
記住我




A total of 256 patients were included in this analysis, with 92 CAR-T, 55 BsAb and 109 ADC-treated patients. Fifty-seven percent, 56% and 18% of CAR-T, BsAb and ADC patients were treated on clinical trials, respectively. The baseline characteristics of patients that received T-cell redirecting therapies (CAR-T and BsAb) are summarized in Table 1. The median age of patients treated with CAR-T was 62 years (interquartile range [IQR]: 56−69 years) compared to 65 years (IQR: 58−72 years) in the BsAb treated group (P = 0.043). Patients treated with CAR-T received a median of 7 prior lines of therapy (IQR: 5−8) compared to a median of 6 prior lines of therapy (IQR: 4−9) with BsAb. Nearly all patients in the CAR-T arm had a prior autologous transplant (97%), compared to 75% in the BsAb arm (P < 0.001). Thirty-three percent of patients in the BsAb group had prior exposure to CAR-T, whilst only 1% in the CAR-T cohort had prior BsAb exposure.
Table 1 Baseline characteristics of patients who received T-cell redirecting therapies.Incidence and grade of severe infections in recipients of CAR-T and BsAbThe median follow-up duration for infection-specific events was similar in patients that received T-cell redirecting therapies, with a median follow-up of 5.8 months (IQR: 3.7−9.2 months) in the CAR-T arm compared to 4.3 months (IQR: 3.2−9.8 months) in the BsAb arm.
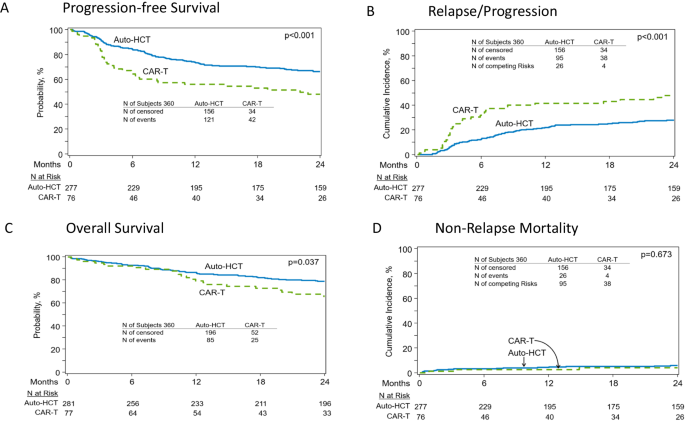
A total of 214 infectious events were reported, with 115 after CAR-T and 99 after BsAb. Forty percent of CAR-T recipients and 27% of BsAb recipients had no infections reported during the follow-up period. Regarding the primary endpoint, the incidence of severe (grade ≥3) infections was numerically lower with CAR-T with 26% of patients experiencing severe infections compared to 40% with BsAb (hazard ratio [HR] 0.58, 95% confidence interval [CI] 0.32−1.04, P = 0.067) – Fig. 1.
Fig. 1
Estimated cumulative incidence of grade ≥3 infections over time.
After adjusting for pretherapy variables, the multivariable analysis demonstrated a lower risk for time to first severe infections with CAR-T compared to BsAb, but this did not reach statistical significance (HR 0.60, 95% CI 0.31−1.17, P = 0.14) – Table 2. Pretherapy variables including patient age, triple/penta-refractory status, prior receipt of BCMA-targeted therapy and baseline lymphopenia or hypogammaglobulinemia did not predict for severe infection on multivariable analysis in the entire cohort. However, within the CAR-T cohort, baseline lymphopenia (prior to lymphodepleting chemotherapy) was associated with a higher risk for severe infection (HR 2.82, 95% CI 1.18−6.72, P = 0.02). We did not assess for baseline neutropenia as there were very few patients with pretherapy neutropenia in both cohorts (baseline neutropenia in CAR-T: 1% and BsAb: 6%).
Table 2 Multivariable cause-specific Cox regression of baseline characteristics for time to first severe infections.Of the 26% of CAR-T patients with severe infections, all experienced only grade 3 infections, and there were no grade 4 or 5 events in the CAR-T cohort. In the BsAb group, 40% experienced grade 3 infections, 4% had grade 4 infections and 7% experienced grade 5 infections – Table 3. Seven percent of patients in the CAR-T arm and 20% in the BsAb arm experienced >1 severe infection.
Table 3 Primary study endpoint of severe (grade ≥3) infections.In case dual exposure to both BsAb and CAR-T may have impacted the study findings, the 18 patients within the BsAb arm that received prior CAR-T were excluded, and the analysis was repeated for the primary endpoint. The baseline characteristics of this subset of patients is included in Supplemental Table 1A. Of the 37 patients treated with BsAb and who did not receive prior CAR-T, the median follow-up duration was 4.7 months (IQR 3.5−10.9 months) during which there were a total of 81 infections reported. The incidence of ≥ 1 severe infection remained high at 46%, including 5% of patients experiencing grade 4 infections, and 8% having grade 5 infections. Of the 18 BsAb recipients who received prior CAR-T, a total of 18 infections were reported, of which there were 28% grade 3, 0% grade 4, and 6% grade 5 infections (Supplemental Table 1B).
