
記住我



This study utilized data from the UK Biobank (Application Number: 143,136), a large, ongoing prospective cohort study. Between 2006 and 2010, the UK Biobank collected a substantial dataset from more than 500,000 individuals aged 37 to 73 years across the UK. Through touchscreen questionnaires, physical examinations, and collection of biological samples, participants furnished sociodemographic, lifestyle, and health-related details. The UK Biobank also provides participants with health outcome information by establishing connections with diverse health-related records. Detailed data on the UK Biobank is available on the internet at http//www.ukbiobank.ac.uk, in addition to being accessible on published articles [17, 18].
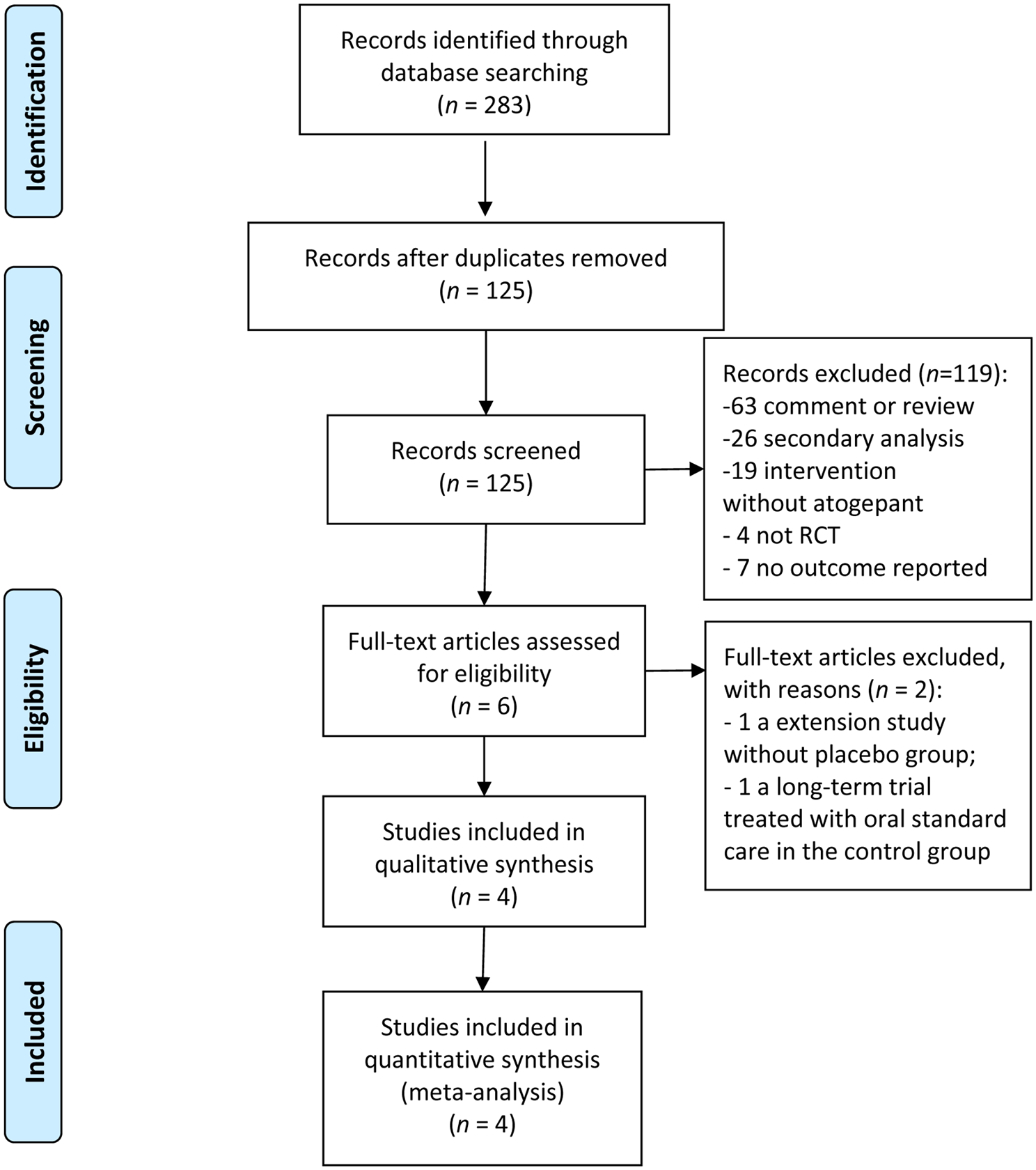
Initially, we excluded participants from our study who had incomplete data on lifestyle factors (including BMI, smoking status, alcohol consumption, physical activity, sleep pattern, sedentary time, and diet) and LE8 components. Subsequently, participants with missing sociodemographic and migraine-related covariates were also excluded. Furthermore, participants lost to follow-up and those with migraine at baseline were finally excluded. Ultimately, the analysis comprised a total of 332,895 participants (Fig. 1).
