Even with optimal patient selection, tumor characteristics, and treatment considerations, a majority of patients with initially resected pancreatic cancer have disease progression with either locoregional and/or distant failure. A retrospective review from the Johns Hopkins Hospital demonstrates 76.7% of patients had recurrence, with 23.7% developing local recurrence only [24]. Examination of patterns of local recurrence from ESPAC-4, a large multicenter clinical trial, demonstrated 65.6% disease recurrence of the 730 patients that underwent initial resection, with only local recurrence in approximately half of patients with recurrence [5]. These results emphasize both the need for improved up-front treatment paradigms, as well as effective tools for the treatment of recurrences when they occur.
Local control is crucial in pancreatic cancer, as evidenced by published data indicating that 30% of patient deaths result from local disease progression [25]. There are no clear guidelines for the treatment of LR-PAC, with re-resection, chemotherapy alone, chemoradiation, and SBRT all being potential therapies. There is a lack of prospective clinical trial data to determine optimal treatment modalities, however re-resection appears to have the best outcomes with a significant survival benefit [3, 4, 7, 8, 26]. A systematic review by Groot et al. identified the best survival outcomes with re-resection at 32 months, while chemoradiotherapy and SBRT are similar at 19 and 16 months, respectively [4]. Reoperation is a safe an effective option in a carefully selected group of patients [26]. That being said, patients with LR-PAC that are amenable to re-resection make up a small subset of the population. Chemoradiation for LR-PAC as a means to re-resection has also been explored previously with Habermehl et al. reporting on retrospective outcomes in 41 patients undergoing fractionated chemoradiotherapy. Treatment was well tolerated, however only 12% were able to undergo re-resection and only 15% had complete response with chemoradiation further highlighting the need for improved local therapy in LR-PAC [7].
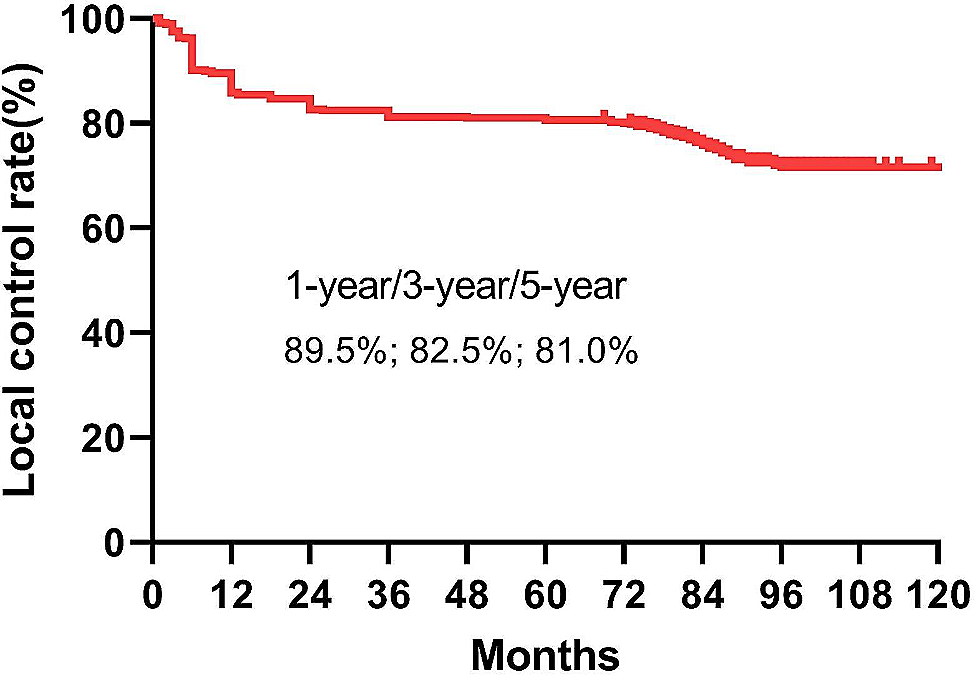
SBRT is an attractive treatment option given that it can be completed quickly while achieving biologic equivalent doses similar to long course chemoradiation [9]. The majority of published data regarding SBRT for pancreatic cancer pertains to locally advanced or unresectable disease, with SBRT for LR-PAC being sparse. A small study by Reddy et al. demonstrated in a cohort of 19 radiation naïve patients with LR-PAC, that SBRT is safe and feasible with a mean BED10 of 54.8 Gy. Despite relative safety in this challenging patient population, 1 patient experienced gastric perforation and almost 50% experienced local failure, with BED < 54.8 Gy being associated with inferior local control [13]. Several other small cohorts of patients treated with SBRT for LR-PAC have been reported on with variable SBRT dosing and local control outcomes. A few studies reporting on treatment with conservative SBRT doses to a median 24 or 25 Gy had good toxicity outcomes, however they demonstrated relatively poor local control of 56–78% at 6 months and 19–72% at 12 months [11, 14, 15]. Meng et al. had the highest treatment dose for SBRT to a median of 45 Gy (42–50 Gy) for 19 patients, with the best reported local control at 6 months of 95%, although control declined