
記住我



Reduced bone density is a risk factor for unsatisfactory clinical outcomes after orthopedic surgery of the lower extremities. This is related to the influence of bone density and stable fracture fixation.1,2 Furthermore, fragility fractures may occur in severe osteoporosis.3–6 Even after ankle arthrodesis, a reduction in bone density in the calcaneus could persist for many years after fusion.7,8 Studies on ankle and calcaneal fractures have shown that reduced bone density alters clinical outcomes after fracture fixation.9,10
Quantitative computed tomography, dual-energy Radiograph absorptiometry (DEXA), and CT scanning with calculation of Hounsfield units (HU) have been established as methods for measuring bone mass density (BMD).10–12 Alternative non-ionizing methods, such as (semi)-quantitative ultrasonography densitometry (QUS), have also been used to evaluate bone density. In addition to the absence of radiation exposure, it is more cost-effective and requires less space than either quantitative computed tomography or DEXA.13,14
The aim of this study was to assess whether bone mineral density in the calcaneus is reduced after open reduction and internal fixation (ORIF) of the lateral malleolus at mid-to long-term follow-up and whether there are side differences between the treated and non-injured sides. The correlation between bone density and outcome was also evaluated.
MethodsAll adults treated for isolated closed Weber-B-type ankle fractures without any further surgery for degenerative, posttraumatic, and rheumatoid changes in our trauma department were included. The minimum follow-up period was 24 months.
Patients less than 18 years of age with open fractures, additional fractures of the lower extremity, dementia, language barriers, decreased activity due to reasons other than the foot, multiple injuries, and revision surgery or amputation at the time of recruitment were excluded. Patients who had received treatment for osteoporosis before injury were also excluded. The bone density of both calcaneus was measured semi-quantitatively with ultrasonography densitometry using the Pegasus smart according to the manufacturer's instructions (Medilink). We conducted bone density measurements no earlier than 24 months and no later than 10 years after the fracture and surgery (follow-up in years 6.2 ± 3 [range, 2 to 12]). There was no standardization for these later time periods.
Pegasus was automatically calibrated in a phantom before use. This calibration enables compensation for any drift from the electrodes or probes, thus producing stable measurements, even after many years of use.
The calcaneal width, broadband ultrasound attenuation (BUA), speed of sound (SOS), stiffness index (SI), T-score, and Z-score were calculated from the ultrasonography signal transmitted through the calcaneus. The range and accuracy of the BUA were 30 to 120 dB/MHz ± 2% reproducibility. The range and accuracy of the SOS were 1,000 to 2,000 m/s ± 2% reproducibility.
BUA levels were correlated with bone density. The measurement of attenuation corresponds to the measurement of the reduction in the ultrasonography signal power through the bone. BUA corresponds to the slope of the attenuation related to the frequency. This measurement was performed over the frequency range of 0.2 to 0.6 MHz. The SOS increased in the rigid materials but decreased in the heavy materials. In the bone, the SOS value is higher than that in soft tissues and is correlated with bone density and strength. A reliable correlation between BUA and bone density has been demonstrated in adults and children.14–16
The SI, an index established by Lunar combines both BUA and SOS and was defined as SI = 0.67 × BUA + 0.28 × SOS − 420.13 The SI was also expressed as Z-score and T-score based on a US reference database using the following equations: Z-score = (SI − age-matched mean SI)/16.6, where age-matched mean SI = 68 + 31.6/[1 + (age/55.9)] × 10.1, and for T-score= (SI −100/16).
The T-score and Z-score were based on a large European and United States reference database for BMD.17 The patients were categorized as “osteoporotic” (T-score of −2.5 or below), “osteopenia” (T-score between −1.0 and 2.5) and “normal bone density” (T-score of −1.0 and above) according to the conventional World Health Organization definition.18 The width of the calcaneus was measured in millimeter.