Regarding any-grade infections in the entire cohort, there was no significant difference in the infection incidence between BsAb and CAR-T on both univariable and multivariable analysis – Supplemental Table 2. The median time to the first infectious event of any-grade was shorter at 2.5 months (95% CI 1.2 – not reached [NR]) post-CAR-infusion compared to 3.1 months (95% CI 1.2−5.5 months) after the initiation of BsAb.
Comparison to severe infections with ADCA cohort of 109 patients treated with BCMA-directed ADCs were used as a control to assess the infection risk with BCMA-directed ADCs in a similarly heavily pretreated patient population. The baseline characteristics of this patient population are provided in Supplemental Table 3 and were overall comparable to both the CAR-T and BsAb groups with a median age of 67 years (IQR 61−73 years), median of 6 (IQR 5−8) prior lines of therapy and 78% having received a prior autologous stem cell transplant.
The median follow-up duration for infection-specific events was 3.8 months (IQR 1.4−8.7 months) during which time there was a total of 31 infections reported. The incidence of severe infections in patients treated with ADC was low at 8% - Table 3. There was 1 grade 4 infection, and 0 grade 5 infections. Pretherapy patient or disease characteristics did not predict for infection in this cohort.
Infection rates over time in the CAR-T and BsAb recipientsIn univariable analysis, there was no significant difference in the incidence rate of severe infections up to 100-days post CAR-T compared to 100-days post BsAb (incidence rate ratio [IRR]: 1.11, 95% CI 0.55−2.39, P = 0.8), and this was maintained in a multivariable analysis adjusting for the baseline covariates (IRR 1.58, 95% 0.68−3.89, P = 0.3). Similarly, there was no significant difference in incidence rate of severe infections between the two groups up to 6-months post treatment initiation. However, when extending the follow-up to 1-year, there was a significantly lower incidence rate for severe infections with CAR-T compared to BsAb (IRR 0.45, 95% CI 0.27−0.74, P = 0.002), and this was maintained in a multivariable analysis (IRR 0.43, 95% CI 0.25−0.76, P = 0.004) – Table 4. Notably, 79% of first severe infections occurred within day-100 post CAR-infusion in the CAR-T arm compared to only 50% occurring within the first 100 days after commencement of BsAb. Together, these findings suggest that the risk of severe infections is prolonged with BsAb compared to CAR-T.
Table 4 Multivariable analysis of severe infections up to the 1st year follow-up post-therapy.Similar findings were also observed when assessing the incidence rate of any-grade infections between the two groups.
Impact of treatment-emergent hypogammaglobulinemia on infectionsFirst, we assessed the impact of treatment-emergent hypogammaglobulinemia on incidence rates of severe infections. The proportion of time that patients experienced treatment-emergent hypogammaglobulinemia was similar in the BsAb and CAR-T arms – Fig. 2. CAR-T recipients appeared to have a lower incidence rate of severe infections than BsAb recipients during these periods of hypogammaglobulinemia (IRR at 6-months 0.61, 95% CI 0.33−1.14, P = 0.11) - Supplemental Table 4A. When extending the follow-up to 1-year, the difference was statistically significant (IRR 0.44, 95% CI 0.25−0.76, P = 0.004). Similarly, a lower incidence rate of any-grade infections was also observed with CAR-T compared to BsAb during periods of treatment-emergent hypogammaglobulinemia (IRR at 6 months 0.65, 95% CI 0.45−0.95, P = 0.025: IRR at 12 months 0.55, 95% CI 0.40−0.77, P < 0.001). During periods of non-hypogammaglobulinemia, the lower severe infection rate that was seen with CAR-T did not reach statistical significance (IRR at 1-year 0.46, 95% CI 0.13−1.54, P = 0.2) – Supplemental Table 4B. Within both the CAR-T and BsAb arms, there appeared to be no significant difference in the IRR for severe infections during periods of hypogammaglobulinemia compared to periods of non-hypogammaglobulinemia – Supplemental Table 4C.
Fig. 2: Functional serum IgG levels over time after treatment initiation up to 6 months of follow up.
The x-axis represents individual patients. The colored bars report the number of days within the 1st 6-months during which each patient experienced functional hypogammaglobulinemia (IgG < 400 mg/dL) or non-hypogammaglobulinemia (IgG ≥ 400 mg/dL).
