This systematic review summarises the available evidence on the influence of relative age on the rating of ADHD symptoms by teachers or parents, revealing a discrepancy between the impact of relative age on teacher and parent ratings. These findings contribute to our understanding of this topic by showing that teacher ratings of ADHD symptoms were influenced by relative age; in contrast, parent ratings showed no or weak association with relative age [23, 24]. Our review also confirms findings from the previous literature [3, 4] by incorporating data from more recent studies, showing that the effect of relative age on clinical ADHD diagnosis and prescribed medication has persisted. Furthermore, we extend previous systematic reviews by investigating the relative age effect in ASD, a different neurodevelopmental disorder usually diagnosed in childhood [45].
The presence of ADHD symptoms in children as reported by teachers and parents, does not automatically translate to a formal diagnosis. Distinguishing between adult-reported symptoms and the diagnostic process allowed us to explore how relative age influences symptom interpretation, independent of diagnosis. Improved knowledge about how teachers and parents perceive and report ADHD symptoms is important as both are essential informants about a child’s ADHD-type behaviours in different settings [13, 46]. Overall, our results show that teacher ratings for ADHD-related symptoms are more influenced by relative age, in contrast to parent ratings. This difference between parent and teacher reporting of ADHD symptoms could be influenced by several factors. The higher demands and limited flexibility of the school environment, the presence of large numbers of peers to compare the child with, and the less close and shorter duration of the relationship of teacher to child compared with parent to child could all cause this observational bias in teacher ratings [3, 14, 26]. The limited classroom-specific support strategies for teachers to help relatively younger children with ADHD symptoms meet classroom expectations may also influence their assessments of ADHD symptoms. Parents may also be subject to social desirability bias towards their child, potentially overlooking certain behaviours. Teacher perceptions and susceptibility to relative age bias may impact a child’s referral and diagnostic process. Teachers are more likely to identify ADHD symptoms in younger children in the school year and give higher scores on symptom scales, which are then taken into account by clinicians when doing a diagnostic assessment. Conversely, teachers might also miss ADHD symptoms in relative older children in the class as they are being referenced against their younger and slightly less mature classmates [23].
In terms of diagnosis and prescriptions, our results overall confirm an association between younger relative age and a clinical diagnosis of ADHD or prescribed medication. The strength of this association showed high heterogeneity for both outcomes. This could be explained by methodological factors such as different ways of measuring exposure and outcomes, variability in sample characteristics, sample sizes and cut-offs for ‘oldest’ and ‘youngest’ in the year; educational differences such as different curriculums, systems and policies including but not limited to rates of delayed school entry, rates of repeating school year due to failure to progress, absolute age at starting school, school classroom size; and cultural differences such as societal attitudes towards neurodevelopmental disorders or expectations around conformity and educational achievements. International variations in diagnostic and prescription practices, including access to services and who can make a clinical diagnosis, likely contribute to the observed heterogeneity, reflecting discrepancies in ADHD identification and medication use rates across countries. Such cross-cultural differences in ADHD diagnostic and treatment guidelines should be considered when interpreting the findings of international studies [3, 27, 44]. Most studies did not consistently report sociodemographic characteristics of their total sample; although six studies adjusted their analysis for some sociodemographic characteristics as potential confounders. Due to many studies relying on nationwide prescription or health record databases, data collected by primary authors were often representative of the clinically relevant populations of the area.
A persistent relative age effect was found for studies published since 2018 (when the previous systematic review was conducted) for both diagnosis and medication [1, 5, 13, 29]. This phenomenon has been documented in the literature over the past decade, so one might expect that clinicians to factor relative age into assessments, however, there is little evidence that this has occurred [37]. One reason could be the lack of guidance on how to best account for relative age in the diagnostic process, as international guidelines such as NICE and American Academy of Pediatrics do not incorporate relative age considerations [46, 47]. Other factors could be diagnostic uncertainty, clinicians’ time pressure, reliance on subjective evaluations or over-reliance on standardised questionnaires, limiting the ability perform age-matched comparisons for younger children.
