The unmet needs and weaknesses identified in the sector - Health: access and care domain, have a high impact on health prevention and chronic disease management, which is often present in older populations, as it also conditions expectations of growing old in place. Bambra, Smith and Pearce (2019: 36) recognized that health at the level of the place is determined by the nature of the place itself in terms of the economic, social, and physical environment, with direct (environmental pollution, traffic) and indirect effects (access to services, quality of the neighbourhood) existing at the local level. Ferreira et al. (2021) also observed that the older adults, with low education levels and residing in areas with low population density, has lower rates of health care access, which translates into a doubly disadvantageous situation, since these older adults are potentially the most frequent users of these services.
Co-researchers disclosed the increasing difficulty of accessing primary healthcare (PHc) in the place where they resided, which resulted from a combination of multiple factors: (1) continued public disinvestment in low density regions, especially subsequent to the economic crisis of 2009, which has resulted simultaneously in the low rate of replacement and/or less urgency regarding the replacement of health professionals, (2) public transport network unsuitable for the needs of populations and progressively scarcer due to reduced demand; (3) increase in health needs associated with ageing and the occurrence of events with high traumatic potential (forest fires); and (4) the progressive decrease in the economic power of the retired population.
A study in the interior of southern Portugal (Alentejo), whose high level of population dispersion and low population density closely resemble that in the CR55+ (Freitas & da Costa, 2021) revealed that the accessibility to public health care (PHc) is only generally adequate for those Baixo Alentejo residents with their own automobile, since public transport is insufficient. The authors emphasized, however, that, given the economic capacity and physical condition to drive their own car, the issue of accessibility to PHc is not problematic, except when considering the dimension of equity, a critical factor in this type of assessment.
In the case of the three participant Arganil parishes, PHc access is more problematic because some health services, despite having adequate physical infrastructures, were closed or only worked a few days a month due to a shortage of qualified workers (doctors and nurses) who are either not attracted to the region, or were not replaced in case of retirement, a fact which leaves the population underserved and reduced the region’s ability to attract population. As Slater (2013) suggested, we need to think about the place where we live also in terms of life opportunities, understanding why individuals live where they live, why this place has the characteristics it has and how it enhances the process of selective exodus. Bambra et al. (2005: 109) emphasized the same point: “The relationship between health and place - and the health inequalities that exist between places - are to a large degree politically determined: Place matters for health, but politics matters for place”.
The co-researchers’ proposal for mitigating the local problem of PHc access was similar to that recommended in Freitas and da Costa (2021), which involved the regular provision of flexible transport by the parish council on a copayment basis to ensure transport. For this to happen, however, some PHc facilities had to be reopened or restructured. For regions with identical characteristics, Pisco (2011) and Rita (2021) proposed an integrated reorganization of health care provision, promoting close coordination between PHc and other more differentiated providers, with resources for the telemonitoring of chronic patients and the use of itinerant health teams able to move regularly throughout the region; they proposed the opening of pilot programs. These types of solutions would require an improvement of telecommunication networks to guarantee the safety of both users and providers so as to guarantee telemonitoring and the communication of essential data.
The academic researchers were surprised to observe that the co-researchers equated their needs for health conditions and land and forest management. This type of evidence can only be achieved in a collaborative research context where the co-researcher’s perspective is clear and understandable, giving relevance to the methodology used. These co-researchers found that the provision of PHc at the local level is interdependent with policies to attract and fix populations. The effective implementation of such policies would leverage conditions to improve quality of life in these regions, including attracting investment to promote job setting and qualified human resources, as well as the definitive reorganization of essential public services. What was required was proper spatial and forest management and planning, improvement of road and mobile communication networks, and the adoption of a responsible and scientifically informed approach to forest management. Over the past 50 years, the local landscape has increasingly been overrun by pine (Pinus pinaster) and eucalyptus (Eucalyptus globulus) monocultures, due to a decreasing number of agricultural workers and an exodus of residents. These monocultures pose a significant risk for forest fires. The forest and its extraction are both an economic asset and a source of seasonal threat to these populations, as shown by the cyclical occurrence of large, increasingly frequent, and violent forest fires (Félix & Lourenço, 2019). This typology of needs and the hierarchy signalled by the co-researchers, is aligned with the perspective of quality of life associated with planning discussed by da Costa et al. (2013: 279): “Quality of life is the central objective of sustainable communities, which must seek a better quality of life for all their residents, maintaining the capacity of nature to function over time, minimizing waste, preventing pollution, promoting efficiency and developing local resources to revitalize the local economy”. Any approach, however partial, toward achieving this goal, will improve the permanence and safety of people in place and generate a favourable environment for the more efficient and sustainable provision of essential services. In addition, forest (de)planning and fire risk have a potential impact on the physical and mental health of populations, as the coresearchers emphasized. The fact that they are surrounded by a disorderly and poorly managed forest with a high risk of fire significantly increases residents’ levels of stress and anxiety, due to life-threatening events in recent decades.