All fractures were treated with internal fixation of the fibula using the posterolateral approach. All patients, with or without syndesmosis injury, are subjected to partial weight bearing with 15 kg on the injured extremity. Syndesmotic screw was inserted to stabilize the syndesmosis if it was found to be unstable after fixation of the distal fibula. An unstable distal fibula was fixed by using a screw perpendicular to the syndesmosis to approximate the ends of the syndesmosis for sufficient healing without elongation. The syndesmotic screw was removed after 6 to 8 weeks. After removal of the transfixating screw, a pain-free increase in weight-bearing and strengthening was initiated. Patients without a transfixating screw initiate full weight-bearing after 6 to 8 weeks based on radiological evidence of healing.
The postoperative realignment of the fracture was assessed based on Radiograph image. The evaluation using the scoring system proposed by Phillips et al19 requires the availability of X-rays of the uninjured ankle. However, these were not available for our study.19 Postoperatively and during the follow-up examinations, we only conducted X-rays of the injured side. To obtain a quantitative assessment of the quality of the postoperative realignment, we adapted the scoring system proposed by Phillips et al.19 The item “Fibular length compared with the opposite side” is originally weighted only with one point. By eliminating this item, we derived a modified Phillips score of maximum 34. We assumed the talocrural angle to be 84°. The remaining items of the score do not require the opposite side for calculation. Naturally, only properly realigned fractures of the upper ankle joint were included and tested by the modified score.
