection of multiple respiratory pathogens. J. Clin. Microbiol. 49, 2175–2182. doi: 10.1128/JCM.02270-10
PubMed Abstract | CrossRef Full Text | Google Scholar
Kuo, F.-C., Chien, C.-C., Lee, M. S., Wang, J.-W., Lin, P.-C., Lee, C.-H. (2020). Rapid diagnosis of periprosthetic joint infection from synovial fluid in blood culture bottles by direct matrix-assisted laser desorption ionization time-of-flight mass spectrometry. PloS One 15, e0239290. doi: 10.1371/journal.pone.0239290
PubMed Abstract | CrossRef Full Text | Google Scholar
Li, K., Cao, W.-W., Chen, S.-H., Zhang, B.-F., Zhang, Y.-M. (2023). Association between total cholesterol and all-cause mortality in geriatric patients with hip fractures: A prospective cohort study with 339 patients. Adv. Clin. Exp. Med. doi: 10.17219/acem/169795
CrossRef Full Text | Google Scholar
Liebling, M. R., Arkfeld, D. G., Michelini, G. A., Nishio, M. J., Eng, B. J., Jin, T., et al. (1994). Identification of Neisseria gonorrhoeae in synovial fluid using the polymerase chain reaction. Arthritis Rheum 37, 702–709. doi: 10.1002/art.1780370514
PubMed Abstract | CrossRef Full Text | Google Scholar
Liu, J., Gratz, J., Amour, C., Nshama, R., Walongo, T., Maro, A., et al. (2016a). Optimization of quantitative PCR methods for enteropathogen detection. PloS One 11, e0158199. doi: 10.1371/journal.pone.0158199
PubMed Abstract | CrossRef Full Text | Google Scholar
Liu, M., Ji, S., Yang, C., Zhang, T., Han, N., Pan, Y., et al. (2022b). Prealbumin as a nutrition status indicator may be associated with outcomes of geriatric hip fractures: a propensity score matching and 1-year follow-up study. Aging Clin. Exp. Res. 34, 3005–3015. doi: 10.1007/s40520-022-02243-4
PubMed Abstract | CrossRef Full Text | Google Scholar
Liu, J., Kabir, F., Manneh, J., Lertsethtakarn, P., Begum, S., Gratz, J., et al. (2014). Development and assessment of molecular diagnostic tests for 15 enteropathogens causing childhood diarrhoea: a multicentre study. Lancet Infect. Dis. 14, 716–724. doi: 10.1016/S1473-3099(14)70808-4
PubMed Abstract | CrossRef Full Text | Google Scholar
Liu, J., Ochieng, C., Wiersma, S., Ströher, U., Towner, J. S., Whitmer, S., et al. (2016b). Development of a TaqMan array card for acute-febrile-illness outbreak investigation and surveillance of emerging pathogens, including ebola virus. J. Clin. Microbiol. 54, 49–58. doi: 10.1128/JCM.02257-15
PubMed Abstract | CrossRef Full Text | Google Scholar
Liu, J., Platts-Mills, J. A., Juma, J., Kabir, F., Nkeze, J., Okoi, C., et al. (2016c). Use of quantitative molecular diagnostic methods to identify causes of diarrhoea in children: a reanalysis of the GEMS case-control study. Lancet 388, 1291–1301. doi: 10.1016/S0140–6736(16)31529-X
PubMed Abstract | CrossRef Full Text | Google Scholar
Liu, J., Xu, X., Lv, X., Shen, G. (2022a). Correlation between surgical site infection and time-dependent blood platelet count in immunocompromised patients after femoral neck fracture. J. Int. Med. Res. 50 (1), 3000605211068689. doi: 10.1177/03000605211068689
PubMed Abstract | CrossRef Full Text | Google Scholar
Long, H., Zeng, X., Liu, Q., Wang, H., Vos, T., Hou, Y., et al. (2020). Burden of osteoarthritis in China 1990–2017: findings from the global burden of disease study 2017. Lancet Rheumatol 2, e164–e172. doi: 10.1016/S2665-9913(19)30145-6
PubMed Abstract | CrossRef Full Text | Google Scholar
Metsemakers, W. J., Morgenstern, M., McNally, M. A., Moriarty, T. F., McFadyen, I., Scarborough, M., et al. (2018). Fracture-related infection: A consensus on definition from an international expert group. Injury 49, 505–510. doi: 10.1016/j.injury.2017.08.040
PubMed Abstract | CrossRef Full Text | Google Scholar
Metsemakers, W.-J., Moriarty, T. F., Morgenstern, M., Marais, L., Onsea, J., O’Toole, R. V., et al. (2023). The global burden of fracture-related infection: can we do better? Lancet Infect. Dis., S1473–3099(23)00503–0. doi: 10.1016/S1473–3099(23)00503–0
CrossRef Full Text | Google Scholar
Moore, C. C., Jacob, S. T., Banura, P., Zhang, J., Stroup, S., Boulware, D. R., et al. (2019). Etiology of sepsis in Uganda using a quantitative polymerase chain reaction-based TaqMan array card. Clin. Infect. Dis. 68, 266–272. doi: 10.1093/cid/ciy472
PubMed Abstract | CrossRef Full Text | Google Scholar
Morgenstern, C., Cabric, S., Perka, C., Trampuz, A., Renz, N. (2018). Synovial fluid multiplex PCR is superior to culture for detection of low-virulent pathogens causing periprosthetic joint infection. Diagn. Microbiol. Infect. Dis. 90, 115–119. doi: 10.1016/j.diagmicrobio.2017.10.016
PubMed Abstract | CrossRef Full Text | Google Scholar
Pneumonia Etiology Research for Child Health (PERCH) Study Group. (2019). Causes of severe pneumonia requiring hospital admission in children without HIV infection from Africa and Asia: the PERCH multi-country case-control study. Lancet 394 (10200), 757–779.
PubMed Abstract | Google Scholar
Premkumar, A., Kolin, D. A., Farley, K. X., Wilson, J. M., McLawhorn, A. S., Cross, M. B., et al. (2021). Projected economic burden of periprosthetic joint infection of the hip and knee in the United States. J. Arthroplasty 36, 1484–1489.e3. doi: 10.1016/j.arth.2020.12.005
PubMed Abstract | CrossRef Full Text | Google Scholar
Talsnes, O., Hjelmstedt, F., Dahl, O. E., Pripp, A. H., Reikerås, O. (2012). Biochemical lung, liver and kidney markers and early death among elderly following hip fracture. Arch. Orthop Trauma Surg. 132, 1753–1758. doi: 10.1007/s00402-012-1611-7
PubMed Abstract | CrossRef Full Text | Google Scholar
Wang, V. T. J., Tan, J. H., Pay, L. H., Wu, T., Shen, L., O’Neill, G. K., et al.
留言 (0)