
記住我



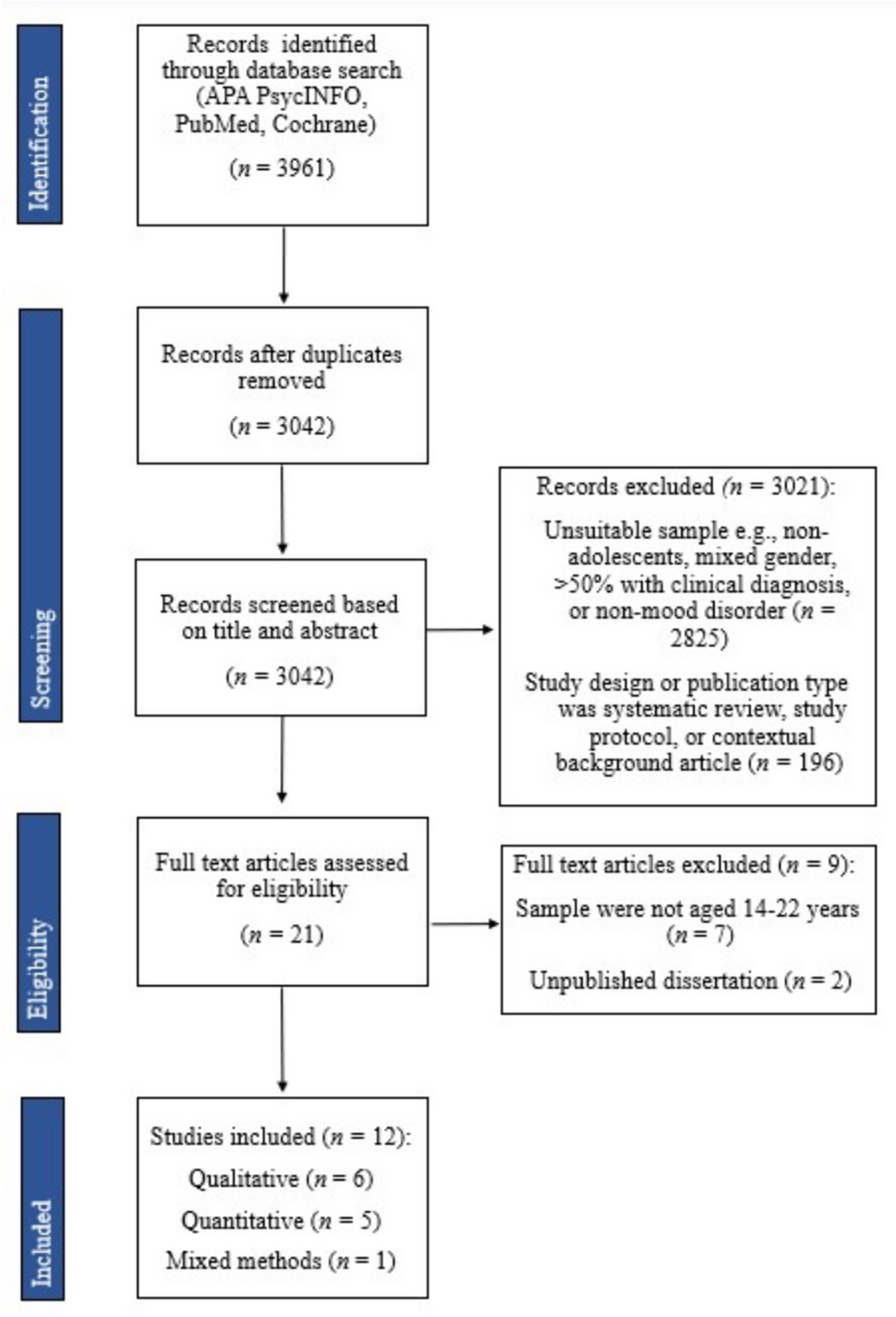
We identified 78 eligible studies (total N = 1389; age range 3–25 years, M = 16.43, SD = 4.51; 61.4% male; see Fig. 1), composed of four double-blind, sham-controlled RCTs [35,36,37,38], one double-blind, sham-controlled, crossover RCT [39], four single-blind sham-controlled RCTs [40,41,42,43], one single-blind, comparator-controlled RCT [44]; one sham-controlled RCT [45], two waitlist-controlled trials [46, 47], one non-randomised, wait-list controlled trial ( [48]; see Table 1), one multi-arm open-label study [49], one two-arm open-label study [50], 27 single-arm open-label studies, and 35 case series/studies (see Supplementary Material S2 and S3). Of these studies involving CYP, 28 studies were in participants with depression, 20 were in ASD, seven in schizophrenia, five in obsessive-compulsive disorder (OCD), four in Tourette’s syndrome, four in attention-deficit/hyperactivity disorder (ADHD), two in anorexia nervosa (AN), borderline personality disorder (BPD), and catatonia, and one in binge eating disorder (BED) and internet gaming disorder (IGD). Across studies, rTMS was typically delivered over ~ 20 sessions (M = 19.7; SD = 8.51; range 5–50) with a stimulation intensity of 80–120% of the resting motor threshold (RMT). The most common protocols employed across studies was 10 Hz, HF-rTMS and/or 1 Hz, LF-rTMS to the left- and/or right dorsolateral prefrontal cortex (DLPFC) (n = 44; 56.4%).
Fig. 1
PRISMA flow diagram of selected studies (n = number of articles). A total of 78 studies were systematically reviewed
Table 1 Summary of controlled trials using repetitive transcranial magnetic stimulation in children, adolescents, and young people with psychiatric disordersQuality assessmentOf the thirteen RCTs, overall risk-of-bias was rated as “high” in two studies [45, 47]; nine with “some concerns” [35,36,37, 40,41,42,43,44, 46], and three with “low” [35, 38, 39] (see Supplementary Material S1). The non-randomised, controlled clinical trial was rated with moderate risk of bias [48]. All open-label studies, case