The American Orthopedic Foot and Ankle Society (AOFAS), Foot Function Index (FFI), Olerud-Molander-Ankle-Score (OMAS), and Hannover-Score (HS) scoring systems were used. Limitations in health-related quality of life were scored by the Short Form Health Survey (SF)-36 v2.0. The treated side was compared with the contralateral uninjured foot.
We used the Kellgren-Lawrence Score (KLS) on lateral and mortise view radiographs of the weight bearing foot to evaluate osteoarthrosis of the ankle joint.20 KLS higher than “1” was defined as significant osteoarthrosis.
All data were analyzed using SPSS 26. Statistical significance was set at P < 0.05. The relationship between the T-score and each clinical outcome was explored using Pearson's correlation coefficient, followed by a linear regression model that was controlled for age and smoking status, as both are potential confounders because of their known associations with both outcomes and bone density.
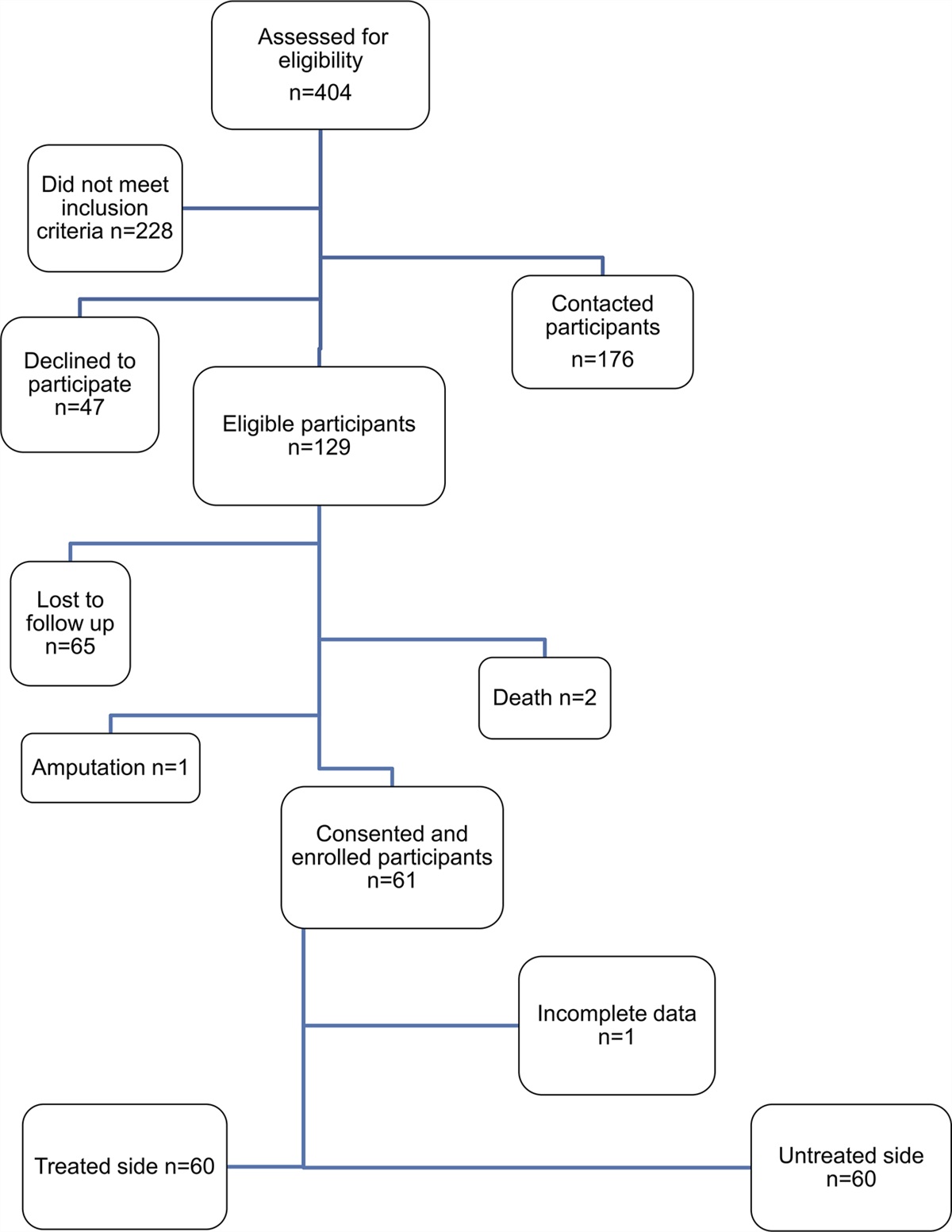
Results Characteristics of the PatientSixty patients met the inclusion criteria for ORIF for non-open Weber-B-type ankle fractures between January 2006 and July 2016 with a minimum 2-year follow-up period (Figure 1).
 Figure 1:
Figure 1: Overview of study design.
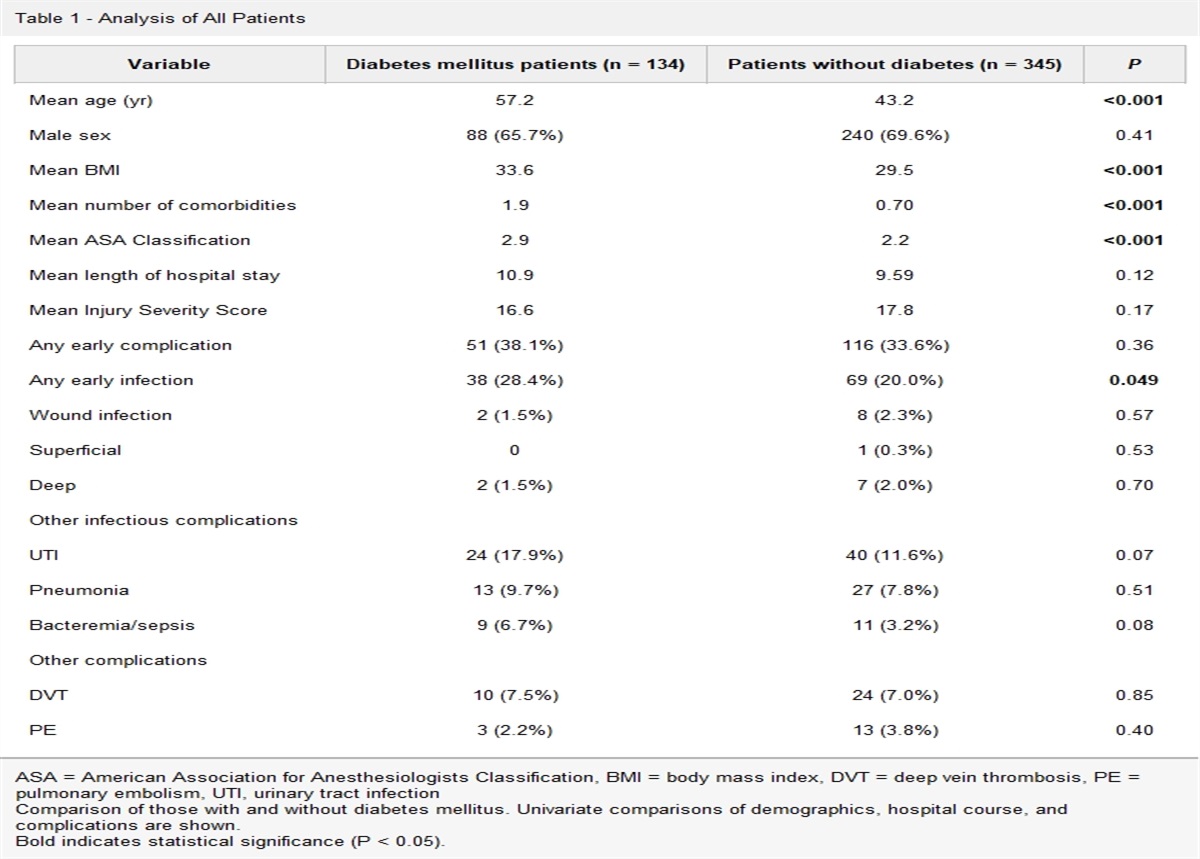
The demographic and disease-related characteristics and variables of the cohort are presented in Table 1. Twenty-one patients with and another 40 without syndesmotic screw participated in the clinical examination. There were no new ipsilateral fractures of the lower extremities during the follow-up period. For detailed findings regarding the study population in Kohake et al.21
