Based on our literature search analysis, iterative discussions, and analyses of UME curricular content taught at our institutions, we discovered two principal themes across the basic sciences and clerkships related to DEI: (1) topics and terminology/language that can be readily fixed, adjusted, or replaced to enhance inclusion and (2) topics that are more complex which require more thoughtful discussion with students. For example, some topics may require a discussion on the pros and cons of including race, sex, gender, or sexual orientation as part of medication management or guidelines. These discussions could be paired with didactic sessions on the guideline’s origins (i.e., the history of race in medicine). However, in some instances, topics may need to be addressed by an expert or be considered as part of a case discussion to allow time for deeper engagement (which is often limited in foundational science presentations). Regardless, there are multiple avenues via which DEI topics can be incorporated across medical curricula.
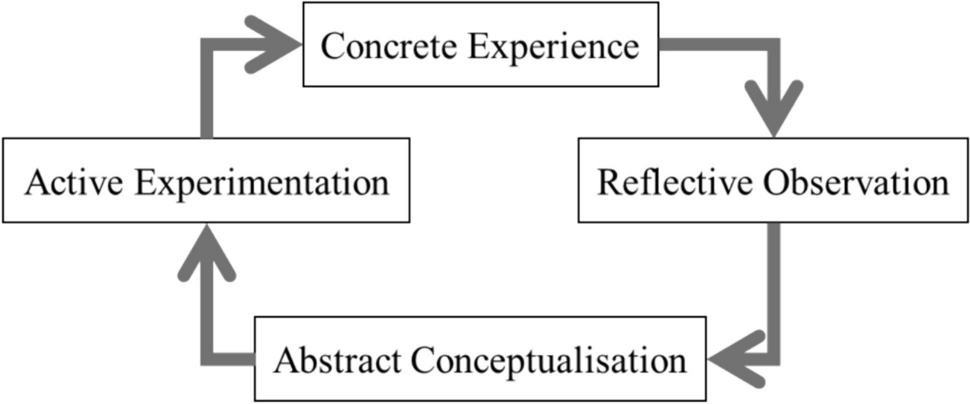
To conduct a systematic analysis of topics for embedding DEI in curricula, we formulated a framework which is divided into three different domains (Fig. 2). The first domain is focused on insensitive and inaccurate wording and concepts. The second domain concerns the inappropriate substitution of cultural constructs for genetic differences. Lastly, the third domain entails keeping curricula current through constant vigilance and review. The three domains operate in a cyclical manner linked by the “gray area of learner and educator comfort and understanding” which represents a region of interaction where significant benefit can be derived by discussing topics that are more complex and nuanced, not lending themselves to a single “right or wrong” answer. The goal of this framework is to foster open discussion to imbue educators and learners with the principle that this is a continuous cycle of analysis and improvement, not just a single pass of material.
Framework for Systematic Analysis of DEI Issues in Undergraduate Medical Education Basic Science ContentDomain I. Insensitive and Inaccurate Wording or Concepts
Careful re-examination of teaching materials and content can ensure that the language used is not insensitive or inaccurate and that wording or concepts are free of bias. Removing or modifying harmful language or concepts may be under the control of the educator whereas in other cases we rely on outside societies or organizations to address these changes. Provided below are five clinically relevant DEI examples on the use of insensitive and inaccurate wording or concepts.
Example 1. Out-of-Date Guidelines That Still Include Race as a Variable
There are still a number of clinical guidelines used both in practice and teaching that continue to incorporate race as a variable (e.g., Joint National Committee (JNC) on Hypertension 8 guidelines) without compelling data to support its inclusion [16, 17]. The JNC 8 guidelines have not yet been updated to remove race as a factor, nor have the more recently developed 2017 American College of Cardiology/American Heart Association (ACC/AHA) guidelines, which also contain race as a variable [18]. However, these guidelines provide a remarkable opportunity to discuss study design, race, and treatment response.
Example 2. Potential for Harm by Removing Race as a Variable from Clinical Calculators
In contrast to JNC 8 or 2017 ACC/AHA guidelines, certain guidelines that have removed race may actually be harmful to certain vulnerable patient populations. For example, the MDRD (Modification of Diet in Renal Disease) formula for calculating glomerular filtration rate (GFR) was updated to remove race because race is not a biological construct, it does not adequately capture multi-racial diversity, and the original studies lacked sufficient evidence to support the inclusion of race [19]. However, removing race from the GFR formula may have a negative impact for self-identified Black/African American patients with both chronic kidney disease (CKD) and type 2 diabetes as eligibility and dosage of diabetes medication for these patients are determined by GFR [20]. This discordance can lead to confusion and frustration on the part of learners in the absence of sufficient explanation prior to their presentation and discussion. To help address this confusion, having a case conference or integrated session that includes professionals in primary care, specialists in kidney disease, and diversity experts can give learners a broad view of the issue both as it relates to medicine and DEI.
