
記住我

This study was based on the publicly and freely accessible database named Medical Information Mart for Intensive Care III (MIMIC-III, version 1.4). This database comprises information associated with over 40,000 distinct hospital admissions at the Beth Israel Deaconess Medical Center (Boston, USA) form 2001 to 2012 [12]. The establishment of this database was approved by the Institutional Review Boards of the Beth Israel Deaconess Medical Center and Massachusetts Institute of Technology. To apply for permission to access the database, we passed the National Institutes of Health’s web-based training course named ‘Protecting Human Research Participants’ (Certification number: 41624341).
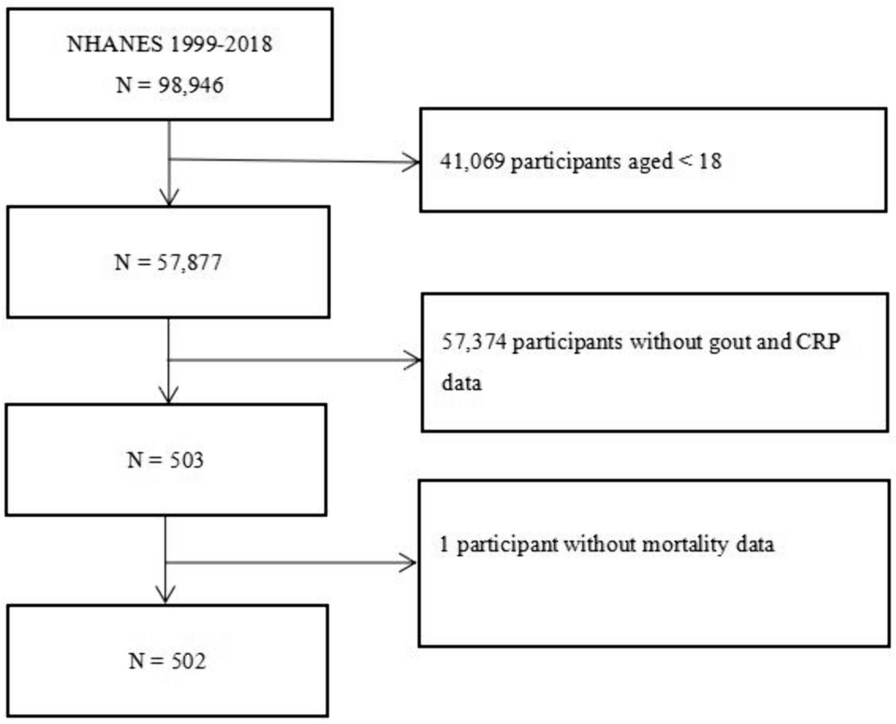
A total of 11,467 distinct patients with AKI were recorded in the database. In this study, we collected 4461 patients who were older than 18 years and the primary diagnosis was AKI at ICU admission. AKI was defined according to ICD-9 diagnostic code containing the terms “acute renal failure”. The individuals were excluded if (1) absence of data on the serum lactate level at the first admission; (2) > 5% of the required data were missed; (3) baseline data values exceeded the mean ± 3 times the standard deviation (SD) (Fig. 1).
Fig. 1
The flowchart of inclusion and exclusion procedure
Data extractionData on the clinical parameters, laboratory parameters, clinical scores and comorbidities were extracted from MIMIC-III using the Structured Query Language (SQL) with PostgreSQL tools (version 12.0). The clinical parameters included age, sex, heart rate, respiratory rate, temperature, systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), percutaneous oxygen saturation (SPO2), vasoactive drug, and RRT. The laboratory parameters included glucose, white blood cell, platelet, sodium, potassium, blood urea nitrogen (BUN), bicarbonate, chloride, anion gap, and creatinine. Comorbidities including congestive heart failure, hypertension, diabetes, stroke, chronic renal disease, chronic liver disease and malignancy were also extracted. Furthermore, the Simplified Acute Physiology Score II (SAPS II), Sequential Organ Failure Assessment (SOFA) and Glasgow Coma Scale (GCS) were calculated for each individual. The patient’s data at first admission were used as the baseline data. The primary outcome was 365-day mortality and secondary outcomes were 30-day mortality, 90-day mortality and 270-day mortality.
Statistical analysisDescriptive statistics such as mean ± SD and percentage were calculated for continuous and categorical variables, respectively. To obtain a deeper understanding of the association between serum lactate and mortality in AKI, all patients were divided into three groups by serum lactate tertiles statistically. In this study, tertiles were categorized separately as follows: Q1 ≤ 1.60 mg/dl, Q2 = 1.61–2.70 mg/dl, and Q3 ≥ 2.71 mg/dl. Continuous variables were presented as the mean ± SD and compared using one-way ANOVA or Mann–Whitney U test as appropriate. Categorical variables were summarized as percentages and compared using X2 test. The relationship between lactate and mortality was explored using Cox regression for univariate and multivariate analyses. We were based on Kaplan–Meier analysis and log-rank test to construct survival curves. The results were expressed as hazard ratios (HRs) with 95% confidence intervals (Cls). All statistical analyses were performed using SPSS 21.0 (SPSS Inc, Chicago, IL). Values of P < 0.05 were defined as statistically significant.
留言 (0)