Table 1 - Patients Demographics and Baseline Data Demographic Variables Subjects Mean (n = 60) Age (yr)a 56 ± 16 (range, 23-85) Male sex 32 (52%) Female age >45 24 (40%) BMI (kg/m2)a 27 ± 5 (range, 16-44) Current smoker 19 (31%) Diabetic 3 (5%) Anatomical realignment scorea,b 32 ± 3 (range, 26-34) Follow-up (yr)a 6.2 ± 3 (range, 2-12)BMI = body mass index
aThe values are given as the mean, standard deviation and range.
bModified according to Phillips et al.19 Maximum 34.The mean clinical outcome scores ranged from satisfactory to good. The range of motion of the treated side was reduced for a mean of 7° (±10.5, 95% CI, 4.3 to 9.7) compared with the untreated side.
At follow-up, 16 (28%) patients had a KLS grade 2 or higher (Tables 2 and 3). No significant correlation was found between the KLS grade and T-score of the treated foot and the KLS grade and modified anatomical score by Phillips in an ordinal regression model.
Table 2 - Clinical Outcome Clinical Outcomesa AOFAS 87.8 ± 11.3 (95% CI, 59.0-100.0) FFI painb 6.0 ± 8.7 (95% CI, 0-36.0) FFI functionc 9.6 ± 13.7 (95% CI, 0-50) OMAS 88.1 ± 18.0 (95% CI, 30.0-100.0) Hannover-scored 32.5 ± 14.1 (95% CI, 20.0-73.0) SF-36 PCS 52.6 ± 8.9 (95% CI, 24.1-63.2) SF-36 MCS 51.3 ± 8.3 (95% CI, 22.5-65.4) ROM treated, degree 46.3 ± 11.6 (95% CI, 4.0-70.0) ROM untreated, degree 53.3 ± 9.3 (95% CI, 30.0-80.0)95% CI = 95% confidence interval, AOFAS = American Orthopedic Foot and Ankle Society score, FFI = Foot-Function-Index, MCS = Mental Component Summary, OMAS = Olerud-Molander-Ankle-Score, PCS = Physical Component Summary, ROM = Range of motion, SF-36 = Short Form Health Survey-36
aThe values are given as the mean, standard deviation and confidence interval. Subjects mean n = 60.
