2.1 Data
We used Medicaid MAX and TAF data for 100% of Medicaid beneficiaries in all states for selected years: MAX personal summary (PS) file and other therapy (OT) files in 2011 and 2012 and TAF Demographics and Enrollment (DE) and OT files from 2016 to 2018. Data from the MAX to TAF transition period (2013 through 2015) were not included in this study as there were a mix of states with MAX and TAF data in each year, making quality examination complicated.Footnote 1 The MAX PS file and TAF DE file are annual files that include demographic, eligibility, and enrollment data on beneficiaries enrolled for at least one day during the calendar year. The OT files contain fee-for-service (FFS) claims and managed care encounter records for a variety of Medicaid services, including HCBS.
2.2 HCBS related data elements in TAF data
To identify which claims/encounter records are for HCBS, we mainly focused on three data elements that are related to HCBS (all in the OT file): type of service code (TOS), HCBS taxonomy, and the procedure code. Each of these data elements represents a potential standalone approach to identify HCBS.
TOS is a data element that contains the type of service for any claim or encounter record, including state plan and waiver claims. In MAX, the information from TOS was commonly used to identify HCBS. In TAF, the TOS has 133 service categories, including 22 categories labelled as HCBS and other categories that are not labelled as HCBS but that indicate similar services (e.g. personal care, home health, etc.). While this data element can be useful to differentiate HCBS from other services, it is directly reported by each state and states differ in how they apply the type of service codes to the same type of record. For this reason, CMS’ TAF data documentation warns about using TOS to systematically identify a specific service across different states without including information from other fields.(CMS 2020).
The HCBS taxonomy was added to MAX data in 2010 in order to better categorize waiver claims into meaningful HCBS categories,(Peebles and Bohl 2014) and soon it became the standard tool used by researchers to identify and classify HCBS. Based on procedure codes in the OT file, the taxonomy used a comprehensive (and publicly available through 2015) crosswalk to assign each 1915(c) waiver claim into 1 of 18 HCBS categories. As it was developed mainly for services provided through 1915(c) waivers, this data element is not available for most state plan claims. Unlike in MAX where HCBS taxonomy information was systematically added to the national data by CMS contractors, in TAF it is directly reported by individual states and data quality variation across states is expected. Indeed, it has been documented that in TAF the HCBS taxonomy codes reported by more than half of states were completely or mostly missing.(Caswell, Waidmann, and Wei 2021) This leads to the need for new approaches to identify and classify HCBS provided in waiver programs.
Procedure codes, mainly Current Procedural Terminology (CPT) and Healthcare Common Procedure Coding System (HCPCS) codes, provide information about the service associated with each claim. Given the data quality concerns about the HCBS taxonomy in TAF, we used procedure codes and the HCBS crosswalks to recreate taxonomy categories. HCBS crosswalks were created by Mathematica for classifying HCBS claims in MAX data into one of the HCBS taxonomy categories.(Peebles and Bohl 2014) As these crosswalks were only available if MAX data was produced for that state in the given year, the most recent national crosswalk was the 2012 crosswalk; it was available for only selected states between 2013 and 2015, and was not produced after 2016. Therefore, to obtain a relatively up-to-date crosswalk that can be used in all states, we constructed a national crosswalk by combining HCBS crosswalks published in 2012 through 2015. More specifically, we compiled the crosswalks in these four years, kept all unique mapping rules and removed duplicated ones, then we applied this combined crosswalk to TAF data from 2016 to 2018.
Other data elements that are not directly related to HCBS but were used to determine the nature of the claim include: program type code, waiver type code, claim type code, benefit type code, bill type code, and place of service. The data elements used in this study are described in Appendix Table 1.
Table 1 Types of HCBS in all HCBS claims/encounter records, by FFS vs. managed care (MC), and by 1915(c) wavier vs. state plan2.3 Data quality examinations and descriptive analysis
To make our investigation of the HCBS-related data quality in TAF more practically meaningful, we focus on the identification of HCBS claims from TAF and its two main applications relevant to how researchers commonly use Medicaid administrative data to study HCBS: identifying types of HCBS users, and classifying HCBS into specific service categories. For identifying HCBS claims, we first examined data missingness in HCBS-related data elements, and then used three approaches to identify HCBS from 1915(c) claims.
