Multiple endocrine neoplasia 2B is a rare autosomal dominant disease characterized by the presence of MTC, pheochromocytoma, and a peculiar face [2]. Approximately 95% of all individuals with MEN 2B have a pathological variant in the tyrosine kinase domain of RET proto-oncogene at codon 918 in exon 16, which substitutes a threonine for methionine [2]. The estimated incidence of MEN 2B was no fewer than 1.4 per million live births per year between 1991 and 2000 [9]. About 75% of patients with typical MEN 2B have a de novo germline pathological variants of RET [4, 5, 10]. Among patients without family history of MEN 2B, the mean age at diagnosis was 14.2 years (range, 1–31 years), and all the patients had complications with MTC at diagnosis, and 33% died from MTC [11]. Moreover, Bracuckhoff et al. reported that severe intestinal manifestations were predominantly observed in patients with early onset MTC. These findings reflect the difficulty in the timely diagnosis of the syndrome in patients harboring a de novo pathological variant of RET. The present case was also a sporadic case with phenotypically normal parents, and it required a long period to diagnose MEN 2B, which was complicated by MTC. The authors emphasize that MEN 2B is an important disease that should not be forgotten as an organic disease with constipation, abdominal distention, and megacolon. This may help clinicians pay attention to Marfan-like fatigue, a peculiar facial appearance with thickening of the lips, and mucosal neuromas of the lips and tongue.
The importance of the alimentary tract components of MEN 2B was reported by Carney et al. in 1976 [8]. The frequency of gastrointestinal symptoms or abnormalities were observed in 14 of 16 patients (88%), which include constipation in 10 patients, diarrhea in three, and megacolon in five. Brauckhoff et al. reported that 74% (14/19 cases) of sporadic MEN 2B patients had intestinal dysfunction (constipation and/or diarrhea) before MEN 2B diagnosis [11]. Recently, Nagaoka et al. reported four Japanese cases of MEN 2B in both children and adults. Three of the four patients had gastrointestinal