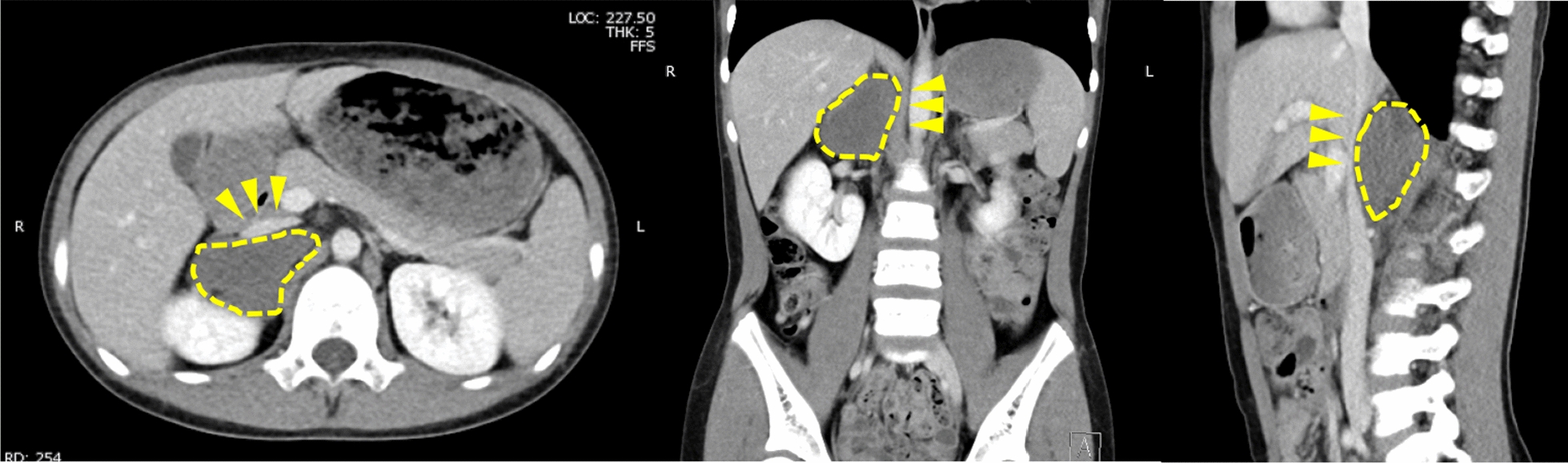
SMA occlusion is a condition characterized by obstruction of the SMA by an embolus or thrombus, leading to extensive intestinal ischemia affecting both the small and large intestines. Unless promptly treated, SMA occlusion carries a high mortality rate [1]. Thrombosis leading to SMA occlusion may arise from emboli originating from the heart, such as the LAA, or from atherosclerosis or stenosis of the mesenteric artery [2]. Despite advancements in medical management for facilitating early diagnosis and intervention, the mortality rate of SMA occlusion remains alarmingly high, ranging from 60 to 80%, thus it is associated with a generally poor prognosis [4, 5].
Presently, a range of anticoagulant options, including direct oral anticoagulant (DOAC) administration, is available for prevention of thromboembolism in patients with AF. However, absorption of anticoagulants primarily occurs in the stomach and proximal small intestine [6,7,8]. Following extensive resection of the small intestine, notable structural and functional changes are known to occur in the remaining intestinal tract, including dilatation, wall thickening, alterations in villi morphology, and increased expression of sodium–glucose cotransporter 1 (SGLT-1) [9]. Such alterations can significantly impact drug absorption, including anticoagulants. Additionally, many of the anticoagulants available, including DOACs, lack easily accessible methods for monitoring in the bloodstream.
Buchholz et al. [10] reported that a functional small bowel length of 60 cm or more is advantageous for use of rivaroxaban. However, even a vitamin K antagonist such as warfarin, which can be monitored, poses challenges for achieving therapeutic control due to absorption issues. Therefore, when devising a medication regimen, careful considerations regarding overall health and nutritional status of the patient, as well as laboratory parameters, treatment efficacy, potential side effects, and other pertinent factors are imperative. Fortunately, both of the present patients had greater than 100 cm of the small intestine remaining. Nevertheless, they were subsequently presented with compromised renal function, necessitating management with warfarin, though their anticoagulation monitoring values remained markedly unstable despite treatment.