The relative age effect on ADHD shows a pronounced impact in younger children attending primary school, with peak age varying in individual studies, but overall gradually diminishing through adolescence. This observation suggests that actual age and developmental expectations significantly influence ADHD identification, with early schooling years witnessing the greatest disparities [1, 2, 32, 33]. Existing literature has discounted the presence of a seasonal effect on ADHD, as variations do not align with specific seasons but shift according to local school entrance policies [38]. Previous meta-analyses have speculated that more flexible school entry could reduce the relative age effect [3, 4]. However, two recent studies found that children who were held back a year, entering school relatively later than their classmates, were more likely to be prescribed ADHD medication [11, 42]. The authors explained this may be due to systematic differences in children with delayed school entry, such as having more complex special developmental needs [42] or parents who worry more about perceived relative immaturity and neurodevelopmental diagnoses [11]. However, these findings suggest that changes to school entry policy may not have the desired effect of reducing the relative age effect. Importantly, families of higher socioeconomic status are more likely to afford deferring their child’s school entry while less affluent families are more likely to have children in the youngest school year cohort [11]. This introduces a social inequity aspect to the disparity in diagnostic rates in areas with flexible school entry policies.
While the relative age effect is well documented in ADHD, data for other neurodevelopmental disorders are still emerging. Only two studies, both from the same country using the same data source, were identified investigating the relative age effect in ASD diagnosis and children who were the youngest in their school year were more likely to be diagnosed with ASD compared with their older classmates. The reasons behind this are not clear but it is possible that immature speech or social skills of relatively younger children may be interpreted as traits of autism by referrers [5, 48]. Although the timing of identification of characteristics for many autistic children takes place before they reach school age [49, 50], no information on the age of autism diagnosis was available in the two studies to comment on the differences between autistic children diagnosed before school age and those after.
Strengths and limitations
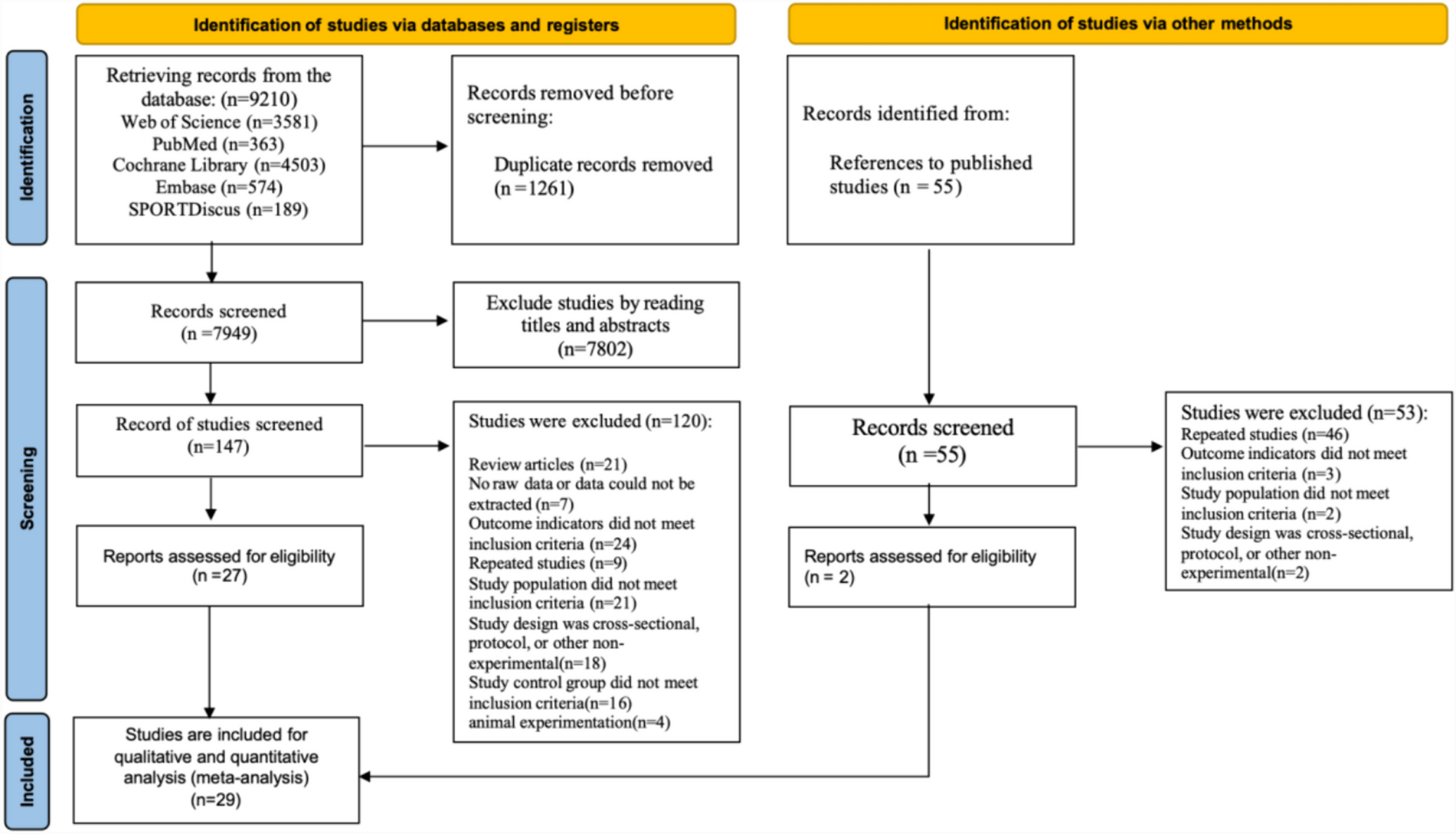
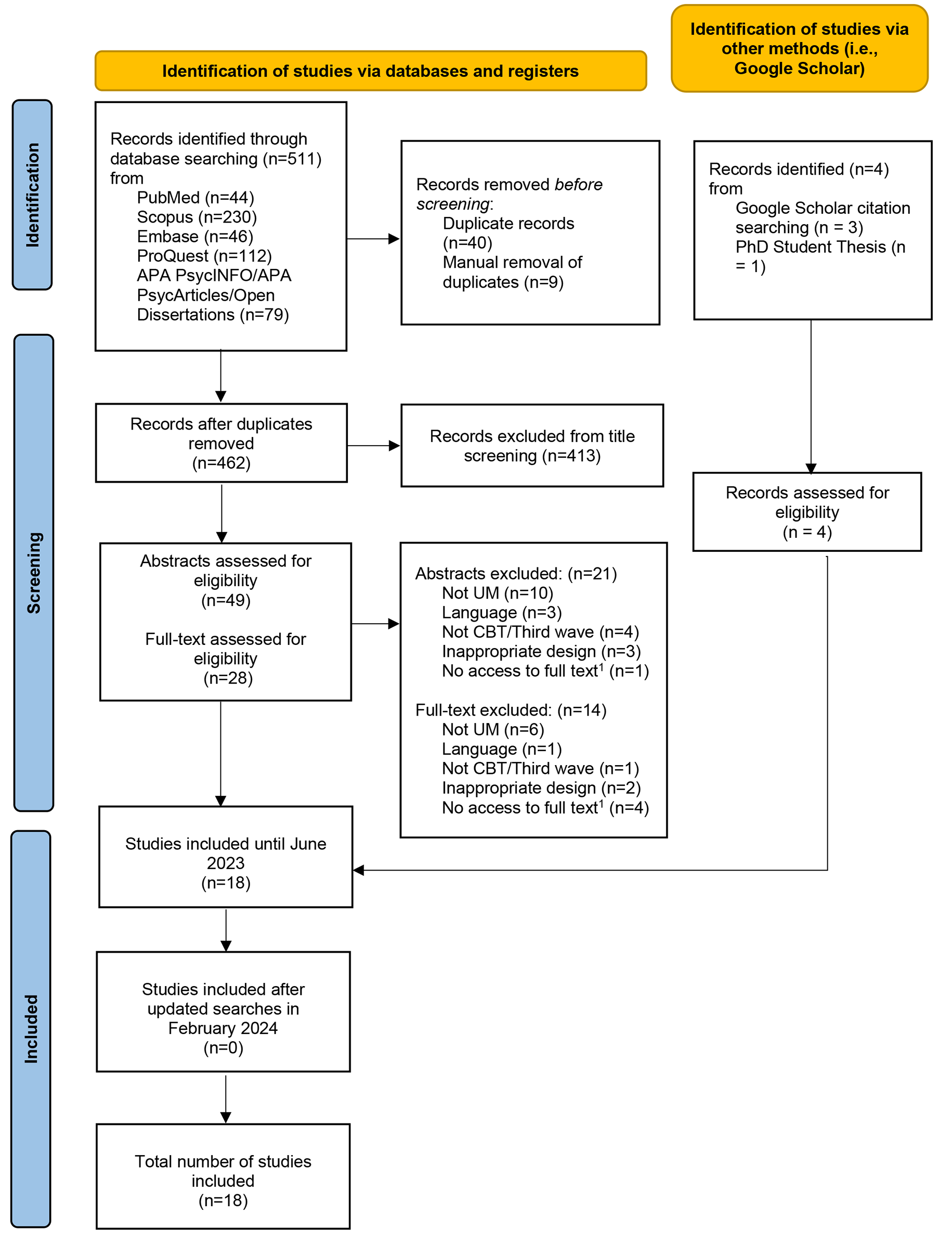
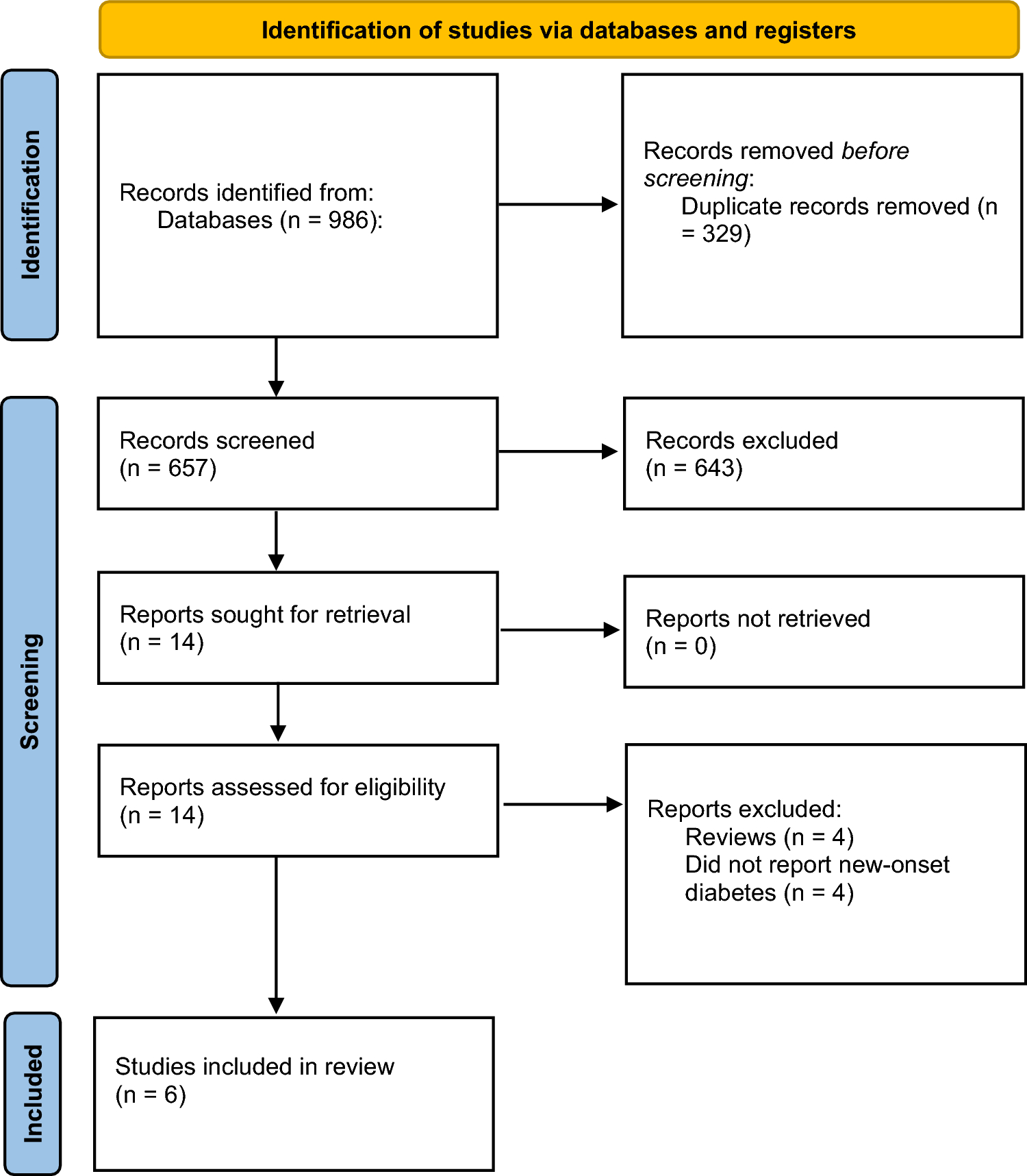
A strength of this review was the systematic search of the available literature across seven databases by two independent reviewers and quality of studies was assessed as high or moderate for all except one study. Studies from eighteen countries were included, collecting data from diverse settings. However, there is a risk of potential overlap in populations across studies from the same countries and using similar databases, especially among the Taiwanese studies, which should be taken into account when interpreting the weight of our findings. For studies investigating ADHD-related symptoms, there was wide variability in chosen assessment tools, leading to challenges in comparing the results between studies. Even though our meta-analysis aimed at combining quantitative data from studies that offered sufficient detail, the high heterogeneity across studies, (despite our