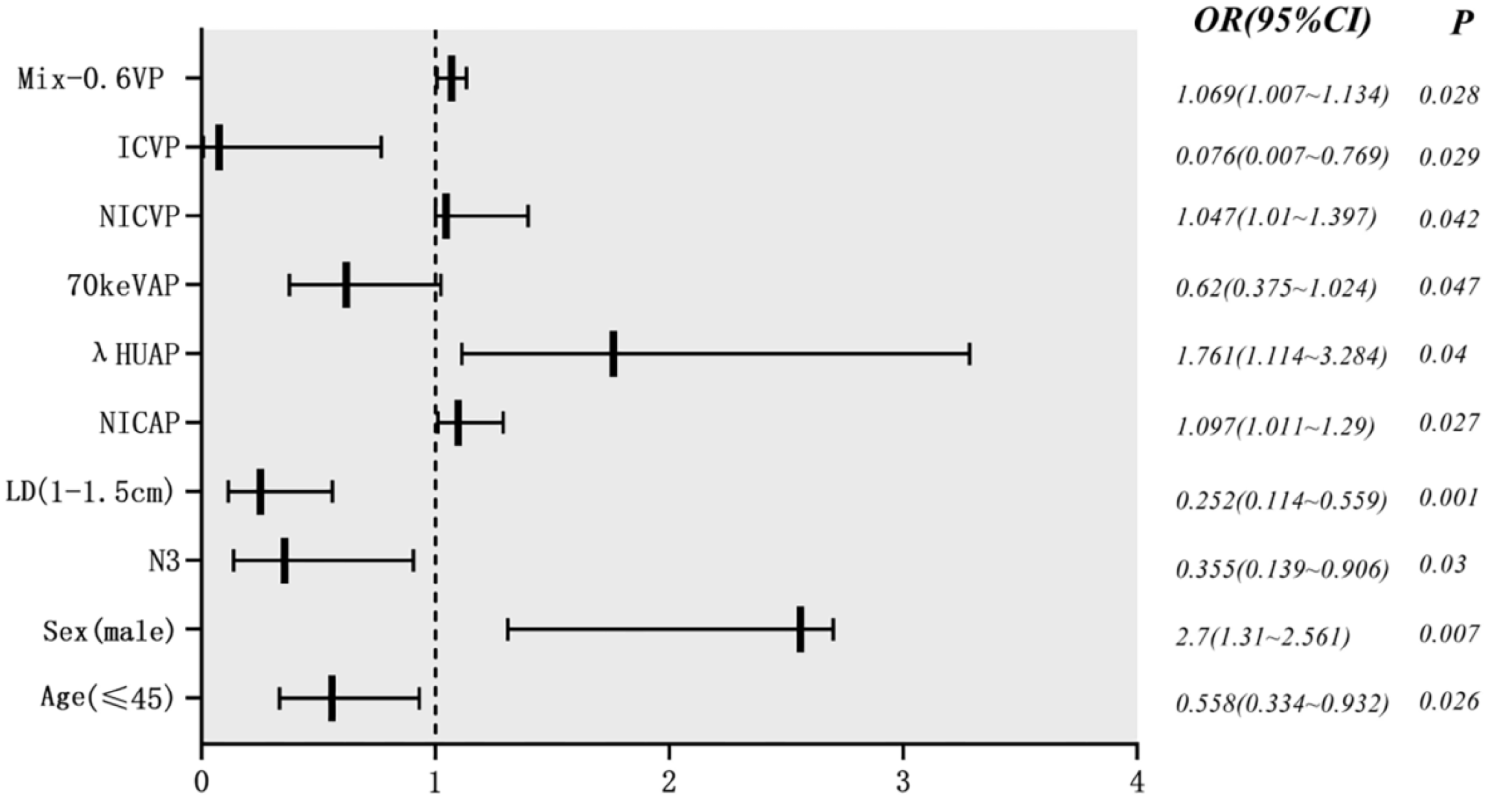
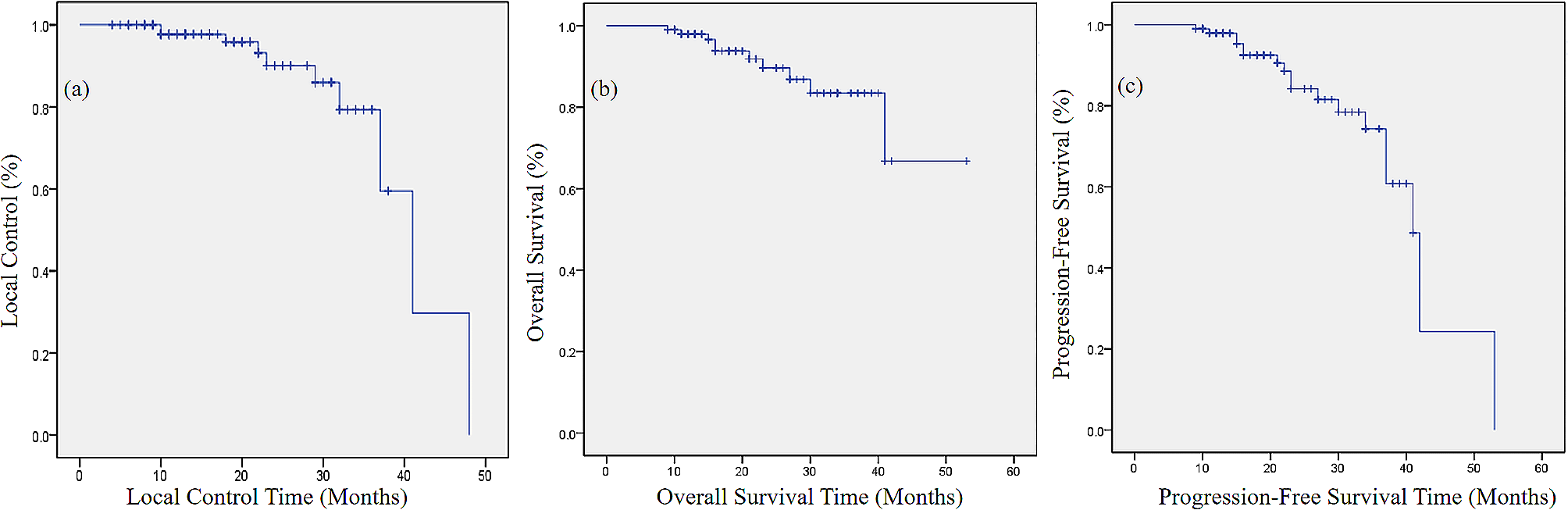
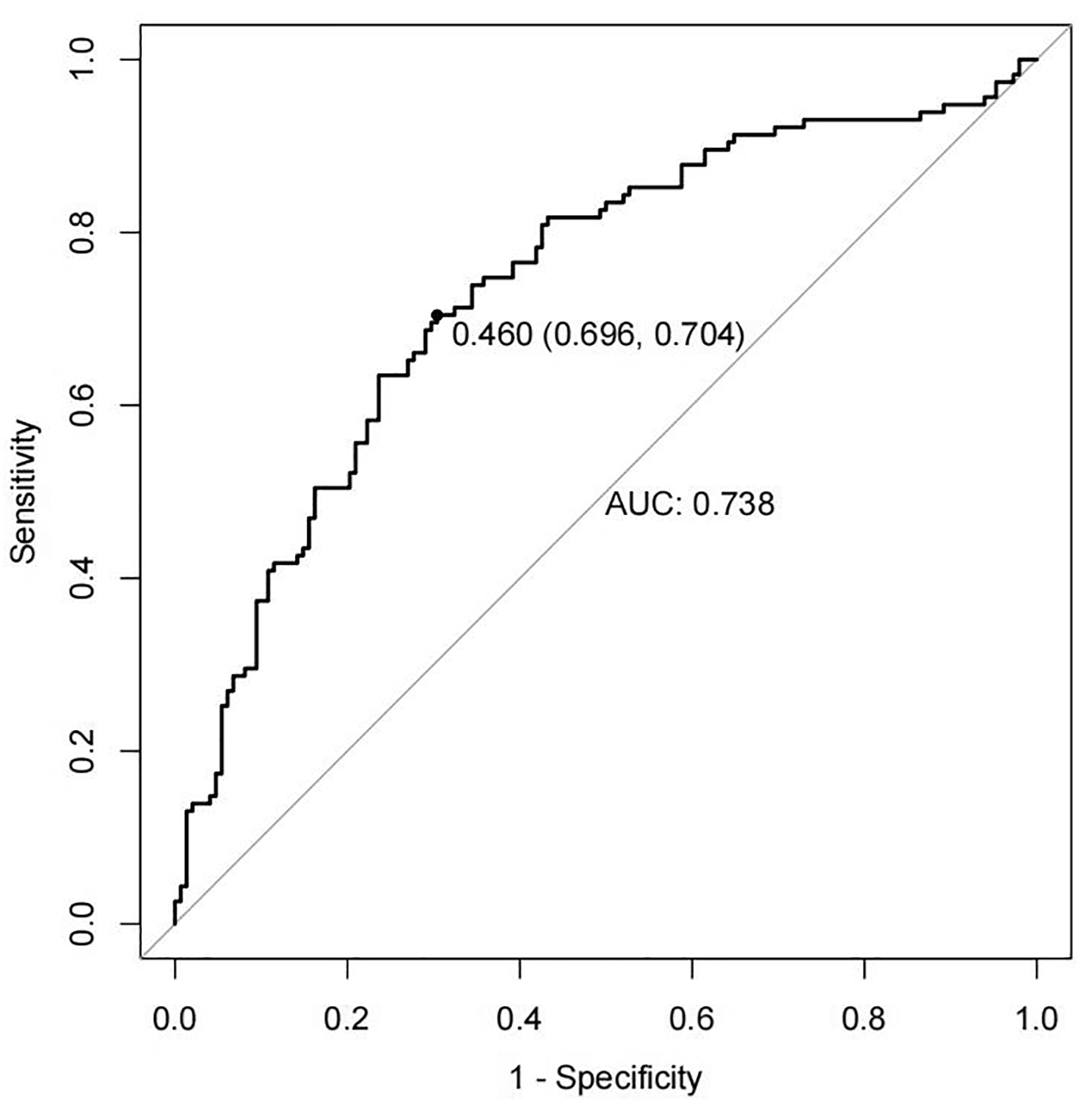
We conducted this retrospective study based on the high incidence (66.7%) of adverse reactions, mainly RP, when using bevacizumab in combination with TRT, as reported in previous small-sample studies [18]. We enrolled a total of 119 patients who underwent TRT during bevacizumab treatment, compensating for the insufficient sample size in previous studies. Our research results shows that the incidence of RP of grade 2 and above is 31.9% and the incidence of grade 3 RP is 9.2%. Fortunately, RP of grade 4 or above did not occur, thus our results did not exceed clinically acceptable limits. Subsequently, V20 > 16.9% and PTV-volume > 183.85 cm3 were identified