series, and case reports were rated as low quality. One RCT was retrospectively registered [37] and four were prospectively registered [35, 38, 40, 42] (and comparison of the registered protocol with final publication showed that one study omitted two registered primary outcomes ( [42]; autism spectrum quotient and social communication questionnaire). One RCT [36] reported an incorrect clinical trial registry identifier and we were unable to find the study record using other trial information (e.g., investigator name) in the search function.
What are the clinical effects of rTMS in children and young people with psychiatric disorders?Neurodevelopmental disordersAutism spectrum disorder (ASD)There have been six controlled trials conducted in ASD. In an integrated 4-week RCT and 4-week open-label extension study [42], iTBS was delivered to the bilateral posterior superior temporal sulcus in 78 CYP with ASD. During the first four weeks, the study group received two sessions of iTBS per week (8-sessions total) and the control group received sham TBS. After unblinding, both groups received eight sessions of real iTBS over the next four weeks. Results showed there were no significant group-by-time interactions for the study vs. control group on clinical symptoms in the first four or eight weeks. However, within-group analysis showed significant improvements in parent-rated social skills and repetitive behaviours at week eight compared to baseline for the 8-week iTBS group [42].
One double-blind RCT [36] applied 10 sessions of HF-rTMS to the right inferior frontal gyrus combined with action observation and execution (AOE) training or sham rTMS with AOE to 10 CYP with ASD. Within-group analyses showed a significant increase in clinician-rated receptive and expressive communication, as well as domestic and community daily living, from baseline to 1-week follow-up in the group that received HF-rTMS + AOE. In addition, clinician-rated communication significantly increased in the sham rTMS + AOE and the HF-rTMS + AOE groups from baseline to 1-week follow-up [36].