significantly to 45% at 12 months [12]. Despite variation among the trials in patient population, prior therapies, and SBRT dosing for LR-PAC, overall survival did not vary significantly among these trials ranging from 9 to 13 months [11, 12, 14, 15]. Although the local control of 83.9% at 1 year for LR-PAC treated with MRgSBRT is an improvement from prior studies of SBRT for LR-PAC, it similar to published data for borderline and unresectable primary disease with studies demonstrating a local control of 82.4–82.9% [22, 23].
The results from our small cohort of LR-PAC that underwent MRgSBRT demonstrate excellent safety and toxicity, with no grade 3 toxicities even among patients with prior radiation. This is comparable to prior published data on SBRT in LR-PAC, even when compared to much more conservative doses in non-MRgSBRT [11, 13,14,15]. Although overall survival with our patient cohort is similar to prior literature, this is unsurprising. Even among prior SBRT data for LR-PAC, the survival following initiation of SBRT varies significantly. Interestingly, in examination of recurrence pattern in ESPAC-4, there was no significant difference in overall-survival between local and distant recurrence following disease recurrence, with median survival of 9.5 and 9.4 months, respectively. There was also no significant difference in overall survival between local and distant recurrence from initial resection, despite distant recurrence occurring earlier than local recurrence [5]. This highlights the fact that in most patients pancreatic cancer is a systemic disease and adequate multimodality therapy with local and systemic therapy is needed to appropriately treat patients.
Although local control is important, there are several factors that influence survival following recurrence including tumor and patient specific factors. This is supported by our data which shows improved survival from recurrence in good performers (KPS > 90), overweight (BMI > 24.9) compared to normal and underweight patients, patients able to receive additional chemotherapy at the time of recurrence, and longer time to recurrence from initial resection. The observation that overweight patients have better survival is likely due to the fact that many of the normal and underweight weight patients had significant weight loss prior to presentation as compared to people that maintained weight with BMI > 24.9. Both BMI and ability to receive chemotherapy are similar markers to performance status.
Importantly, with the ability to dose escalate and adequately cover the target volume with MRgSBRT it seems to confer a local control benefit as compared to non-MRgSBRT, with a 6- and 12-month local control of 92.3% and 83.9%, respectively. The 3 cases of local failure in our population could be explained by pancreatic adenocarcinoma’s inherent radioresistance, but it is also likely that portions of tumor were under dosed in order to protect normal organs.
A strength of the study includes its reporting on novel treatment modalities with MRgSBRT, as well as capturing data in a prospective manner. Limitations of the study include its small population size as well as reporting on patients treated at a single academic center. Additionally, as it captures a wide variety of patients with a range of prior therapies, disease stage, treatment sites and radiation dose, precise interpretation of the results remains difficult.





留言 (0)