bLower values indicate less pain and impairment in function (scale 0 to 100).
cLower values indicate less pain and impairment in function (scale 0 to 100).
dLower values indicate less impairment in function (scale 20 to 100).
KLS = Kellgren-Lawrence-Score, OA = Osteoarthrosis
aRadiologic outcome was evaluated in terms of the graduation as described by Kellgren et al.20bRadiographs are missing from three patients.
cIncrease of KLS between time of surgery and follow-up.
The overall mean (semi)-QUS T-score of the bone density measurement of the treated foot was −0.6 (±1.1, 95% CI, −0.89 to −0.34). This was significantly lower than on the untreated side (−0.3, 95% CI, −0.52 to −0.09, P = 0.05). QUS measurements showed an improvement at the treated foot of 22.0 (95% CI, −20.0 to 63.4) for SOS and 4.7 (95% CI, −7.0 to 16.3) for SI, but a reduction of −2.1 (95% CI, −3.5 to −0.7) for BUA compared with the untreated foot (Table 4).
Table 4 - Bone Density Measures of the Treated and Untreated Side Variable Treated Side (n = 60) Untreated Side (n = 60) Δ Δ (95% CI) P QUS T-score −0.6 ± 1.1 −0.3 ± 1.2 −0.3 −0.5 to −1.0 <0.05 QUS Z-score −0.2 ± 1.1 0.1 ± 1.2 −0.3 −0.6 to −0.1 <0.03 SI 7.5 ± 19.3 2.7 ± 48.1 4.7 −7.0 to 16.3 <0.418 SI T-score 1.3 ± 19.3 −3.5 ± 48.1 4.7 −7.0 to 16.3 <0.418 SI Z-score −14.0 ± 1.6 −14.3 ± 3.0 0.3 −0.4 to 1.0 <0.418 BUA (dB/MHz) 70.0 ± 7.2 72.0 ± 8.5 −2.1 −3.5 to −0.7 <0.004 SOS (m/s) 1,361.0 ± 56.0 1,339.0 ± 167.0 22.0 −20.0 to 63.4 <0.294 Calcaneus thickness (mm) 50.0 ± 4.0 49.4 ± 4.0 0.5 0.1 to 0.9 <0.10BUA = broadband ultrasound attenuation, CI = confidence interval, SI = stiffness index, SOS = speed of sound
Mean (SD) quantitative ultrasound (QUS) measures in 60 patients in the two groups of treated and untreated side. Paired two-tailed Student's t-test used testing differences in bone measurements between treated and untreated sides.
After ORIF, 23 of the 60 patients who underwent QUS had osteopenia or osteoporosis according to the DXA criteria. Three patients had a history of osteopenia before the surgery. In two patients, it was observed on both sides, and in one patient, only on the treated side. Only one patient had osteoporosis. One of the five patients with postoperative bone density reduction exclusively on the treated side developed osteoporosis before surgery. Three of 18 patients with bilateral postoperative bone density reduction had osteopenia or osteoporosis before surgery (Figure 2).
 Figure 2:
Figure 2: Systemic bone quality prior and after surgery. QUS = quantitative ultrasound.
