
記住我




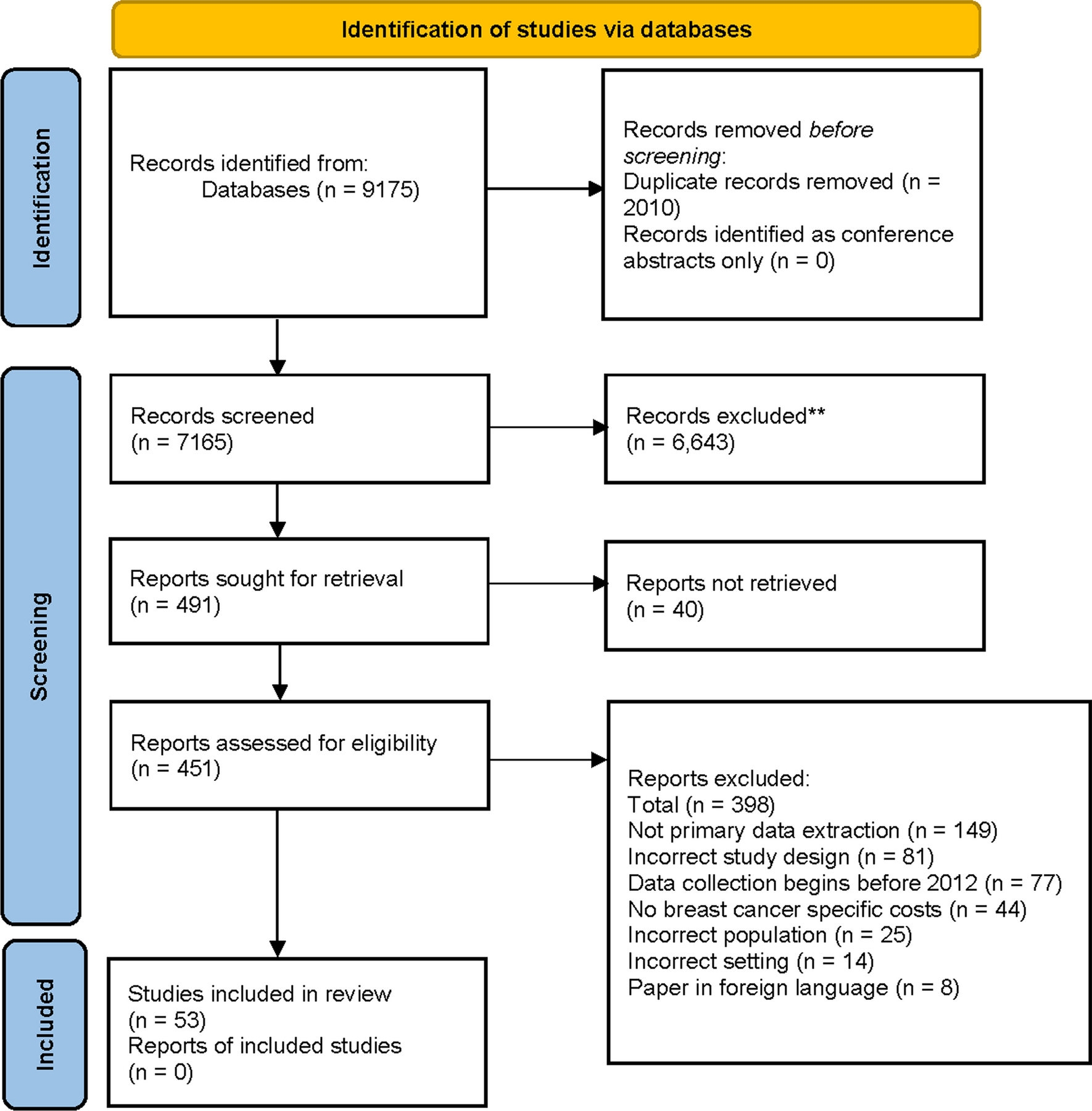


Literature searches across the three databases yielded a total of 8566 hits, which included 1383 duplicates, therefore resulting in a total of 7183 unique hits. First-round screening of titles and abstracts was performed by one investigator and identified a total of 241 hits for full-text review (Fig. 1). During second-round screening, a further 176 articles were excluded, leaving a total of 65 articles detailing utilities/disutilities associated with either T2D-related complications or treatment-related attributes for inclusion. A further three articles were identified via bibliographies of included articles. Searches of meeting abstract databases identified one relevant abstract for inclusion. The final review therefore included a total of 69 studies. Of these, a total of 39 presented findings exclusively related to acute or long-term diabetes-related complications, 15 presented findings exclusively related to the influence of treatment-related attributes on QoL, and 15 captured findings on both complications and treatment attributes. In total, 54 articles presented utility/disutility values for T2D-related complications (Table 1); these included a total of 18 studies conducted in Asia [7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24], 13 conducted in Europe [25,26,27,28,29,30,31,32,33,34,35,36,37], 13 in North America [38,39,40,41,42,43,44,45,46,47,48,49,50], 2 in Latin America [51, 52], one in the Middle East [53] and 1 in Africa [54], and 6 were multinational (or setting not stated) [55,56,57,58,59,60]. Nearly all identified studies were conducted in individuals with T2D, although two presented data gathered from general population samples [34, 56].