Fig. 1
Flowchart of the study. BMI = body mass index; LE8 = life’s essential 8
Approval for the UK Biobank was granted by the North West Research Ethics Committee under reference number 06/MRE08/65. All participants gave written informed consent prior to enrollment.
Healthy lifestyle scoresTo determine Healthy lifestyle scores, we chose seven modifiable well-established lifestyle factors, encompassing BMI, smoking status, alcohol consumption, physical activity, diet, sleep pattern and sedentary time. Further information of each lifestyle factor can be accessed in Table S1.
The calculation of Body Mass Index (BMI) involved dividing the weight of a person (measured in kilograms) by the square of their height (measured in meters). A BMI below 25 kg/m2 was generally considered to be ideal. Smoking status was classified into three categories: never smoked, former smoker, and current smoker, with never smoking being the ideal. Alcohol consumption was calculated by summing the intake of various alcoholic beverages, including wine (red, white, fortified), champagne, beer, cider, spirits, and other alcoholic drinks. In the United Kingdom, the recommended alcohol consumption for women was 0-≤14 g per day, while for men it was 0-≤28 g per day, which was considered to be ideal [13, 19, 20]. Physical activity was evaluated by self-reported measures of the weekly duration of moderate and vigorous physical activity. The attainment or surpassing of 150 min of moderate physical activity, 75 min of vigorous physical activity, or a cumulative total of 150 min of physical activity was defined as ideal [21]. Based on previous studies from UK Biobank [12, 22], we employed a modified dietary score (Table S2) that aligns with the Americanized Mediterranean dietary pattern endorsed by the AHA. The attainment of a score of 5 was deemed ideal in terms of the dietary score. A healthy sleep pattern (Table S3) was formulated by considering five sleep factors, assigning a score of 1 for low risk and 0 for any other condition, resulting in a cumulative score of 5. A total score of 4 or higher indicates the presence of a healthy sleep pattern [23]. The quantification of sedentary time involved the summation of daily durations dedicated to television watching and computer using, wherein an ideal threshold was established at less than 4 h in total [24].
Participants were given a score of 1 if they meet the ideal criteria for each lifestyle factor, and a score of 0 if they did not. The cumulative score for all lifestyle factors was then calculated to determine the Healthy lifestyle scores. Subsequently, Healthy lifestyle scores were classified as ideal (5 or more points), intermediate (3 or 4 points), or poor (0 to 2 points) Healthy lifestyle.
Life’s essential 8 scoresAccording to the AHA’s construct of cardiovascular health [14], LE8 scores were made up by eight component metrics, including diet, physical activity, nicotine exposure, sleep, BMI, blood lipids, blood glucose, and blood pressure.
Healthy lifestyle scores section provides an overview of the methodologies employed to BMI, diet, physical activity and smoking status. Nicotine exposure was ascertained by considering both the individual’s smoking status and their exposure to secondhand smoke. The evaluation of secondhand smoke exposure involved inquiring whether anyone in the participant’s household engages in smoking. Sleep duration was recorded by posing the question, “Approximately how many hours of sleep do you typically obtain within a 24-hour period?” Non-high-density lipoprotein (non-HDL) cholesterol, which is calculated by subtracting high-density lipoprotein (HDL) cholesterol from total cholesterol, was used as the primary indicator for blood lipids. Blood glucose levels were evaluated through the utilization of glycated hemoglobin (HbA1c) and consideration of diabetes history. The average of two consecutive measurements was used to determine the systolic and diastolic blood pressure. Furthermore, medication records were scrutinized to ascertain the utilization of cholesterol-lowering and blood pressure medications.
LE8 scores involved eight components, each ranging from 0 to 100. The overall LE8 scores were determined by averaging the scores of these components. As per the guidelines provided by the American Heart Association (AHA) [14], the overall LE8 scores were categorized into three groups: Low CVH (0–49), Moderate CVH (50–79), and High CVH (80–100). Table S4 contain additional comprehensive information on LE8.