Next, we assessed the impact of treatment-emergent hypogammaglobulinemia on time to first infection within each treatment arm. The presence of hypogammaglobulinemia appeared to be associated with a higher incidence of severe infections than non-hypogammaglobulinemia, but it was not statistically significant in both cohorts (CAR-T - HR 1.44, 95% CI 0.53−3.93, P = 0.5; BsAb - HR 1.37, 95% CI 0.46−4.07, P = 0.6) – Supplemental Table 5A. We then compared CAR-T to BsAb and here we found that the incidence of severe infections in the CAR-T cohort was significantly lower than BsAb during periods of hypogammaglobinemia (HR 0.49, 95% CI 0.25−0.96, P = 0.036) Supplemental Table 5B. Similarly, during periods of post-therapy hypogammaglobulinemia, patients in the CAR-T cohort had significantly lower incidence of any-grade infections compared to BsAb (HR 0.51, 95% CI 0.31−0.83, P = 0.007) – Supplemental Table 5C. There was no significant difference in severe infection risk during periods of non-hypogammaglobulinemia (HR 0.77, 95% CI 0.21−2.78, P = 0.7) – Supplemental Table 5B.
Together, these results suggest that presence of hypogammaglobulinemia may have a more profound impact on infection risk with BsAb as compared to CAR-T. Notably, of the 7% of patients within the BsAb arm that experienced grade 5 infections, the most recent IgG level available prior to the onset of the grade 5 infectious event was <200 mg/dL in all these patients.
Impact of treatment-emergent neutropenia on infectionsPost-therapy neutropenia was more common in recipients of CAR-T compared to BsAb recipients – Fig. 3. The presence of neutropenia was associated with a significantly higher incidence rate of severe infections with CAR-T when compared to periods of non-neutropenia (IRR 2.68, 95% CI 1.14−6.31, P = 0.024) in the first 100-days post treatment initiation. There was also a higher incidence rate of severe infections during periods of neutropenia with BsAb within the first 100 days, but this was not statistically significant (IRR 3.45, 95% CI 0.75−16.00, P = 0.11). Given as severe infections predominantly occurred in the first 100-days post treatment initiation with CAR T-cell therapy, this suggests that periods of neutropenia during the first 100-days may have a more profound impact on severe infection rate in the setting of CAR-T. Periods of post-therapy neutropenia continued to be associated with a significantly higher incidence rate of severe infection at follow-up that extended to 6-months (IRR 3.40, 95% CI 1.47−7.83, P = 0.004) and 1-year in CAR-T recipients (IRR 4.32, 95% CI 1.85−10.1, P < 0.001). For recipients of BsAb, the presence of neutropenia at 6-months (IRR 2.93, 95% CI 0.93−2.93, P = 0.066) and 1-year (IRR 2.85, 95% CI 1.02−7.96, P = 0.046) also appeared to affect the rate of severe infections and reached significance at 1-year follow-up – Supplemental Table 6A. We also tested for differences in the incidence rate for severe infections within periods of post-therapy neutropenia in the CAR-T compared to BsAb cohort and found that the incidence rate was lower with CAR-T, but this difference was not statistically significant (IRR at 100-days follow-up: 0.67, 95% CI 0.18−4.30, P = 0.6) – Supplemental Table 6B.
Fig. 3: Absolute neutrophil count over time after treatment initiation up to 6 months of follow up.
The x-axis represents individual patients. The colored bars report the number of days within the 1st 6-months during which each patient experienced neutropenia (neutrophil count <1000/mcL) or non-neutropenia (neutrophil count ≥1000/mcL).
Notably, during periods of post-therapy non-neutropenia at 1-year follow-up, CAR-T recipients had a significantly lower infection rate compared to BsAb (IRR 0.32, 95% CI 0.17−0.59, P < 0.001) – Supplemental Table 6C. Similarly, during periods of post-therapy non-neutropenia, CAR-T recipients had a significantly lower time to infection compared to BsAb recipients (HR 0.44, 95% CI 0.21−0.93, P = 0.032) – Supplemental Table 7A.
Infection typesIn CAR-T recipients, the proportion of any-grade bacterial, viral, fungal, and parasitic infections was 49%, 48%, 4 and 1%, respectively. In BsAb recipients, the proportion of bacterial, viral, fungal, and parasitic infections was 53%, 42%, 3% and 0, respectively. The two grade 4 infections in the BsAb arm were COVID-19 infection and Stenotrophomonas maltophilia pneumonia. Of the four grade 5 infections in the BsAb cohort, three were bacterial pneumonia (1 Klebsiella pneumoniae, 2 Pseudomonas aeruginosa) and one bacteremia (Klebsiella aerogenes). Grade 5 events occurred between day 30 to day 334 of BsAb initiation.
Infections were most common in the respiratory tract in both cohorts. The proportion of bloodstream, upper respiratory, lower respiratory, gastrointestinal, genitourinary, skin/soft tissue, and other infections was 15%, 40%, 14%, 16%, 11%, 7 and 3%, respectively in the CAR-T arm compared to 9%, 49%, 13%, 9%, 9%, 4 and 5%, respectively in the BsAb treated arm. Grade ≥3 opportunistic infections or viral reactivation syndromes accounted for 1% (1 cytomegalovirus reactivation) of all CAR-T infections, and 4% of BsAb infections (1 Pneumocystis pneumonia, 1 cytomegalovirus reactivation, 1 herpes simplex and 1 varicella zoster viral infection). Further details of the infection site, grades and organisms are provided in Supplemental Tables 8 and 9.
留言 (0)