
記住我









This study aims to utilise T1 contrast-enhanced (T1-CE) and T2 fluid-attenuated inversion recovery (T2-FLAIR) radiomic features to predict EGFR mutations and HER2 overexpression in adenocarcinoma in a personalised manner. Radiological features were derived from segmented regions of the MRI images. The collected data were divided into training and test sets according to the experimental design and were subsequently used for training and independent validation of the model, respectively. The most valuable radiological features were selected using the least absolute shrinkage and selection operator (LASSO) technique. The prediction model was developed using the support vector classifier (SVC) method. A detailed description and analysis workflow can be seen in Fig. 1.
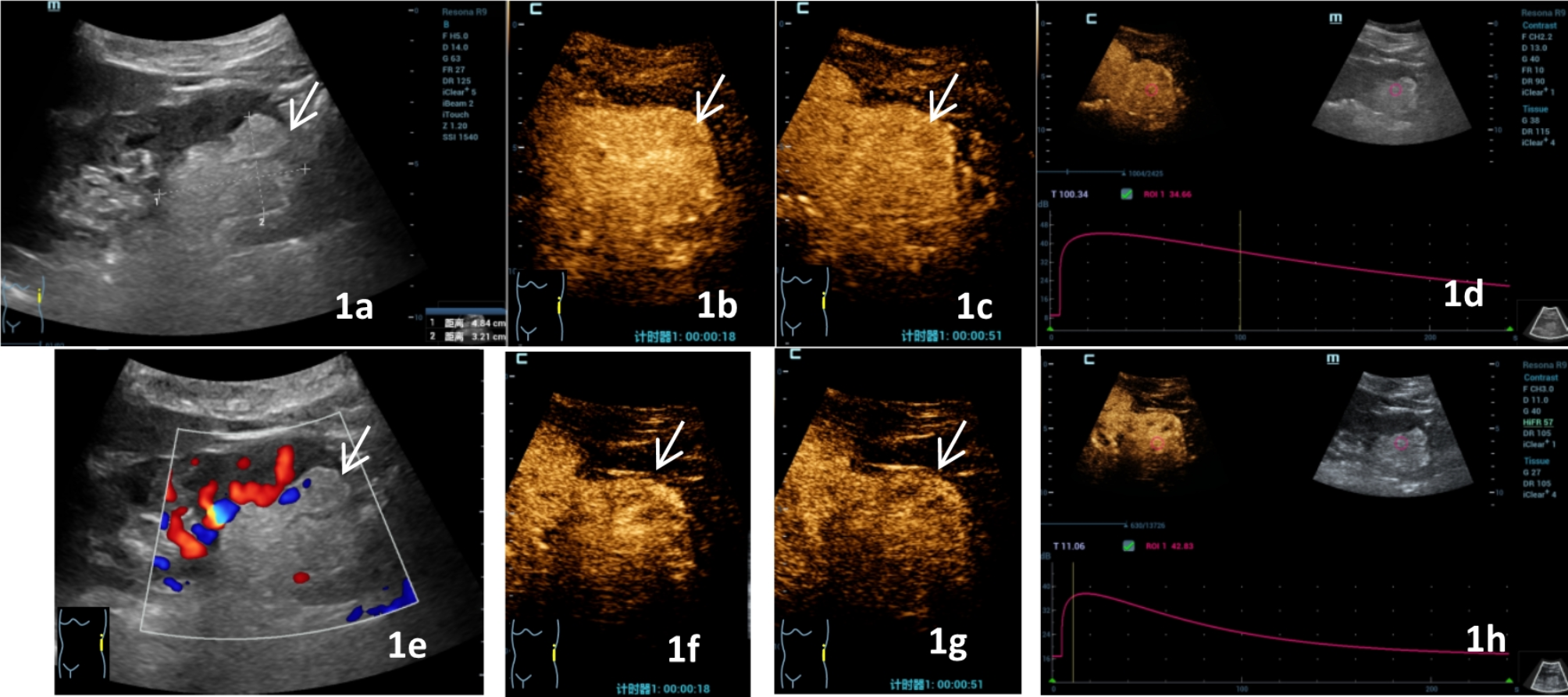
Fig. 1
Workflow for radiomics modeling and analysis including segmentation of metastases and examples from MR images
ParticipantsBetween January 2015 and January 2022, this two-centre retrospective cohort study was authorised by our hospital’s ethics committee. Patients were initially diagnosed with brain metastases resulting from cancer using MR imaging and genetic testing. Pathology confirmed the diagnosis of all primary lesions. All MR-confirmed metastases were reported independently by nuclear medicine specialists and radiologists with at least five years of board certification.
To be included in the study, patients had to meet the following criteria: (1) primary tumour pathologically confirmed as adenocarcinoma by surgery or biopsy, (2) presence of brain metastases, (3) brain metastases confirmed by pathology, and (4) assessment using MR imaging. The exclusion criteria were as follows: (1) various types of original malignancies, (2) absence of genetic testing, (3) patients who had received systemic therapy, and (4) lack of follow-up data.