Fig. 1
Summary of literature searches. T2D, type 2 diabetes. Publication/study type refers to articles that were reviews, editorials, letters, case reports, secondary sources of utility values or discrete choice experiments
Table 1 Summary of studies presenting utility/disutility values for complications related to T2DT2D with No ComplicationsEleven studies were identified that provided baseline utility values for individuals with T2D with no complications, all of which used the EQ-5D-3L or EQ-5D-5L (where studies did not state which version of the EQ-5D was used it was assumed that the EQ-5D-3L was used) (Table 2) [7, 14, 16, 22, 24, 28, 35, 36, 38, 44, 49] with one additionally using the SF-6D [38]. Five of the identified studies were conducted in Asia [7, 14, 16, 22, 24], three in North America [38, 44, 49] and three in European populations [28, 35, 36].
Table 2 Utility values associated with type 2 diabetes and no complicationsUsing the EQ-5D, reported mean baseline values for individuals with T2D with no complications ranged from a low of 0.76 in a community-dwelling sample in Canada aged ≥ 40 years and with HbA1c ≥ 7% [44] to a high of 0.956 in a sample in China with mean (SD) age of 64.9 (9.1) years [14]. One study conducted in Vietnam reported a median baseline value of 1.0, which corresponds to perfect health [16], and is also slightly higher than that previously reported in a general population sample in Vietnam [61]. Differences in baseline characteristics such as age, BMI and duration of disease as well as the source of utility weights may have contributed towards the differences in baseline values between the different study populations.
For economic modeling analyses, the optimal baseline utility values should be as closely representative of the simulated patient population under investigation as possible. In particular, factors such as setting, baseline age and duration of diabetes should be taken into account and, if necessary, adjustments applied to the reference population. The description of the reference population of patients with no complications varied between studies; however, one US-based study provided a comprehensive description. Zhang et al. [49] reported a baseline utility value of 0.92 for no complications with this value referring specifically to individuals that were male, non-Hispanic white, with BMI < 30 kg/m2 and with no risk factors for cardiovascular disease, with income > USD 40,000 per annum and not treated with insulin.
Cardiovascular and Cerebrovascular ComplicationsA total of ten studies that presented disutility values for MI [10, 26, 28, 33, 37, 44, 46, 55, 57, 58], were identified (Table 3) (three studies presented utility values for MI; data not shown [11, 36, 46]). Two further studies presented disutilities for angina [10, 46], and nine studies were identified that presented disutility values for CHF [10, 27, 28, 37, 46, 49, 55, 57, 58]. In studies that utilized the EQ-5D, the reported disutility associated with an MI ranged from − 0.073 in a sample of individuals with T2D attending outpatient clinics in South Korea [10] to − 0.0119 in a sample of patients in Sweden [28]. One study also reported a positive value of + 0.004 in a post hoc analysis of the multinational LEADER trial [58]. However, this value was not an event-related disutility per se but specifically referred to the change in utility value reported in patients who experienced an MI at any point during the 36-month follow-up period rather than a recent MI and may therefore potentially have captured improvements in QoL in patients recovering from an MI. Indeed, in a post hoc analysis of ACCORD trial data, Shao et al. noted that the timing of the event relative to the timing of measurement of QoL was an important determinant of QoL and although the effect of an MI waned over time a degree of long-term impairment persisted [46]. More specifically, using the HUI-3, Shao et al. reported that the mean (SE) disutility associated with MI was − 0.042 (0.016) in the year of the event but − 0.011 (0.006) in subsequent years after the event.
Table 3 Disutility values associated with cardiovascular complicationsTwo studies reported disutility values associated with angina (two studies also reported utility values for patients with angina; data not shown [36, 46]). In a South Korean study that utilized the EQ-5D, Lee et al. reported a mean (SE) disutility of − 0.0266 (0.0114) [10], while for US-based patients, Shao et al., who utilized the HUI-3, reported a disutility of − 0.032 (0.006) in the year of event but − 0.010 (0.021) in subsequent years [46].
A total of nine studies reported disutility values for CHF [10, 27, 28, 37, 46,
留言 (0)