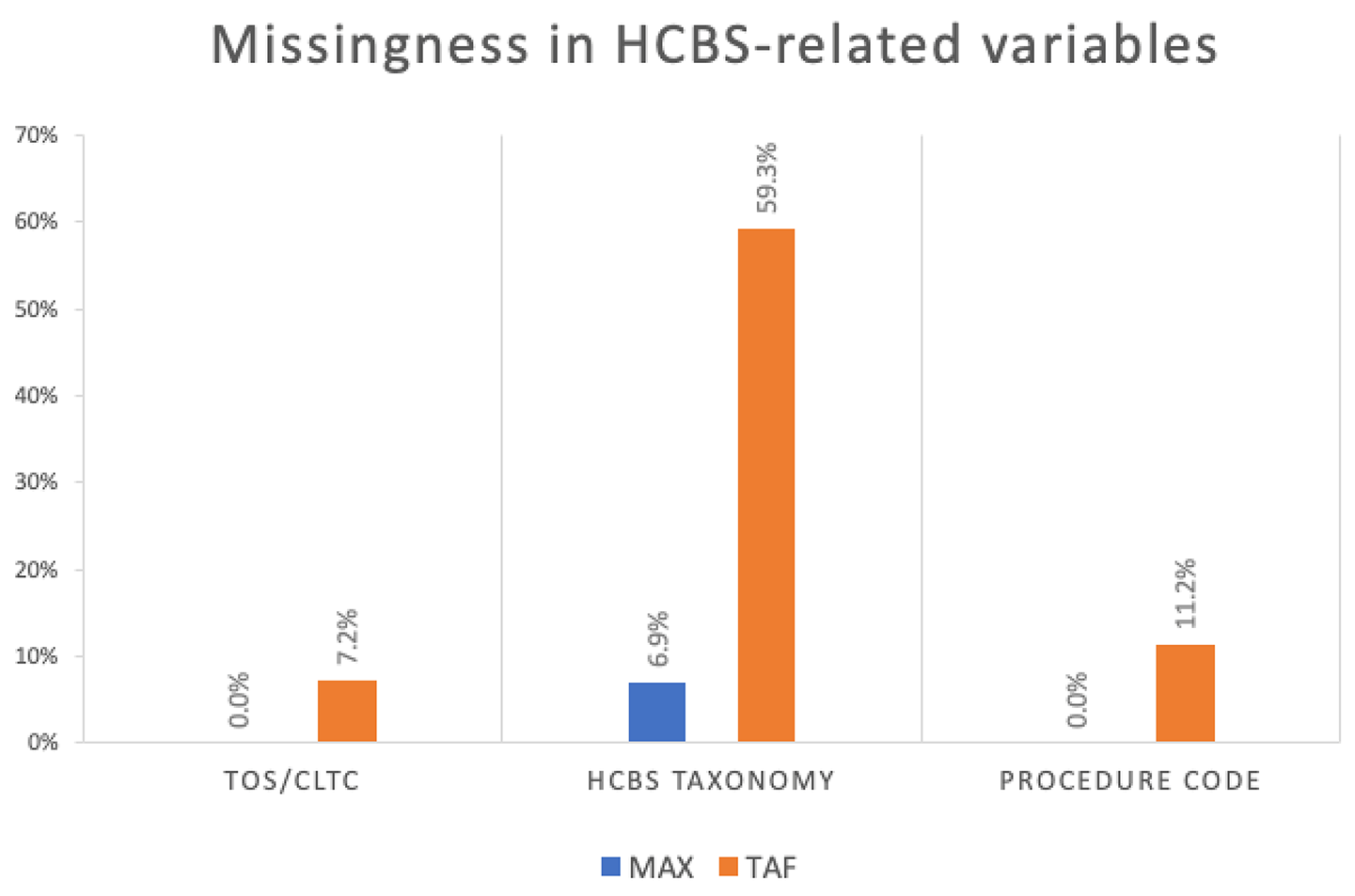
2.3.1 Assessing missingness in HCBS related variables
To examine missingness in key HCBS-related data elements in TAF, we examine how often the states’ TAF data have a missing value in the TOS, HCBS taxonomy, and the procedure code fields. For comparison, the same check was applied to corresponding data elements in MAX OT including CLTC (Community Long Term Care, a commonly used HCBS indicator in MAX data that was constructed based on TOS and waiver status), HCBS taxonomy, and procedure code.