A randomised, sham-controlled trial [45] in 32 children with ASD and intellectual disability, reported significant reductions in parent-rated social relating behaviours, and overall non-adaptive behaviours, immediately after 18-sessions of LF-rTMS to the left- and right-DLPFC, compared to baseline. Although no significant changes were reported in the sham-group, no between-group analysis was conducted. One randomised waitlist-controlled study [47] in 45 adolescents with ASD reported significant between-group differences in parent-rated repetitive and restricted behaviour patterns and irritability immediately after 12-sessions of LF-rTMS, but no difference in social awareness and hyperactivity. These authors [47] did not report outcomes for any other subscales.
A non-randomised waitlist-controlled study [48] in 42 children with ASD reported a significant group-by-time interaction in parent-rated total repetitive and restrictive behaviours, lethargy, and hyperactivity, but no change in irritability, stereotypy, inappropriate speech, self-injurious behaviour or restricted interests, due to a significant decrease from baseline after 18-sessions of LF-rTMS to the right-DLPFC combined with neurofeedback, with no change in the waitlist group. Another waitlist-controlled study (no randomisation details provided; [46]) in 54 adolescents with ASD, reported significant improvements in parent-rated stereotypic behaviour, ritualistic behaviour, irritability, lethargy, compulsivity, and hyperactivity, but no change in inappropriate speech, self-injurious behaviour, and restricted interests, after 18-sessions of LF-rTMS to the right-DLPFC: no changes were seen in the waiting-list group, compared to baseline.
This research group also conducted one multi-arm open-label study [49] and six single-arm open-label studies [51,52,53,54,55,56]. These studies evaluated several outcomes (e.g., Visual oddball task, Aberrant Behaviour Checklist, Repetitive Behaviour Scale-Revised), with some reporting improvement and other outcomes showing no change (see Table 2). The authors provided no evidence to show these studies were statistically powered to detect change and they did not correct for multiple comparisons.
Seven additional open-label studies or case studies were conducted in ASD. Two open-label studies applied HF-rTMS to the inferior parietal lobule (IPL) [57, 58]. One study reported significant improvements in parent-rated speech/language and sociability from baseline to 6-weeks after 30-sessions of HF-rTMS, but not from baseline to post-stimulation, in 11 children with low-functioning ASD [58]. The other study, in four children with ASD, reported no significant changes in clinician-rated ASD symptoms, or parent-rated sociability and communication, immediately after 9-sessions of rTMS compared to baseline [57].
One open-label study [59] applied 19 sessions of individual alpha frequency (IAF)-guided rTMS to 28 children with ASD. IAF-guided rTMS was determined by identifying the dominant peak frequency with the highest power in the 8–13 Hz range and multiplying it by the higher harmonic frequency (5th to 10th ) of the electroencephalogram nearest to the dominant peak frequency. The stimulation site was determined by identifying the brain region with the highest aberrant cortical processes compared to a normative database with equal parameters and measured using the 10–20 system. Within-group analyses showed significant improvement in clinician-rated emotional response, object use, fear or nervousness, intellectual response, and general impressions of autism from baseline to post-treatment [59].
Another open-label study [60], applied 15-sessions of iTBS to the right-DLPFC in 10 adolescents with ASD and reported significant reductions in parent-rated restricted and repetitive behaviour, and obsessive-compulsive symptoms, from baseline to immediately post-stimulation.
A case study [61] in a 15-year-old male with ASD and comorbid depression described improvements in mood and core features of ASD following 20 sessions of LF-rTMS to the right-DLPFC and 10-sessions of LF-rTMS to the left-DLPFC. Two case studies applied deep-TMS ?? to the medial-PFC: in one study [62] a 20-year-old woman with high-functioning ASD, self-reported improvements in social functioning following 9-sessions of deep-TMS, and the other study [63] reported improvements in clinician-rated obsessive-compulsive symptoms, but not self-reported autistic traits, in a 25-year-old female with ASD and comorbid OCD immediately after 27 sessions of deep-TMS.