Even eight and more years after the operation, there was a significantly lower T-score in the treated foot compared with the untreated side (n = 21 participants; treated side −0.63 ± 1.1 (95% CI, 0.79 to 1.5) versus untreated side −0.08 ± 1.5 (95% CI, 0.9 to 2.1, P = 0.001). In 21 patients, the follow-up period was more than 8 years. The follow-up was 2 to 8 years in 39 patients. More than one third (38%) of the patients in both groups showed a decrease in bone density on the treated side. The T-score in the group with more than 8 years of follow-up was lower, but there was no significant difference compared with the patients with less than 8 years of follow-up (Table 5). The T-score remains diminished even upon the exclusion of female participants after menopause (Table 6).
Table 5 - Bone Density Measures of the Treated Side Below and Above 8 yr After Operation Variable FU < 8 yr FU ≥ 8 yr Δ Δ (95% CI) P BD reduced n (% of FU) 15 (38) 8 (38) — — — BD non-reduced n (% of FU) 24 (61) 13 (62) — — — QUS T-score −0.5 ± 1.1 −0.6 ± 1.1 −0.03 −0.6 to 0.5 0.894 QUS Z-score −0.2 ± 1.1 −0.1 ± 1.1 0.05 −0.5 to 0.6 0.690 SI 5.1 ± 18.6 12.0 ± 20.2 6.9 −3.4 to 17.3 0.962 SI T-score −1.1 ± 18.6 5.7 ± 20.2 6.9 −3.4 to 17.3 0.962 SI Z-score −14.3 ± 1.6 −13.2 ± 1.5 1.0 0.2 to 1.9 0.668 BUA (dB/MHz) 69.3 ± 7.4 69.8 ± 6.9 0.4 −3.4 to 4.3 0.625 SOS (m/s) 1,352.3 ± 52.8 1,375.9 ± 59.1 23.6 −6.2 to 53.4 0.856 Calcaneus thickness (mm) 49.5 ± 3.6 50.7 ± 4.3 1.1 −0.9 to 3.3 0.34595% CI = 95% confidence interval, BD = bone density, BUA = bone ultrasound attenuation, FU = follow up, QUS = quantitative ultrasound, SI = stiffness index, SOS = speed of sound
Distribution and mean (SD) QUS measures of 60 patients and treated side in the two groups below and from 8 years after operation. BD non-reduced is defined T-score > −1.0. BD reduced is defined T-score < −1.0 or below. Unpaired two-tailed Student's t-test used testing differences in T-score between the ages.
Distribution and mean (SD) QUS measures of 38 patients and treated side in the two groups below and from 8 years after operation. BD non-reduced is defined T-score >−1.0. BD reduced is defined T-score <−1.0 or below. Unpaired two-tailed Student's t-test used testing differences in T-score between the ages.
95% CI = 95% confidence interval, BD = bone density, BUA = bone ultrasound attenuation, FU = follow up, QUS = quantitative ultrasound, SI = stiffness index, SOS = speed of sound
We found significant positive correlations between the T-score and the AOFAS (Pearson r = 0.503, P = 0.0001), OMAS (Pearson r = 0.410, P = 0.001), and SF-36 physical component summary (PCS) (Pearson r = 0.266, P ≤ 0.05) (Table 7). A negative correlation was found between the T-score and the HS (Pearson r = −0.353, P = 0.006). A significant regression weight for the potential confounding variables age and nicotine abuse in the linear regression model was observed only for the AOFAS score (β = 0.918, P ≤ 0.01). There was only a trend without significance for a correlation between age and nicotine abuse and the Olerud Score, HS, SF-36 PCS, and mental component summary (MCS) (Table 7).