2.3.2 Percent of 1915(c) claims that can be identified as HCBS
As we aim to examine the TAF data’s ability to identify HCBS from claims and encounter records, we used three distinct approaches to identify HCBS from 1915(c) claims, including the TOS approach, the HCBS taxonomy approach, and the procedure code approach. We choose 1915(c) claims instead of all Medicaid claims as the denominator, because services provided through 1915(c) are by design HCBS, and thus we can use 100% as the benchmark when we use different approaches to identify HCBS among 1915(c) waiver claims.
For TOS, as this data element includes 133 service types for a large variety of Medicaid services, the scope of HCBS needs to be determined before it can be used as an HCBS indicator. We included all 22 categories that are labelled as HCBS services, plus 14 categories where the services have a similar nature to HCBS, including home health, personal care, private duty nursing, residential care, rehabilitation, case management, hospice, and medical equipment. Consistent with prior literature, to count these as HCBS we required the place of service for private duty nursing and hospice to be at home.(Konetzka, Karon, and Potter 2012) The list of TOS codes included can be found in Appendix Table 1. TOS can identify HCBS from both Medicaid 1915(c) waiver claims and state plan claims.
For the HCBS taxonomy, the HCBS indicator was triggered if the claim was assigned to any of the 17 categories (excluding unknown) in the HCBS taxonomy data field. This indicator was only applicable to 1915(c) waiver claims and not state plan claims.
For procedure codes, we linked them to the combined 2012 to 2015 HCBS taxonomy crosswalk, following the steps specified for these crosswalks.(Mathematica 2019) If the procedure code of a claim was assigned to one of the 17 taxonomy categories (excluding the unknown category) after being linked to the crosswalk, it was identified as a HCBS claim by the procedure code approach. This approach was applied only to 1915(c) waiver claims in this study.
To assess the performance of these approaches, we applied them among 1915(c) claims and calculated the percent of claims that can be identified as HCBS by each approach. The performance is better when this rate is closer to 100%. Similar approaches were applied to MAX data for comparison.
2.3.3 Identifying type of HCBS users
The goal for this part of the investigation is to examine the usefulness of TAF for identifying different types of HCBS users, including those who use only Medicaid state plan services, only 1915(c) waiver services, or both. The state plan users were identified as those who had one or more non-waiver claims with a TOS code for HCBS and related services. The 1915(c) waiver users were identified as those with any 1915(c) waiver claims that could be identified as HCBS by any of the three approaches described in Sect. 2.3.2.
Unlike waiver claims that can be compared to internal benchmarks, no other existing data source, to the best of our knowledge, provides state-level information about the use of Medicaid state plan HCBS. This means there is no gold standard against which to assess the performance of TOS in identifying HCBS from state plan claims. We constructed the type-of-user indicator with TAF and MAX by identifying HCBS users of state plan only, waiver only, or both, and calculated the percentage of different HCBS users among all Medicaid FFS beneficiaries. In absence of a gold standard, the consistency in the composition of HCBS user type between MAX and TAF may provide some insights into TAF performance in identifying HCBS state plan users, as these calculations from MAX were generally accepted as valid.
2.3.4 Specific types of HCBS
Beyond binary HCBS use, researchers are often interested in the classification of HCBS, i.e. the ability to classify HCBS into service categories based on information from claims or encounter records. Among the state plan or 1915(c) waiver claims/encounter records that are identified as HCBS, we applied the procedure code approach and classified the identified HCBS claims into one of 17 Taxonomy categories. We described the type of HCBS for all HCBS claims, by FFS claims vs. managed care encounter records, and by state plan vs. waiver services.





留言 (0)