Attention deficit hyperactivity disorder (ADHD)Three controlled trials applied HF-rTMS to the right-DLPFC in CYP with ADHD. In a double-blind, sham-controlled RCT [37] in 60 CYP with ADHD, atomoxetine combined with 15 sessions of active HF-rTMS significantly improved parent-rated total ADHD symptoms and teacher-rated inattention at post-treatment and 1-month follow-up compared to sham, as well as parent-rated hyperactive-impulsivity at post-treatment, but not at 1-month follow-up [37]. In a multi-arm, active-comparator RCT [44], 60 children with newly diagnosed ADHD were randomly assigned to receive (a) 30 sessions of HF-rTMS over 6 weeks, (b) atomoxetine once-daily over 6 weeks, (c) HF-rTMS and atomoxetine over 6 weeks. All three groups showed significant improvements in parent-rated severity of core ADHD symptoms at post-stimulation compared to baseline, but the group that received HF-rTMS and atomoxetine showed significantly greater change scores for attention deficit, hyperactivity and impulsivity, but not oppositional defiance, compared to the groups that received HF-rTMS or atomoxetine alone [44]. A sham-controlled, crossover RCT [39] in nine adolescents with ADHD reported no significant differences in core ADHD symptoms or clinical global impression between 10-sessions of real or sham HF-rTMS to the right-DLPFC.
An open-label study [63] applied 5-sessions of LF-rTMS over the left-DLPFC in 13 boys with ADHD and reported a significant improvement in parent- and teacher-rated behaviour at home and at school from baseline to 1-week post-stimulation.
Tourette’s syndromeFour studies applied LF-rTMS or cTBS to the supplementary motor area (SMA) in CYP with Tourette’s syndrome. A randomised, sham-controlled trial [38] delivered 8-sessions of cTBS in 4 trains per day over 2 consecutive days in 12 adolescents with chronic tics. No significant differences in clinician-rated severity of tic symptoms and obsessive-compulsive symptom severity, self-reported severity of tic-related premonitory urges and health-related quality of life, or parent-rated ADHD symptom severity were found between the real and sham cTBS group at 7-days follow-up [38]. An open-label study [64] in 10 children with Tourette’s syndrome reported a significant reduction in clinician-rated tic severity and impact of tics on quality of life after 10-sessions of LF-rTMS, and at 12-week follow-up, compared to baseline. Another open-label study [65] applied 15-sessions of bilateral LF-rTMS to nine CYP with Tourette’s syndrome and reported that tic severity significantly decreased from baseline to post-treatment. Lastly, a case study [66] applied 10-sessions of LF-rTMS in two CYP with Tourette’s syndrome and reported improvement in clinician-rated tic severity from baseline to post-stimulation which was maintained for 1-month in one case and 4-months in the other case. After 1-month, the first case had recurring tic symptoms and 10 additional sessions of LF-rTMS were delivered with similar improvement in clinician-rated tic severity reported [66].
Schizophrenia-Spectrum disordersSchizophreniaFour studies applied LF-rTMS to the left temporoparietal cortex (TPP) in CYP with schizophrenia. One open-label study [67] in 10 adolescents with schizophrenia reported a significant improvement in auditory hallucinations and psychosocial functioning immediately after, and 1-month after, 10-sessions of twice-daily LF-rTMS compared to baseline. In a case study in an 11-year-old boy with schizophrenia [68], 10-sessions of LF-rTMS to the right-temporoparietal junction (TPJ) was not associated with improvements in auditory hallucinations compared to baseline, but after 10-sessions of LF-rTMS to the left-TPJ, auditory hallucinations reduced, and this improvement was maintained at 6-week follow-up [68].
In another case study [69], an 18-year-old female with schizophrenia received 3 separate courses of 10- and 15-sessions LF-rTMS to the left-TPP due to improved self-reported reduced auditory hallucinations following rTMS and subsequent recurrence of symptoms at 5-months after the first course of rTMS and 3-months after the second course of rTMS. After the third course of rTMS, the patient self-reported maintained improvement in auditory hallucinations at 4-months [69]. Similarly, another case study [70] applied two separate courses of 10-sessions of LF-rTMS over the left-TPP in an 18-year-old woman with schizophrenia who self-reported minimal change in audito
留言 (0)