Example 3. Inaccuracies in Outdated Learning Materials
Older textbooks, primary literature, and secondary literature may contain language or references that may also contain insensitive language or biased references. For example, some older literature on acquired immunodeficiency syndrome (AIDS) still inappropriately incorporates the idea of a homosexual Canadian flight attendant named Gaeten Dugas as “patient zero” [21]. Educators using dated texts and literature with references to “patient zero” should strongly consider including a brief historical summary together with the lessons learned. This change would bolster the integration of both the epidemiology behind AIDS research as well as the sociocultural aspects that are often ignored or awkwardly tacked on to content.
Similarly, textbooks and literature provided to learners should be carefully reviewed for insensitive or inappropriate material. In 2017, the academic textbook publisher Pearson issued a recall and public apology for racially biased descriptions of “cultural differences in pain perception” found in a nursing text book (Nursing: A Concept-Based Approach to Learning, Volume I, Edition 2, 2014) [22].
Example 4. Updating Insensitive Language and Terms
For many years, the terms “red man syndrome” or “red neck syndrome” have been used to describe the adverse effect of the antibiotic vancomycin encountered in some patients upon infusion [23,24,25]. This term has the potential to marginalize certain groups of people. The potential for harm from using this term far outweighs the small effort it takes to proactively change or remove it from curricular materials.
Example 5. Addressing Stereotype and Bias During the Learning Process
Clinical vignettes may potentially reinforce stereotypes, introduce bias, and trigger stereotype threat, thereby hindering an examinee’s ability to perform well [26, 27]. Content that can be perceived as promoting stereotypes, bias, shame, or stigma spans many factors such as race, ethnicity, sex, gender, weight, religion, poverty, and disability, among others. Including these dimensions in vignettes can create negative stereotypes, even though exposing learners to the diversity of patients they will encounter in clinical practice is important. Examples include referring to a patient as homeless, rather than “a person experiencing homelessness” or referring to a patient as a “drug addict” rather than “a patient suffering from substance use disorder.” This issue requires careful use of language, prudence, and humility on the part of both educators and learners. However, this does not mean that all identifiers should be removed from vignettes. Rather, the key is to expose learners to a variety of patients without reinforcing stereotypes.
Domain II. Inappropriate Substitution of Cultural Constructs for Genetic Differences
There are many notable examples of using genetics to guide diagnosis, management, prognosis, and prevention in medical care. These include inherited diseases (e.g., cystic fibrosis or Huntington’s disease), drug therapy (e.g., certain anti-coagulants and anti-viral agents), disease progression (e.g., a range of cancer subtypes), and screening (e.g., breast cancer risk, congenital). While these examples rely on genetic differences between patients that may appear to align with race, ethnicity, or cultural ancestry, these associations are tenuous at best. As a consequence, there is a history of using race as a surrogate or proxy for genetics that can have harmful effects on patients and their care [28, 29]. There are now widespread efforts to review and revise the use of cultural constructs in medicine particularly in the context of genetic predisposition to disease or response to therapy.
Yet, in some instances where a clear understanding of genetic linkage is absent, race is still incorporated in screening, diagnosis, and management (e.g., prostate cancer, triple-negative breast cancer). These gray areas are the most difficult for educators and learners to navigate, though they furnish us with opportunities for deeper consideration of social constructs, genetics, and medicine. Examples of such gray areas can be found throughout the continuum of medical care.
Listed below are three examples that serve as prime opportunities to discuss the intersection of race, ethnicity, and genetics, and how this can directly impact a patient’s medical management outcome.
Example 1. Use of Ancestry in Cancer Screening
Prostate cancer screening is an example where it is recognized that self-identified Black/African American patients have a higher risk for developing prostate cancer compared to people of other races [30]. Thus, the American Urological Association (AUA) and the Society of Urologic Oncology (SUO) joint guidelines on PSA screening still include Black ancestry as a parameter and recommends screening at an earlier age than other populations. The current AUA/SUO guidelines state that:
“Clinicians should offer prostate cancer screening beginning at age 40 to 45 years for people at increased risk of developing prostate cancer based on the following factors: Black ancestry, germline mutations, strong family history of prostate cancer. (Strong Recommendation; Evidence Level: Grade B)” [31].
At some point in time, there may be a biological or genetic marker that helps explain this increased incidence. However, at the current time, Black ancestry is still part of the guidelines. If learners were simply provided such guidelines without explanation or discussion (i.e., inclusion of race may benefit some patients in certain situations), then this can lead to stress and discomfort and a perception that no effort was taken to address potential bias. Yet, the guidelines and position statement by the AUA/SUO is actually instructive for teaching and learning efforts. The AUA guidelines have been updated to include a position statement and acknowledge the risks of including race: “Although emerging data exist, a far more comprehensive understanding is required of the impact of race and ethnicity on the operating characteristics of PSA, secondary biomarkers, and prostate imaging. It is also essential to recognize many people undergoing screening are of mixed (or unknown) race and ethnicity. Since dramatic disparities exist regarding access and affordability of certain diagnostic or imaging modalities, efforts should be made by clinicians, payors, and health care systems to bridge this gap.” This statement, in and of itself, provides a learning opportunity regarding recognition and acknowledgment of DEI in medical practice.
