Dual Maternal Alloimmunization by Antibodies of Rhesus and MNSs Blood Group System: Case Series and Approach to Work Up in a Resource Limited Set Up
Backgrounds and Objectives
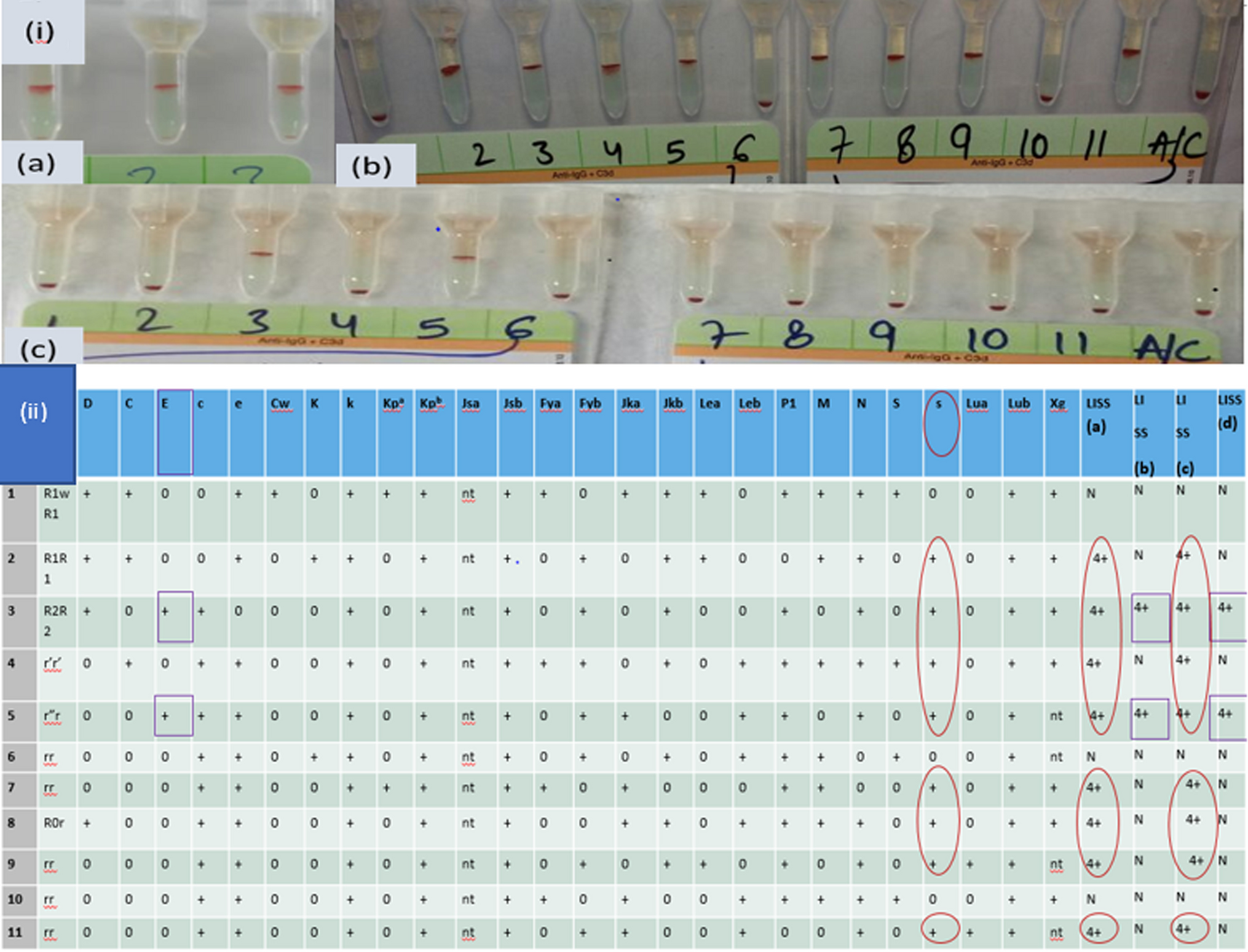
Maternal alloimmunisation by non D Rh and non Rh antibodies leading to HDFN, is a well established problem encountered in Transfusion medicine and poses a serious threat to our health care system. Presence of multiple alloantibodies, especially if one is masking the other, leads to diagnostic dilemma and delay in transfusion therapy of patients. It is significant to correctly identify highly immunogenic alloantibody specificities in such patients with dual and multiple alloimmunization, by use of various immunohematological techniques.
Case Series
Here, we report three rare and interesting cases. In the first case, anti E was masked by anti s, and lead to HDFN in a neonate due to maternal alloimmunisation. The second case was that of anti S causing severe HDN along with probable presence of anti E. In third case, anti D was masked by anti M, leading to maternal alloimmunization. In the first two cases, both neonates were treated by intravenous immunoglobulins and the latter received DVET. While in the third case, alloimmunization was timely detected during the pregnancy and monitoring of maternal antibody titres was done, ensuring delivery of a healthy baby. After extensive search of literature, we found only one report describing coexistence of anti E and s in a newborn, with baby’s eluate showing only anti s. However, despite being IgG type, it did not cause hemolysis. Literature search revealed that Anti S is a rare cause of HDFN and usually presents as mild jaundice. We did not come across any combination of anti S with anti E, after searching the literature. After extensive search of literature, we came across a single case of dual alloimmunization by anti M obscuring anti D.
Interpretations and Conclusion
The above cases highlight the importance of universal antenatal antibody screening despite Rh D status. It is important to look for clinically significant alloantibodies other than anti-D and correctly identify the culprit antibody, especially, when it is masked by the other multiple alloantibodies. Non D Rh minor blood group incompatibilities e.g. anti-E and anti S or anti s hemolytic disease, should always be considered in the differential diagnosis. A stepwise approach for antibody identification and advanced immunohematological techniques including the use of select cells and adsorption elution methods, can help in elucidating the specificities of antibodies.









留言 (0)