Ascertainment of outcomeThe diagnosis of migraine was determined using data obtained from the Tenth Revision of the International Classification of Diseases (ICD10), specifically through hospital admissions and self-report. Migraine was defined by the ICD10, with the data field 41,270 code G43 and/or self-reported with the data field 20,002 code 1265. This study conducted a follow-up on participants who did not have migraine at baseline. The duration of follow-up was determined by measuring the time elapsed from the baseline assessment until the occurrence of migraine diagnosis, death, or the end of the follow-up period (October 31, 2022 for England, August 31, 2022 for Scotland, and May 31, 2022 for Wales), whichever occurred first.
Ascertainment of covariatesThe potential covariates in this study were obtained from questionnaires at baseline. Age, sex and Townsend Deprivation Index (determined by their postcode and indicating higher scores for more deprivation) that were known before arrival at the Assessment Centre. Ethnicity and education were classified as binary variables, with ethnicity categorized as White and Non-White (mixed, Asian or Asian British, black or black British, Chinese, and other), and education categorized as higher degree (college or university degree or other professional qualifications) and other degree (A levels, AS levels, O levels, GCSEs, NVQ or HND or HNC, and other). Average total household income was collected by asking ‘What is the average total income received by your household before tax?’ and was characterized as: £; less than 18 000, 18 000–30 999, 31 000–51 999, 52 000–100 000, greater than 100 000 and Unknown. In addition, a range of medical conditions including vascular/heart problems, cancer and other serious medical condition/disability were also evaluated.
Statistical analysisBaseline characteristics of all participants was using analysis of variance (ANOVA), Kruskal-Wallis test, and chi-square test. Continuous variables were expressed as mean ± standard deviation (SD) if they satisfied normal distribution, otherwise as median [interquartile range (IQR)]. Categorical variables were expressed as percentages (%).
The Cox proportional hazards model to evaluate the potential association between migraine, scores in Healthy lifestyle and LE8, and individual lifestyle factors. Proportional hazards testing was performed using Schoenfeld residuals to ensure the validity of the analysis. The data were stratified based on age (> 55 and < = 55), and three distinct models were constructed in the multivariable analysis. In the analysis, Model 1 was initially modified by taking into account sex and ethnicity. Subsequently, Model 2 was underwent additional adjustments for income, education, and Townsend deprivation index. Model 3 incorporated additional adjustments for baseline cardiovascular diseases, cancer, and other serious diseases. Collinearity between covariates was tested using the variance inflation factor (VIF), and all covariates were found to be acceptable (all VIF were < 5). For detailed results, please refer to Tables S5 and S6. To investigate the dose-response effects, restricted cubic splines were utilized for continuous variables. Additionally, the cumulative incidence of migraine during the follow-up period was computed for participants in Healthy lifestyle categories (poor, intermediate, ideal Healthy lifestyle) and LE8 categories (low, moderate, high CVH), employing Kaplan-Meier survival curves. In theory, the incidence of migraine would decrease if all participants adhered to the low-risk lifestyle. To estimate the population attributable fraction (PAF), assuming a causal relationship between lifestyle and migraine risk, the R package AF was utilized.
Stratified analyses and interactions were conducted to assess the impact of Healthy lifestyle categories (per category increment) and LE8 categories (per category increment) on the incidence of migraine using covariates. These covariates included age (< 55 years and ≥ 55 years), sex (female or male), ethnicity (white or non-white), Townsend deprivation index (quintiles 1, quintiles 2–4, quintile 5), education (higher education or lower than higher education), average household income (£; less than 18,000, 18,000–30,999, 31,000–51,999, 52,000–100,000, greater than 100,000, and unknown), baseline cardiovascular disease (yes or no), baseline cancer (yes or no), and baseline other serious diseases (yes or no).
To ensure the dependability of our results, we conducted three sensitivity analyses. Initially, we employed the chained equation algorithm to conduct multiple imputation for missing data in all exposure variables and covariates, thereby evaluating the influence of missing values. Secondly, for further sensitivity analysis, we excluded individuals who developed migraine within 2 years. Lastly, at the outset of the study, we excluded participants with other types of headaches to mitigate the potential for reverse causation.
The statistical analyses were conducted using R software (version 4.3.2, http://www.R-project.org). A two-tailed p-value below 0.05 was deemed statistically significant for evaluating disparities.
留言 (0)