Table 7 - Correlation Between T-Score Measurements at the Calcaneus of the Treated Ankle Fracture Side and Clinical Outcomes Score Correlation Analysisa Linear Regressionb Pearson r P-Wert Beta P-Wert AOFAS 0.503 0.0001* 0.918 <0.01** FFI pain −0.229 0.079* 0.324 0.275** OMAS 0.410 0.001* 0.673 0.347** Hannover-score −0.353 0.006* 1.006 0.197** SF-36 PCS 0.266 0.040** 0.099 0.695** SF-36 MCS −0.112 0.392* −0.043 0.839**AOFAS = American Orthopedic Foot and Ankle Society, FFI = Foot-Function-Index, OMAS = Olerud-Molander-Ankle-Score, MCS = Mental Component Summary, PCS = Physical Component Summary, SF-36 = Short Form Health Survey-36
aCorrelation analysis performed using Pearson correlation between clinical outcomes and mean T-Score values for treated side n = 60.
bLinear regression performed investigating correlation between clinical outcomes and mean T-Score values for treated side, while controlling for age and smoking status.
*P ≤ 0.01, **P ≤ 0.05.
Bone quality influences clinical outcomes following fracture fixation. Several studies assessed the correlation with outcomes parameters in calcaneal fractures,10 ankle fractures9 or tibial plateau fractures.1,22 The studies used several methods to measure the bone density. Following ankle fusion, bone density measurement in the calcaneus, as established by QUS, revealed a significant reduction in bone density, but no statistically significant correlation with clinical outcome.8
The purpose of this study was to evaluate whether bone density, as assessed on the uninjured and injured sides, differed from each other, showed a persistent change, or correlated with radiological and clinical outcomes.
We found a significantly lower quantitative value for T- and Z-scores and BUA in the treated foot than in the contralateral foot (Table 4). There was only a statistical tendency towards higher bone density measured for SI- T- and Z-scores and SOS. Several years after the operation, these results were evident with the T-score, whereas an insignificantly higher tendency towards the other bone measurements and thus higher bone density was measured in the fracture side group from 8 years postoperatively (Table 5). On an average, the T-score was lower on the injured side. However, manifest osteoporosis post-surgery operation was present in only 8% (n = 5) of the patients. In 30% (n = 18), we measured an osteoporosis of both sides. There was significant regression in the AOFAS score and FFI pain in all cases. A trend was found for the Olerud score, HS, SF-36 PCS and MCS, but significance was not reached. The small sample size and low power of the study may have contributed to this finding. When controlling for risk factors, nicotine abuse, and age, there was only a significant regression in AOFAS score.
We could not find a correlation between the KLS grade and the bone density or the quality of realignment through ordinal regression. Therefore, we assume that the quality of realignment did not influence the development of osteoarthritis in our study, or there was an influence of osteoarthritis on bone density.
In two studies on the correlations between outcome and bone density, HU measurements by CT-Scans were used instead of DXA.9,10 In particular, the relationship between bone density and outcome was examined in both studies. The study population was similar to ours, with 64 and 43 participants, respectively. However, both studies were limited by their retrospective design, unaccounted confounding variables, and disadvantages of HU measurement as a non-volumetric measurement procedure. Nevertheless, they established a correlation between reduced bone density and outcomes of ankle and calcaneal fractures. Possible reasons for the reduced HU values on the injured side have not been elucidated by Warner et al.
Lee et al also reported reduced HU values as indicators of reduced bone density after calcaneal fractures on the injured side. The authors correlated this result with a reduced Böhler angle and increased calcaneal width. Neither study detailed whether there was a reduction in the bone density on the uninjured side.