EGFR mutation status and overexpressed HER2All adenocarcinoma patients underwent an evaluation of their EGFR status using next-generation sequencing technologies.
The HER2 status of all patients with adenocarcinoma was assessed using immunohistochemistry (IHC) or fluorescence in situ hybridisation (FISH) [12]. Two independent pathologists reviewed the patients’ IHC results at the time of the HER2 status assessment. Patients were considered negative for HER2 if IHC results were 0/1 + and positive if IHC results were 3+. HER2 status was further determined using FISH results when IHC results were 2+ [12, 13].
MR image acquisitionBrain MR images were obtained from patients with adenocarcinoma at their initial diagnosis of brain metastases. At the First Affiliated Hospital of Xinjiang Medical University, patients underwent evaluation using a 3.0 T MR scanner (MAGNETOM Skyra, Siemens Healthineers, USA) and a 3.0 T MR scanner (Discovery MR750, GE Healthcare, USA). At Changzhi People’s Hospital, a 1.5 T MR scanner and a 3.0 T MR scanner (MAGNETOM Verio, Siemens Healthineers, USA) were employed. The T1-CE and T2-FLAIR sequences, which are commonly used for detecting brain metastases, were chosen for the extraction of image features [7, 14,15,16,17]. The image matrix size varied from 240 × 240 to 256 × 256 pixels, with slice thickness ranging from 1 mm to 6 mm. Additional scanning parameters for these sequences are presented in Supplementary Table 1.
Image segmentationRegions of interest (ROIs) on the MR images of the aforementioned sequences were delineated using ITK-SNAP [18] around the metastases. To minimise the impact of clustering, only one ROI per image was selected. Initially, ROIs were created around each axial section of the metastatic profile to examine tumour heterogeneity. Subsequently, areas of oedema, haemorrhage, cystic changes, and necrosis were excluded from the images. Representative sections of the metastases for each sequence were chosen. The red spots in Fig. 1 indicate the axial distribution of the metastases.
Radiomics features extractionBefore feature extraction, several preprocessing steps were undertaken to enhance texture recognition. First, the bin width was set to 25. Second, Z-score normalisation was applied to the MR images. Finally, cubic interpolation was utilised to resample the ROIs isotropically to an in-plane resolution of 3 × 3 × 3 mm, ensuring the consistency of proportions and orientation in the acquired 3D features [19].
Prior to radiomic feature extraction, each image underwent preprocessing with eight image filters to highlight specific details and reduce noise. These filters, comprising Wavelet (HH, HL, LL, LHH, LLL), Laplacian of Gaussian (sigma = 1, 2, 3), Square, Square Root, Logarithm, Local Binary Pattern, Gradient, and Exponential, were used to evaluate three different categories of radiomic features in each image. A total of 1,409 radiomic features were extracted per tumour, with an equivalent number of features generated from both T1-CE and T2-FLAIR sequences. The radiomic features were extracted using the open-source Python program Pyradiomics (https://github.com/Radiomics/pyradiomics). Various radiomic features were utilised for this extraction process.
Establishment of radiomics featuresData from Institutions 1 and 2 were combined and subsequently divided into training (70%) and test (30%) sets after manually segmenting and extracting features from all ROIs for each participant. A PyRadiomics-based pipeline, previously tested, was used to extract radiomics features and conduct feature selection. Among the radiomics features retrieved, there were several duplicated, unstable, and irrelevant imaging characteristics. Feature selection methods were used to identify and select the most informative, stable radiomics features. This approach also helps prevent overfitting. The final feature set was established using the LASSO method and recursive feature elimination.
Model buildingA radiomics model was constructed using a linear SVC based on these two MR image sequences after feature selection. To address the data imbalance, the synthetic minority oversampling technique algorithm with default parameters was applied [20]. This created minority instances along a line connecting a minority instance to its nearest neighbours.
Interobserver reproducibility evaluationIn our radiomics inquiry, ROI segmentation repeatability and radiomics feature extraction reproducibility are integral to the interobserver reproducibility process. The repeatability of the ROI segmentation was tested through multi-reader segmentation. For this purpose, two independent radiologists manually delineated ROIs in four MR sequences using the same annotation program, ITK-SNAP (http://www.itksnap.org). For reproducible radiomics feature extraction, we employed PyRadiomics, an open-source program, to compute the radiomics features and to perform image preprocessing. The feature extraction process was guided by a.yaml file, allowing separate individuals to replicate the extraction of radiomics features outlined in our study using the same file.
Pleas einclude the supplier’s information.
Statistical analysisSPSS (version 22.0) was utilised for the statistical analysis. To explore group differences, we applied chi-squared tests to categorical variables and t-tests for continuous data. The model’s effectiveness was assessed using the receiver operating characteristic (ROC) curve and the area under the curve (AUC). Sensitivity and specificity metrics were calculated using a threshold of 0.5. A p-value of less than 0.05 was deemed statistically significant.
留言 (0)