“We live in the mountains, and we are used to fire…but when it gets hot, from late spring until the first autumn rains, our days and nights are restless… the hell we went through with the 2017 fire has been forever etched in our memories!” (Co-researcher, 70 years).
Research has documented the incidence of post-traumatic stress disorder (PTSD) in communities exposed to forest fires (Bryant et al., 2014), following the Victoria, Australia, catastrophe known as Black Saturday. In Portugal, following the 2017 forest fire wave, the very one mentioned by all coresearchers, Pereira et al. (2021) tracked a group of adolescents (n = 1828 young people; 6–18 years old) who were exposed to a traumatic forest fire event, some of whom were from Arganil. Of these, 4.6 per cent (n = 84) showed PTSD, adaptation disorder, separation anxiety and grief, while 2.2 per cent (n = 41) showed a higher risk of failure and school dropout. No research was found dealing specifically with pathology in older adults exposed to forest fires. However, according to Heid et al. (2017), older adults exposed to natural disasters, particularly violent ones, are also likely to show signs and symptoms compatible with PTSD, in severity varying inversely with social cohesion levels in the surrounding community. This stresses the importance of neighbourhood networks as potential factors reducing PTSD incidence. This last point highlights the added value of cohesion and local support networks, directly relating to unmet needs that were pointed out by coresearchers in the domain Living in Place – topophilia. Threats to co-researchers’ permanence in place (Table 5) included: night-time isolation of people living alone; poor coverage of mobile communication networks; low levels of domiciliary support for low mobility residents; and a strong sense of seasonal insecurity due to the high risk of forest fires. Participants clearly expressed that the perception of physical and emotional insecurity must be considered if the right of these communities to age safely and remain in place is to be guaranteed. When perceived insecurity is combined with the weaknesses and unmet needs presented in the domain – Community empowerment: inclusion and participation (Table 8), we are faced with a worrisome situation in which a community is potentially less resilient when confronted with adverse events that are highly likely to reoccur. The continued loss of the region’s attractiveness particularly to young and adult populations is worsened by apparently inefficient public policies regarding social cohesion and the guarantee of health care provision. This combination not only increases the potential for depopulation, but also compromises the return of former residents, reducing the resilience of these communities.
“Some of my friends who left with me in the 1970 to look for work and escape the tedium, are afraid to return or, when they do, they don’t change their official residence so as continue to guarantee a family doctor in Lisbon.” (Co-researcher, 71 years).
The weakening of solidarity and neighbourhood networks makes communities less resilient, increases the risk of exclusion, and compromises the right to belong. Buffel and Phillipson (2019: 989), citing May (2018), point out that: “If belonging is what connects us to the surrounding world, it stands to reason that the world must allow this connection to take place in order for this sense of belonging to be sustainable. Thus “belonging” entails more than identifying with a particular group – it means being accepted by others as an integral part of a community or society.”. Signalling this potential fragility by the co-researchers, highlights the importance of local social networks as essential elements of support for ageing in place.
