
記住我






Instrument fracture inside the oral cavity is a frustrating and undesirable occurrence [15]. There is limited data available regarding periodontal instrument fractures [6, 7]. These fractures may result from procedural errors, such as excessive force application without a stable fulcrum, use of aged instruments subjected to sterilization and/or sharpening cycles, or compromised metallurgy [5, 7, 16]. On average, a curette fractures approximately after 14.34 sterilization cycles [2]. Lieu et al. demonstrated that the size of the instrument’s working end decreases when scaling cycles increase, elevating the fracture risk during instrumentation [2]. Furthermore, sharpening contributes to discernible wear of the instruments, which can lead to breakage, as reported by Lieu et al. where the #11/12 Gracey curette fractured when the blade width reduced to less than 0.55 mm [2]. This case report raises a similar incidence wherein the fractured blade exhibited a width of 0.4 mm when measured after the event.
Kwon et al. [17] explored the correlation of instrument fracture with type of procedure, breakage point, and operator expertise. Root planning exhibited the highest fracture rate (63.8%), amounting to around 16 fractures per one thousand curettes utilized. The upper one-third of the blade was the most frequent site of fracture, accounting for 44.8% of fractures, followed by the terminal shank (29.3%). Additionally, the authors reported that the fracture incidents were independent of the clinical expertise of the operator. Our case reflected a similar incidence of fracture site at the upper one-third of the blade despite maintaining stable fulcrum by the practicioner [17].
Instrument quality and maintenance, therefore, prove imperative in averting such incidents. Periodontal hand instruments are essentially made up of martensitic steel, which is well known for its durability and resistance to corrosion [18]. Tal et al. found high carbon steel (HCS) dental curettes more wear-resistant than stainless steel (SS) ones [19]. However, the widespread use of stainless steel instruments persists due to their biocompatibility, adherence to international standards (ISO7153-1), and longevity when properly maintained [7]. Innovations in instrument coatings, like multilayered filtered arc coatings, extend their lifespan and clinical utility, with some instruments retaining their clinical usefulness for up to 11 months [20]. Nonetheless, ensuring optimum instrument quality requires meticulous compliance with maintenance guidelines by clinicians. This includes conducting regular inspections before packaging to preemptively address wear and/or fatigue caused by repeated use of the instrument [6].
Fractured instrument segments entail risks of swallowing or aspiration, persistent pain, abscess formation, septicemia, or bleeding [21]. Timely removal of the fragment is essential to prevent migration into adjacent spaces; for instance, a fragment fractured on the lingual side of the mandible can migrate to the submandibular or parapharyngeal space. This may potentially cause catastrophic complications, such as laceration of the maxillary artery or jugular vein [22, 23]. Delayed removal increases the risk of infection and tissue destruction due to inflammation, thrombosis, erosion into the carotid artery or its branches, and nerve interference [24]. Hence, it is imperative to immediately search for and retrieve the fractured fragment [25], as was done in this case by maintaining a composed and calm demeanour.
In healthcare, it is crucial to promptly identify the errors and inform the patient about the potential injury [26]. A ubiquitous consensus exists regarding the ethical principle of truth-telling [27] that is the healthcare professionals have a duty to uphold patient autonomy and disclose errors that have a substantial impact on the patient’s health and well-being [28, 29]. It prompts healthcare professionals to promptly identify the errors in practice and explain the situation to the patient clearly and concisely, conveying any oral health issues and the potential consequences of inaction [30]. Additionally, offering a sincere apology is important, as it has been shown to increase patient compliance and decrease the likelihood of litigation [31]. A similar protocol was followed in our case, as the patient was promptly briefed about the incident and was offered an apology with reassurance.
Following the diagnosis and informing the patient, the subsequent step involves instrument retrieval. Several methods, categorized as surgical or non-surgical, exist for retrieving retained broken instrument segments [17] including tweezers or suction without specific manipulation, removal with another curette, or employing the double-ended magnetic instrument known as the Periotriever [17, 32]. In this particular case, a curved artery forceps was selected for its suitability for the intended task. Utilization of X-rays, MRIs, CT scans or metal detectors have been suggested in the literature to aid in the navigation of the broken fragment to minimize potential risk of damaging critical anatomical structures [33, 34]. Aperi-apical radiograph aided in accurately localizing the broken fragment in this case, which was then retrieved by curved artery forceps after creating a pathway by deflecting gingiva.
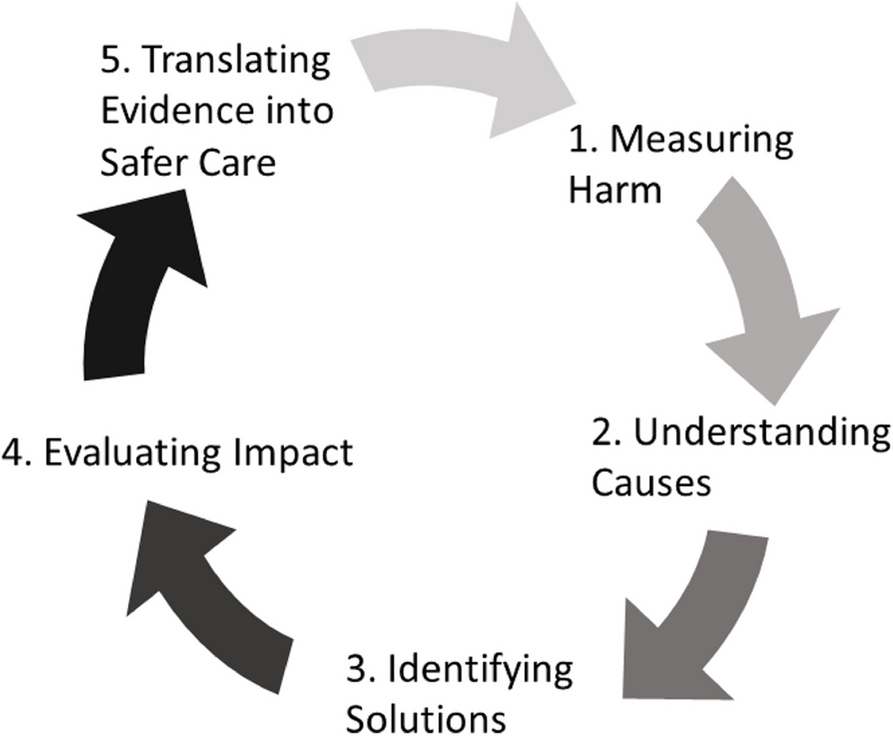
This case report reminds dentists about their ethical responsibilities and obligation to transparently inform patients about adverse events. The lack of established protocols highlighted the pressing need for guidelines. Based on the available evidence, the authors propose a protocol (Fig. 5) to manage such incidents with a published guideline for foreign body management [35,36,37]. It further encourages dental professionals to maintain composure and a calm demeanour during stressful situations, and signifies the importance of conducting thorough checks for instrument fatigue and ensuring correct equipment maintenance (Refer to Table 1 for recommendations regarding replacement of periodontal instruments).
Fig. 5
Protocol for instrument retrieval. * Indicates that the fragment must be removed before informing when visible to prevent aspiration or ingestion
Table 1 Recommendations regarding replacement of periodontal instruments
留言 (0)