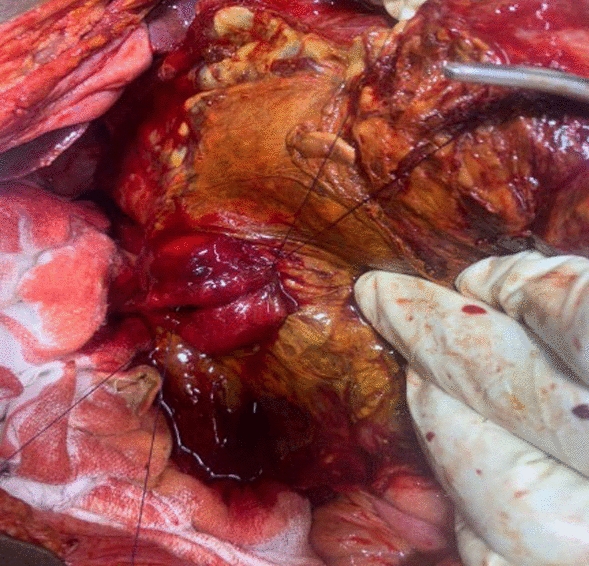
Given the aforementioned challenges, discontinuation of anticoagulation therapy in both cases became necessary, thus necessitating meticulous and dependable management of the LAA. In 2003, thoracoscopic left atrial appendage resection emerged as a non-pharmacological intervention procedure for left atrial thrombus. This technique effectively mitigates the risk of embolism in patients with non-valvular AF in the short term, with no observed neurological complications [11]. Furthermore, a report by Ohtsuka et al. presented a left thoracoscopic stapler left atrial appendage resection method that facilitates stapler insertion at an optimal angle, resulting in a precise dissection plane [12]. This approach permits additional loop procedures on the dissected surface, rendering it as an optimal technique for achieving comprehensive left atrial appendage management.
In the present two patients, transcutaneous catheter-based ablation was deemed inappropriate for two primary reasons. Firstly, anticoagulation is necessary post-catheter ablation until endothelial lesions have healed [13]. Conversely, the technique employed in these cases is known to rapidly isolate the PV from the epicardial side, thus minimizing endothelial damage [14]. Second, while AF may recur, affected patients face renewed risk of thromboembolism, which is particularly heightened with advancing age. Although AF recurrence remains a possibility in our patients, the continued low thromboembolic risk is attributed to removal of the LAA. While transcutaneous implantation of an LAA-closure device, such as Watchman or Amplatzer, might have been considered, the present straightforward cutting method was deemed preferable due to reported instances of clot formation on such devices, thus necessitating ongoing anticoagulant therapy [15, 16]. Despite this, both patients received warfarin treatment for 3–4 weeks. The procedure involved temporary myocardial blockade, such as pulmonary vein isolation with Atricure and left ventricular closure with Stapler. While minimal endocardial damage may occur, inflammation at the site is expected to persist. Indeed, Inoue et al. [17] reported a 15.8% incidence of thrombus formation near the LAA during the acute phase of LAA closure using a stapler. Although the clinical significance remains unclear, our department follows a protocol of administering empirical anticoagulation for approximately one month until contrast-enhanced CT confirms a thrombus-free closure area in the left atrium, as we routinely perform. The protocol essentially dictates discontinuing anticoagulation after 1 month, regardless of residual atrial fibrillation, upon obtaining contrast-enhanced CT images indicating a clear absence of thrombus, as demonstrated in the two patients. Further evidence in this area is warranted. In this context, thoracoscopic left atrial appendage closure emerges as an exceptionally favorable procedure, offering robust closure management and facilitating the gradual cessation of anticoagulation therapy. In 2018, a total of 201 patients in Japan underwent thoracoscopic LAA resection (Wolf–Ohtsuka procedure) [18]. Over a mean follow-up period of 48 months (range 12–110 months) after completion of anticoagulation therapy, only two developed cardiogenic thromboembolisms, translating to 0.25 events per 100 patient-years. Based on those findings, we propose this method as a viable option for preventing recurrence of ischemic stroke in patients with left atrial appendage thrombus refractory to medical therapy. Despite its invasiveness and the necessity of general anesthesia in contrast to other LAA management techniques, the procedure offers the advantages of a small incision (eliminating the need for cardiopulmonary bypass) and a brief operative duration. We propose this approach as a viable strategy for mitigating the risk of recurrent ischemic strokes in such patients.
In the two cases presented here, we were fortunate enough to successfully restore the patients to sinus rhythm through pulmonary vein isolation alone. Although pulmonary vein isolation is typically effective for paroxysmal atrial fibrillation, its efficacy diminishes for persistent cases, where extensive myocardial ablation via the maze procedure, as advocated by Cox et al. [19], proves superior. However, in the context of the two cases under study, the primary objective is the prevention of embolism and the gradual discontinuation of anticoagulant therapy through LAA management, with achieving perfect sinus rhythm being of secondary importance. Moreover, the invasiveness associated with a full maze procedure utilizing artificial heart–lung support would be more than twice as high, prompting the present study to confine its intervention to rhythm therapy within the scope of thoracoscopic manipulation. Another advantage of this treatment is its flexibility. In the event of atrial fibrillation recurrence, a hybrid approach is available, permitting a second attempt at rhythm therapy through supplementary catheter ablation. In these two cases, we were fortunate to achieve sinus rhythm solely through bilateral pulmonary vein isolation. However, if maintaining sinus rhythm became problematic, we had a plan to explore the option of additional catheter ablation postoperatively.









留言 (0)