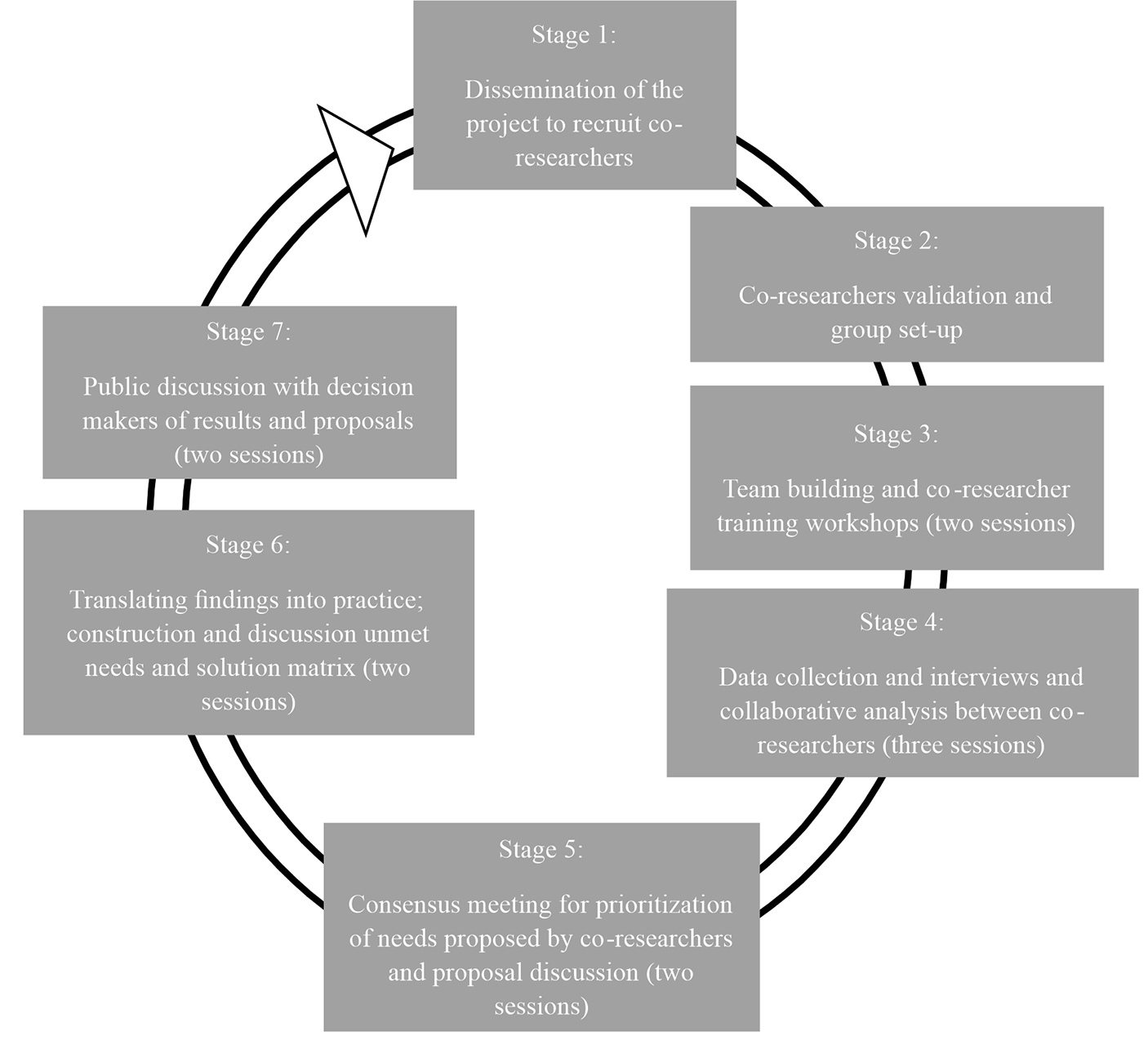
Finally, the development of Stage 7 - Public Discussion with Decision-Makers - has been instrumental in demonstrating that it is possible to correct or mitigate power imbalances in these areas as well (James & Buffel, 2022), amplifying the voice of residents through the co-investigator process and qualifying them as protagonists of change. The return of results took place in two phases, as a corollary of the CR55 + project, both aimed at discussing at regional and local level the identified and unmet needs, as well as the proposals made by older people. The first dissemination of results took place in June 2022, facilitated by academic researchers, and brought together regional health policy managers, service providers and mayors, who listened and reflected, in direct discourse, on the shortcomings and proposals for change and improvement validated by the co-investigators. The second round of feedback took place in October 2022, at the suggestion of Arganil’s Social Action Councillor, who invited local security, transport, and health authorities to the discussion, as well as various public and private actors involved in providing social support to older residents. At Stage 7, it has been shown that the training of co-investigators, involving the transfer of knowledge and appropriate training to enable them to be the authors of proposals for substantive change, is a tool that can help to reverse traditional top-down decision-making processes, combat potential levels of ageism and, at the same time, contribute to the cohesion of territories that have accumulated demographic losses, economic losses, disinvestment in public services and, consequently, losses of cohesion over time.
The WHO (2015) recognises people’s right to live at home, in the community and to age in place safely and independently. Understanding this concept implies the need to adapt the physical and social environment to daily life, knowing that most older people want to remain in an environment that is familiar to them, preferably staying in the same house, contacting the same neighbourhood, maintaining affiliation with the same community (Iecovich, 2014). The concept of place used here is a multilevel one, which involves housing, the neighbourhood and, in a broader sense, a set of conditions that allows people to enjoy a decent life: access to social networks, transportation, health resources and leisure opportunities (Fonseca & Porto, 2018). It should be noted that the co-researchers recognise as positive the existence of locally based support services, mostly provided by the social sector. These services involve both formal and informal carers and contribute to employment and the local economy. Additionally, these services maintain a sense of protection and social cohesion, despite their relative isolation and the inadequacy of some public services, particularly health services. More restrictive public policies may contribute to the weakening of these organisations and make it impossible for the older populations to age in these places with a minimum of dignity, security, and care, resulting in an even faster depopulation of these territories.


留言 (0)