as independent predictors of RP occurrence. In terms of survival, the combination of bevacizumab and TRT in our study resulted in significant survival benefits (mPFS, 14.27 months; mOS, 37.09 months). In summary, there was no severe RP of grade 4 or above, and the addition of TRT brought significant survival benefits to patients, simultaneous bevacizumab and TRT is feasible.
Previous studies have reported the incidence of RP in various treatment modes combination with TRT [19]. Under the traditional curative radiotherapy and chemotherapy mode, the incidence of RP is 13 -37% [20]. In addition, a systematic literature review and meta-analysis reported that the incidence of grade 3 and above RP ranged from 3.62 to 7.85% [21]. When immunotherapy is combined with TRT, the incidence of RP varies depending on the medication used. The incidence of grade 2 or above RP with programmed cell death ligand-1/ programmed cell death-1 (PD-L1/PD-1) inhibitors is 33.9%/15.1 -21.6%, and the incidence of grade 3 or above RP is 2.6 -3.3%/5.9 -11.7% [22,23,24,25,26,27]. For patients with positive driver genes, the incidence of grade 2 or above RP in patients receiving first generation epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) combined with TRT is 44.78%, and the incidence of grade 3 or above RP is 8.96 -10% [28, 29]. When Osimertinib combined with TRT, the incidence of RP above grade 2 is 63.6% [30]. Based on our research results, which showed a 31.9% incidence rate of grade 2 and above RP, TRT can be safely treated in combination with bevacizumab.