Example 2. Focusing on Disease Prevalence in Racial Groups Can Lead to Harmful Generalizations
Triple-negative breast cancer (TNBC) more commonly occurs in self-identified Black/African American women compared to people of other races and genders (i.e., TNBC in males, while rare, can occur) [32]. This widely reported observation, while accurate, can lead to the harmful assumption that TNBC only affects self-identified Black/African American women or is strictly associated with race and gender. Taking into consideration that both genetic (biological) and non-genetic (lifestyle) factors appear to play a role in pathogenesis makes TNBC an ideal vehicle to discuss the intersection of cultural constructs and genetics [33, 34].
Example 3. Genetics and Adverse Drug Reactions
The adverse drug reaction known as Stevens-Johnson syndrome (SJS) is associated with some types of medications (e.g., agents for management of gout, anti-convulsant drugs) in patients with mutations in certain human leukocyte antigen (HLA) genes [35]. Some HLA polymorphism–associated adverse drug reactions are disproportionately represented in patients who have self-identified as certain ethnicities, such as Black, Asian, and Indian [36, 37]. However, while SJS develops more commonly in these ethnic groups after treatment with certain medications, it does not only occur in these ethnicities. In the absence of a better understanding of the role that complex population genetics play in this adverse drug reaction, teachers, learners, and practicing physicians are left with an incomplete understanding that exposes patients to both potential bias and serious medical complications. Articulating that prevalence is not a blanket permission to overlay race, ethnicity, and genetics is important for learners to hear, given that mixed ancestry as well as unknowns about biology can render the relationship between race and genetics invalid.
Domain III. Keeping Current Through Constant Vigilance and Review
Our understanding of the intersection of medicine, genetics, race, ethnicity, sexual orientation, and gender is constantly evolving. As this relationship develops and new knowledge is generated, educators and learners must stay up to date on changes. Additionally, as our understanding changes, so too does the language we use, which has the potential to promote or propagate bias. Thus, it is imperative that educators and learners stay current and up to date on changes in the field of DEI. Likewise, educators and learners need to consider the ever changing political, religious, and cultural influences that can shape medical education and presentation of certain topics (e.g., abortion, transgender care). These influences often vary by region, state, or even among local hospital systems. Provided below are two examples where constant vigilance and review are warranted.
Example 1. Continual Learning of Transgender Health
Current medical care and terminology relating to transgender patients provides a cautionary tale for those who believe that complacency in addressing DEI issues in the classroom is acceptable. While transgender patients have always been a part of our society and medical practice, more visibility has been garnered through advocacy. As a result, society and health science professions grapple with both biological issues and their role in management, diagnosis, and patient counseling. Terminology and proper use of pronouns is evolving. A growing body of research continues to highlight health inequities experienced by transgender individuals, and further underscores the need for medical providers to be appropriately trained to deliver care to this population [38, 39]. A number of tools have been developed and reported in the literature to address gender and transgender health inequities in education and clinical care [40, 41]. These resources can be utilized to improve attitudes and awareness toward transgender populations, provide knowledge of unique clinical concerns, and help develop skills to deliver competent care [40].
Research suggests that incorporating transgender clinical competencies across the curriculum (rather than in one or two condensed lectures) helps reinforce topics in their relevant clinical context with emphasis over time [39, 42]. Because of rapid changes in our society, cases and material should be reviewed regularly and updated. For example, the aforementioned AUA/SUO PSA prostate cancer screening guidelines also acknowledge gender as a potential source of bias: “For non-binary patients or transgender women there is a lack of data on prostate cancer screening preferences, if and when to initiate, the accuracy of biomarkers (e.g., PSA, secondary biomarkers, MRI), potential psychological consequences, impact of gender-affirming hormonal therapy, and priorities regarding management options. Considerably more effort and research are required.” [31]. This facet of patient care may escape some learners and educators who are only thinking about male patients in regard to prostate cancer. This could lead to a lack of consideration for a pathological issue that could affect male patients who have transitioned to female. This highlights the importance of carefully reviewing resources for changes so that teaching material can be updated appropriately.
Example 2. Impact of Gender Bias
Gender bias represents another area of clinical medicine which has unique challenges [43]. For example, gender bias has permeated published textbooks used in medical education [44]. While strides have been made to address bias within some areas of gender, the coverage of topics specifically highlighting transgender populations is often inadequate or altogether missing in medical and health science curricula. The lack of knowledge surrounding transgender health has manifested in reports of transgender people being denied health care or experiencing discrimination, including verbal and physical abuse, even in health care settings [45, 46].









留言 (0)