attempts to explain the reasons behind it), made it challenging to generalize our findings reliably. Additionally, not all retrieved studies could be included in the meta-analysis due to the way data were analysed and presented, meaning some studies with large datasets were excluded from the quantitative synthesis. Although searches were comprehensive there is a small risk of publication bias, as smaller studies or ones with negative results may have not been published and so might have been missed from our database search, potentially causing an over-estimation of the studied effect. Pervasive developmental disorder not otherwise specified (PDD-NOS) was not included in our search criteria, which could be seen as a limitation. For studies investigating teacher ratings, there was no information on the training and experience of individual teachers in identifying ADHD symptoms or on how long they had known the child.
Clinical and research implications
Teacher ratings form an important part of ADHD assessments, and so it is important to understand the effect of relative age on their perception of what are normative or immature behaviours. Clinicians would benefit from collaborative involvement of parents and teachers in their assessments, whilst taking into account the possible differences in the relative age effect bias of these two informants. Despite the relative age effect being previously described in the literature, this has not translated into a change in clinical practice for diagnosis or medication prescribing, although a conclusion around the magnitude of the relative age effect is difficult to draw given the level of heterogeneity observed. It will be useful to incorporate this phenomenon in the clinical guidelines and training of healthcare professionals specialising in neurodevelopmental disorders as well as teachers to help them think critically about children’s symptoms during their assessments. Importantly, diagnosis of ADHD in relatively younger children is no more likely to decrease in persistence than diagnoses in relatively older children and so the relative age effect should not necessarily deter clinicians from diagnosing relatively younger children with ADHD [51]. Referrers and clinicians should consider the possibility that the relative age effect may be leading to a decreased likelihood of older children in the class being identified with ADHD symptoms [51]. Systematically considering contributing factors like relative immaturity as part of a child’s presentation is important to improve accuracy of ADHD diagnosis and subsequent appropriate treatment with medications.
Given the prevalence of ADHD [52], addressing the diagnostic challenges and accounting for biases becomes increasingly relevant. From a research perspective, a more standardised methodology (e.g. choice of measures) across future studies would allow for a more reliable quantitative analysis due to more comparable results, which was not possible in this work.
In terms of educational implications, studies investigating the effect of delaying school entry on children’s likelihood of being prescribed ADHD medication have found that held-back children were more likely to be treated for ADHD. As this work is crucial to informing educational policies, further research on the impact of flexible school entry would be valuable, as current evidence is limited.
Further research is necessary to replicate and extend the current limited findings on ASD, investigating if this effect is also present in other countries and healthcare settings.


留言 (0)