
記住我




The UKB is a large population-based prospective cohort study conducted in 22 assessment centers throughout the UK. Between 2006 and 2010, the UKB recruited more than 500,000 participants aged 40–69 years from the general population. Baseline demographic and lifestyle information was collected via a self-completed touchscreen questionnaire, and anthropometric measurements were taken by trained staff. A detailed description of the UKB project is reported elsewhere [25]. The UKB research was approved by the Northwest Multicenter Research Ethical Committee (reference number: 11/NW/0382). All participants provided written informed consent for the study.
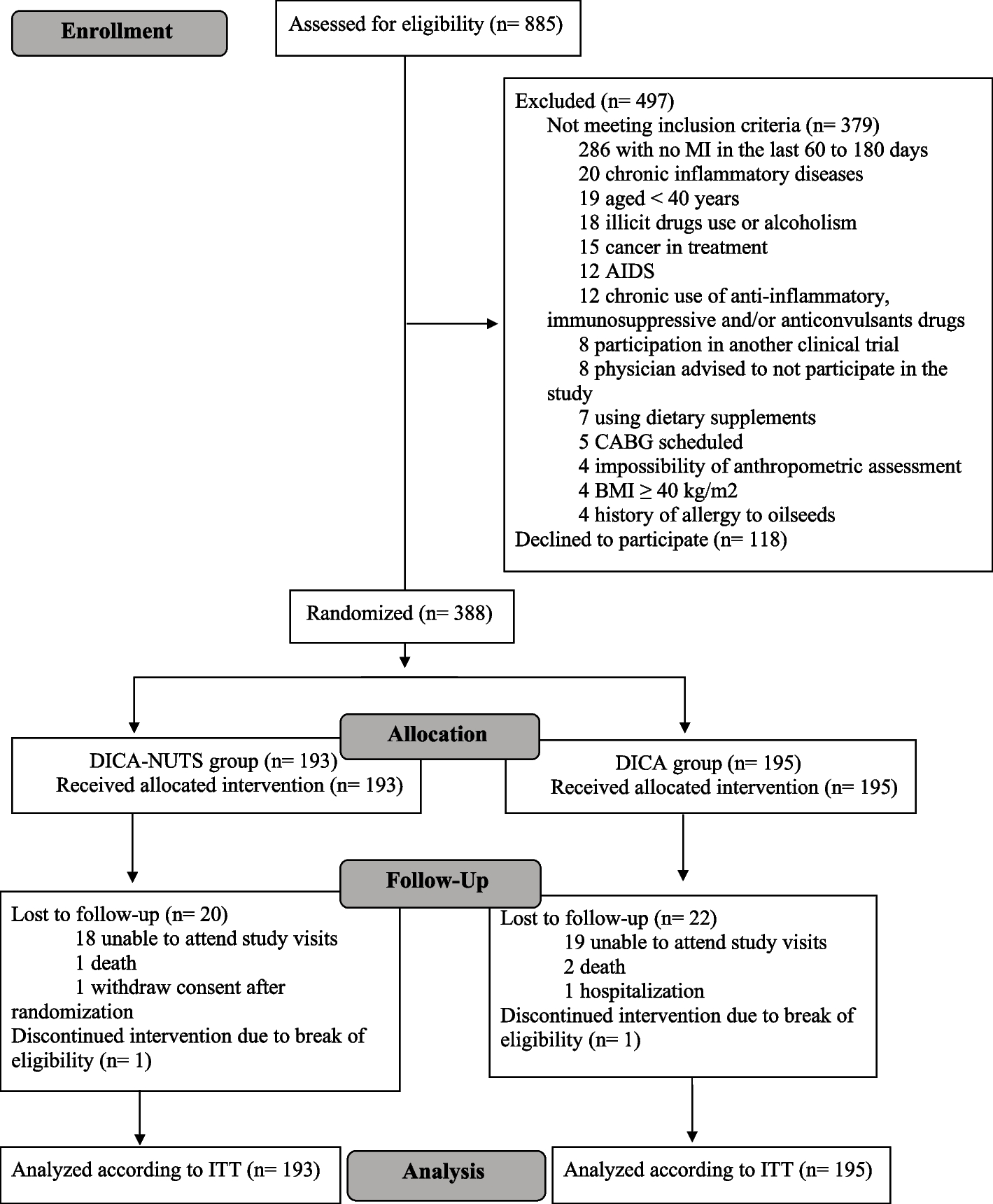
Data from 502,492 participants were available for our study. Participants with SLE at baseline were excluded (n = 764). We also excluded participants with cancer at baseline (n = 38,442), those who withdrew from UKB during the follow-up (participants have withdrawn consent for future data linkage, n = 156), and those with missing data on fish oil use (n = 1,484). In this process, 461,646 participants were included. After excluding participants with missing data on other covariates (e.g. smoking status, drinking status, physical activity, history of diseases, n = 71,369), we included 390,277 participants in our analysis in the end. Details of the study sample selection are shown in Fig. 1. Detailed information on the number of missing covariates is shown in Supplementary Table S1.
Fig. 1
Flowchart for the selection of the analyzed study sample from the UK Biobank
Ascertainment of fish oil use and covariatesIn the baseline assessment, participants were asked, “Do you regularly take any of the following supplements?” through a touchscreen questionnaire. Multiple dietary items were incorporated, including fish oil use. We classified participants into fish oil user and fish oil non-user groups according to whether they selected the “fish oil (including cod liver oil)” item.
Information about other covariates was also obtained in the baseline assessment from touchscreen questionnaires or by linking to hospital inpatient records. Age, sex, race, location of assessment centers, body mass index (BMI), education, Townsend deprivation index (TDI), smoking status, alcohol drinking status, physical activity, dietary intake, vitamin supplementation use, mineral supplementation use, the use of nonsteroidal anti-inflammatory drugs (NSAIDs), history of hypertension, history of diabetes, history of hyperlipemia and ultraviolet (UV) radiation were included.