QUS is a reasonable alternative method for bone density measurement compared with CT and DEXA with a sufficiently documented positive correlation between SOS/BUA and BMD.23 QUS can adequately distinguish between normal and osteoporotic bone structure.24 DXA and QUS measurements are comparable.13,25 Along with the International Society for Clinical Densitometry position statement, peripheral measurements such as QUS are useful for assessment.26
The disadvantages of measuring bone density using DXA or CT are that they are non-volumetric methods associated with significant radiation exposure. In our study, we used QUS to collect data on bone density and volumetric values by measuring BUA and SOS. The participants were not exposed to ionizing radiation. Another advantage is the opportunity of measurement at single bones in the foot, contrary to DXA which is commonly used in spine and femur.27 In addition, the QUS is cheaper and easier to use in daily clinical practice.24
The current study had some limitations. The AOFAS is not a validated scoring system. However, we used it for the study as it is frequently employed in the scientific literature for assessing outcomes following foot surgeries or injuries. Our intention was to achieve comparability with existing literature. Given the small number of cases, the data can only be used to generate the hypotheses. Consecutive series of patients treated by a single surgeon using the same surgical and postoperative protocols were retrospectively included. In addition, unaccounted confounding variables may exist, and the data derived in this study are device specific. Therefore, these results may not necessarily be applicable to other QUS devices. Measurements from any value preoperatively or several times postoperatively were not possible owing to the retrospective design. Therefore, conclusions regarding reduction in bone density as a result of fractures are not possible. We were unable to answer the question of whether it remained unchanged or was already present due to other factors.
ConclusionIn our cohort, the quantitative values of bone density (T-score and Z-score) of the treated feet were significantly lower than those of the uninjured ankles. This difference persisted for up to eight years post-surgery, without statistical significance. The reduction in bone density in the T-score decreased over time but never returned to the values of the untreated foot (Table 5). We observed a reduction in bone density on both sides. We observed a significant correlation between the postoperative outcomes and decreased bone quality using only one scoring system (AOFAS). Relevant regressors may be missing in the model, so that the estimated coefficients can only be interpreted causally to a limited extent. Despite the significantly lower bone density on the injured side than on the uninjured side, we did not observe any loss of reduction or loosening of the implants in our study. Further studies should investigate these results in larger cohorts by using preoperative bone density measurements. Furthermore, we investigated the correlation between these changes and the bone metabolism. The cause of the decreased unilateral bone density after ankle arthrodesis remains unknown.8
References 1. Ali AM, Saleh M, Eastell R, et al.: Influence of bone quality on the strength of internal and external fixation of tibial plateau fractures. J Orthop Res 2006;24:2080-2086. 2. Johanson NA, Litrenta J, Zampini JM, et al.: Surgical treatment options in patients with impaired bone quality. Clin Orthop Relat Res 2011;469:2237-2247. 3. Soubrier M, Dubost J-J, Boisgard S, et al.: Insufficiency fracture. A survey of 60 cases and review of the literature. Joint Bone Spine 2003;70:209-218. 4. Kato M, Warashina H, Kataoka A, et al.: Calcaneal insufficiency fractures following ipsilateral total knee arthroplasty. Injury 2021;52:1978-1984. 5. Jeong M, Jin JW, Shin SJ, et al.: Calcaneal insufficiency fracture after ipsilateral total knee arthroplasty. J Bone Metab 2016;23:45-48. 6. Cakmak S, Mahiroğulları M, Kürklü M, et al.: Bilateral femoral neck stress fracture following bilateral total knee arthroplasty: A case report. Acta Orthop Traumatol Turc 2012;46:312-315. 7. Gaedke IE, Wiebking U, O'Loughlin PF, et al.: Clinical and radiological mid- to long-term outcomes following ankle fusion. Vivo 2018;32:1463-1471. 8. Wiebking U, Gaedke I, O'Loughlin FP, et al.: Bone density loss following ankle fusion persists at long-term follow-up. Arch Trauma Res 2022;11:59-64. 9. Warner SJ, Garner MR, Fabricant PD, et al.: Bone density correlates with clinical outcomes after ankle fracture fixation. Arch Orthop Trauma Surg 2018;138:1653-1657. 10. Lee SM, Seo JS, Kwak SH, et al.: Bone density of the calcaneus correlates with radiologic and clinical outcomes after calcaneal fracture fixation. Injury 2020;8:1910-1918. 11. Link TM: Osteoporosis imaging: State of the art and advanced imaging. Radiology 2012;263:3-17.
留言 (0)