There is no consensus on the mechanism by which bevacizumab use with TRT increases the incidence of RP, but some signal pathway may explain the relationship between bevacizumab and RP. On the one hand, the anti-VEGF receptor effect of bevacizumab can normalize tumour blood vessels, improve the hypoxic environment of tumour tissue and sensitize tumours to radiation. Anti-VEGF antibody inhibits the VEGF signalling pathways required for wound healing following typical tissue damage by radiation, suggesting caution in treating patients with combinations of targeted agents and radiotherapy. In preclinical studies, angiogenesis inhibitors have been shown to enhance radiation-induced cell killing and brief normalization of the tumour vascular system leading to increased oxygenation [31, 32]. Bevacizumab has also been shown to significantly downregulate the gene base and DNA repair involved in proliferation [33]. Whether the mechanism of tumour radiosensitization is also the reason for enhanced radiation-induced lung injury remains to be studied.
Based on the high-risk factors identified in our results, we provide some recommendations to reduce the incidence of RP. One of the high-risk factors for RP is radiation dosimetry, including V20 > 16.9% and PTV-volume > 183.85 cm3 is an independent predictor of RP occurrence. Therefore, it is necessary to strictly select the treatment population, and selecting smaller treatment targets may be a good suggestion for better patient protection. Also strictly limit the physical parameters of radiotherapy, balance the relationship between radiotherapy target area and radiation dose. At last, suspended the use of bevacizumab in a given cycle or increase the interval between bevacizumab and TRT is also a suggestion worth considering. It is worth mentioning that one patient adverse event occurred and the cause of death was massive haemoptysis caused by TEF in our study. Coincidentally, in a clinical study targeting NSCLC, 2 out of 5 patients developed TEF during TRT and bevacizumab maintenance treatment [34]. Two patients also had severe oesophageal toxicity after CRT and bevacizumab treatment. The implication is that the severe oesophageal toxicity caused by this treatment may make patients more susceptible to TEF. This adverse event is worth our vigilance.
In terms of survival, the combination of bevacizumab and TRT significantly prolonged the survival of patients in our study (mPFS, 14.27 months; mOS, 37.09 months) compared with the BEYOND study [2] (mPFS, 9.2 months; mOS, 24.3 months) and ECOG4599 [1] study (mPFS, 6.4 months; mOS, 12.3 months) reported the survival outcomes of first-line chemotherapy combined with bevacizumab (without TRT). The reason for this phenomenon may lie in the potential screening of the treatment population. Firstly, multiple previous studies have confirmed the significant effect of TRT on prolonging patient survival as mentioned in the background, and this is no exception in our study. Secondly, in our study, the majority of patients (89.1%) included TRT as consolidation therapy, which means these patients have a relatively good response to first-line treatment. In addition, the patients selected in our study were those who received first-line treatment, and patients who used bevacizumab after progression were excluded. This means that these patients have limited lesions and are relatively more likely to have a better prognosis. In summary, considering both the significant survival benefits obtained by patients and the acceptable incidence of RP, simultaneous bevacizumab and thoracic radiotherapy can be allowed. But it is necessary to require clinical doctors to do a good job of patient treatment follow-up and promote education on possible discomfort symptoms.
Several limitations should be acknowledged. Firstly, this was a retrospective study in a single institution, inevitably resulting in selection bias. Secondly, although we expanded the sample size as much as possible, an insufficient sample size is still a drawback. The reason for the small sample size may be that the previously reported high incidence of adverse reactions led clinical doctors to be more cautious when using bevacizumab and TRT. Effective intervention measures for RP are a direction of interest in subsequent research. The treatment for RP is only routine anti-inflammatory and hormone therapy, but some patients are still not treated. Therefore, there is an urgent need for an effective preventive drug to curb the occurrence of RP. A paper reported the protective effect of Erb-(IL-10)2, a bispecific protein synthesized by cetuximab and IL-10, on radiation-induced skin damage and mucosal repair, which may be helpful for the intervention of RP even oesophagitis radiation injury [35].







留言 (0)