Education level was categorized as higher (College/university degree or other professional qualification), upper secondary (A levels/AS levels or equivalent), lower secondary (O-levels or Certificate of Secondary Education or equivalent), or other. BMI was calculated as the weight (kg) divided by height squared (m2), and classified into four groups based on the World Health Organization standards [26]. Socioeconomic status was reflected by using the TDI, which was calculated based on postcode-specific information on the percentages of unemployment, overcrowded households, people with no car ownership, and non-homeowners [27]. The higher the score, the higher the level of deprivation. According to the healthy physical activity recommendations from the World Health Organization [28], we classified participants into two groups based on the total time spent in moderate physical activity or vigorous physical activity in minutes each week (dichotomous variable): less than 150 min, 150 min or more per week. NSAIDs use included the use of aspirin, ibuprofen, or paracetamol. The histories of hypertension, diabetes, and hyperlipemia were defined according to self-reported information or hospital in-patient records, and detailed definitions of those diseases are shown in Supplementary Table S2. UV radiation was measured by asking, “In a typical day in summer, how many hours do you spend outdoors?” According to the definition of previous study [29], we divided participants into two groups (“<3 hours/day”, “≥3 hours/day”).
Dietary intake included 10 types of food (fruit, vegetables, whole grains, refined grains, fish, dairy, vegetable oils, processed meat, unprocessed meat, and sugar-sweetened beverages). We also constructed a healthy diet score based on the definition of ideal dietary component intake for cardiometabolic health [30]. One point was given if the intake goal was met. The detailed definitions of each type of food intake and intake goal were presented in Supplementary Table S3. The healthy diet score ranged from 0 to 10, with a higher diet score representing a healthier diet. The healthy diet score ≥ 5 was considered as an ideal diet, < 5 was considered a poor diet [30]. In analyses, we included healthy diet score as dichotomous variable (< 5, ≥ 5).
Outcome ascertainmentThe outcome of the study was the incidence of SLE. We used the data fields 131,894 and 131,895 in the UKB. These two data fields recorded all sources (primary care, hospital admission, death register, and self-report) of SLE and the first SLE occurrence date. The International Classification of Diseases version 10 (ICD-10) code M32 was used for the identification.
Statistical analysisThe baseline characteristics of participants were described as means ± standard deviation (SD) for continuous variables or numbers (percentages) for categorical variables. The follow-up time was calculated from the baseline date to the date of the first SLE occurrence, death, lost to follow-up, or last update date of the linkages (30 November 2020), whichever occurred first. Death data were obtained by linking death registry records. Lost to follow-up was defined as the inability to follow an outcome because of departure from the UK or because a relative had reported death or national datasets indicated lost to follow-up.
The association between fish oil use and SLE incidence was explored by using Cox proportional hazard models, and the hazard ratios (HR) and 95% confidence intervals (CI) were calculated. The Schoenfeld residual method was used to test the proportional hazards assumptions for the Cox model. In our analyses, no violation of this assumption was observed. Four Cox models were built. Model 1 adjusted for age and sex. Model 2 adjusted for age, sex, race, location of assessment centers, BMI, education, TDI, smoking status, alcohol drinking status, physical activity, vitamin supplementation use, mineral supplementation use, NSAIDs use, history of hypertension, history of diabetes, history of hyperlipemia, and UV radiation. Model 3 further adjusted for fruit, vegetables, whole grains, refined grains, oily fish, non-oily fish, dairy, vegetable oils, processed meat, unprocessed meat, and sugar-sweetened beverages based on Model 2. Considering the complex interactions between dietary components, we further adjusted for the healthy diet score representing the overall diet quality in model 4 based on model 2.
We performed subgroup analyses to estimate the potential modification effect according to age (< 60, ≥ 60 years), sex (male, female), race (White, non-White), BMI (< 30, ≥ 30 kg/m2), current smoking status (yes, no), current drinking status (yes, no), physical activity (< 150, ≥ 150 min/week), vitamin supplementation use (yes, no), mineral supplementation use (yes, no), NSAIDs use (yes, no), history of hypertension (yes, no), history of diabetes (yes, no), history of hyperlipemia (yes, no), oily fish (< 1, ≥ 1 times/week), non-oily fish (< 1, ≥ 1 times/week), UV radiation (< 3, ≥ 3 h/day), and healthy diet score (< 5, ≥ 5). Potential modifying effects were assessed by modeling the cross-product term of the stratifying variable with fish oil use. As females are a high-risk group for SLE [31], to explore whether these stratifying variables have modifying effects in female group, we also conducted subgroup analysis and calculated p for interaction in the female group.
We performed a sensitivity analysis by excluding participants who developed SLE during the first two years of follow-up to test the robustness of our study and minimize the influence of reverse causation. Based on the previous evidence that showed some female factors related to the risk of SLE [32], we further adjusted for age at menarche (≤ 10 years, > 10 years), oral contraceptive use (yes, no), menopause status (yes, no, not sure), and hormone-replacement therapy used (yes, no) in the female group for sensitivity analysis. In addition, we further tested the robustness of the results by performing sensitivity analyses adjusting for the use of sun protection measures (never/rarely, sometimes, most of the time, always, do not go out in sunshine). The measuring methods of these five potential covariates (age at menarche, oral contraceptive use, menopause status, hormone-replacement therapy used, sun protection measures) are shown in Supplementary Table S4.
All analyses were performed using Stata (version 16) and R (version 4.1.1). Statistical significance was defined as a two-sided p-value < 0.05.
留言 (0)