manifestations, one of whom had intestinal malrotation and megacolon at age 14 years of age, and the other had chronic constipation and flatulence since infancy [12]. According to previous reports, gastrointestinal symptoms in patients with MEN 2B included constipation (73–79%) [5, 13, 14], diarrhea (29–62%) [13, 14], and flatulence (79%) [14]. Moreover, the onset of gastrointestinal symptoms occurred during infancy or early childhood in 73% of patients [13]. Gastrointestinal manifestations offer the most important window of opportunity for early detection of MEN 2B. In the present case, we suspect that constipation at the age of 6 years was caused by mild loss of intestinal tone, and abdominal bloating and constipation at the age of 14 years was the result of megacolon.
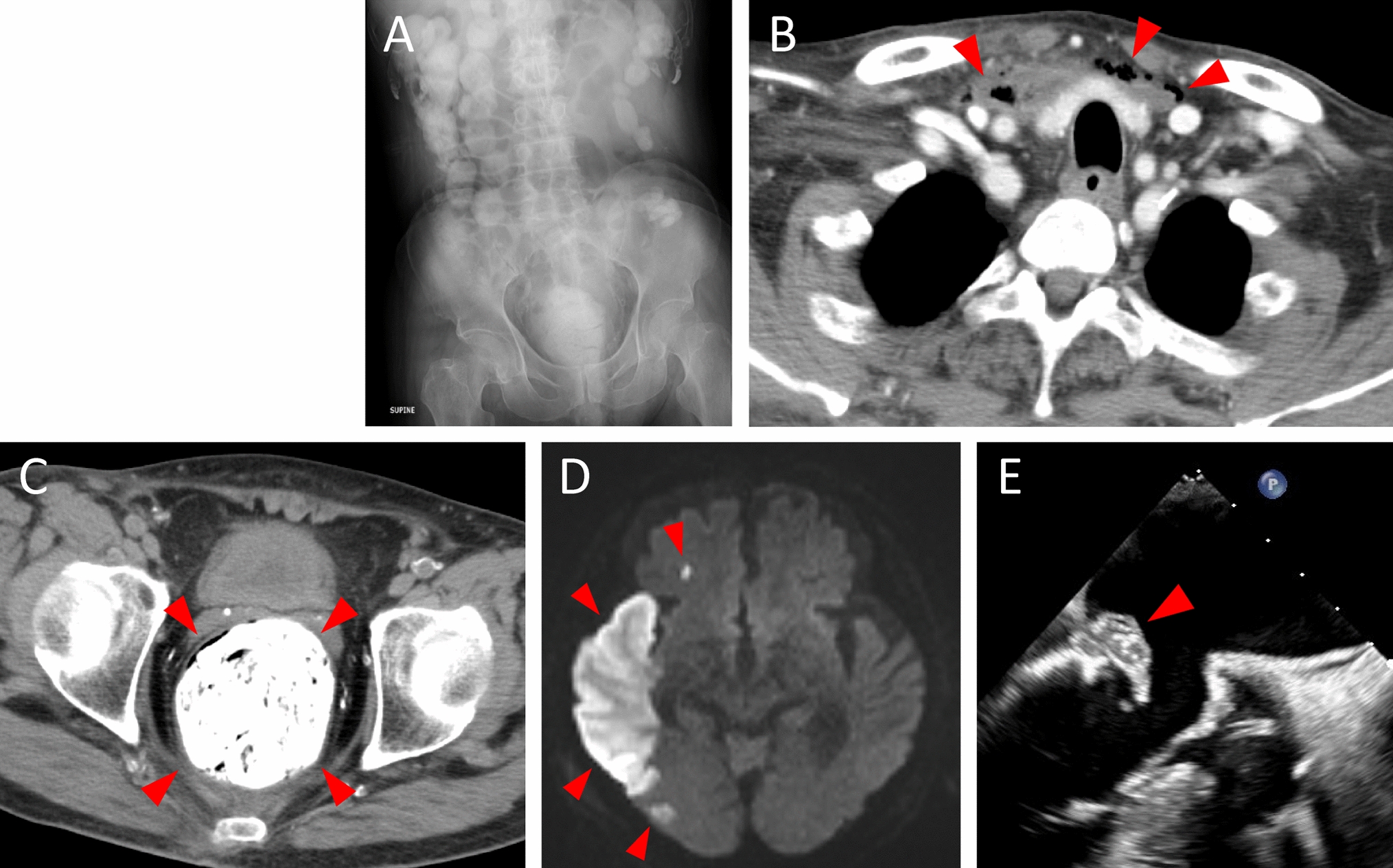
Based on the radiographic findings, the megacolon was reported among 29–63% cases and considered a typical feature of MEN 2B [8, 13, 15]. Gibbons et al. reported that megacolon was diagnosed during infancy to elderly age among MEN 2B patients [15]. The ganglioneuromatosis could lead to loss of bowel tone, distension, segmental dilation and, ultimately megacolon [15]. In patients with megacolon, it is crucial to differentiate it from Hirschsprung’s disease [15, 16]. Hirschsprung's disease is characterized by a transit disorder of intestinal content, delayed meconium excretion, abdominal distention, bilious vomiting, constipation, and intestinal dilatation (megacolon) at the proximal side, resulting from dysperistalsis and a lack of a recto-anal reflex caused by aganglionosis of the intestinal tract at the distal side [17]. Transanal rectal biopsy has been proposed as a valid procedure to differentiate Hirschsprung disease from MEN 2B by detecting the presence of ganglion cells in the rectum [13, 18, 19]. It is known that 10–25% of MEN 2A cases with the RET gene pathological variants in codons 609, 611, 618, or 620 co-occur with Hirschsprung disease [7, 20]. However, few cases are complicated by Hirschsprung’s disease in MEN 2B [13].
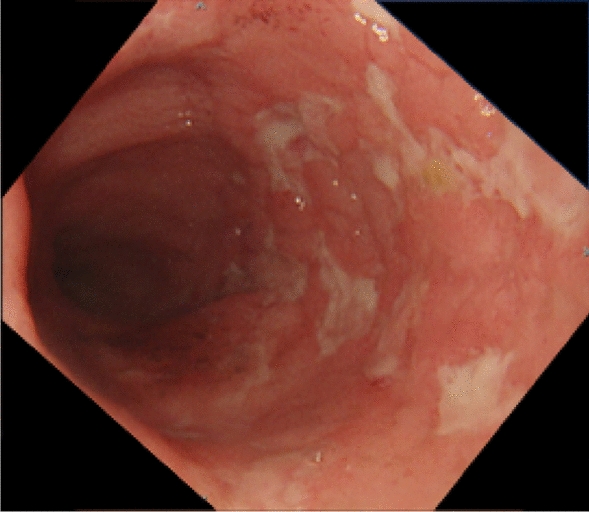
The pathophysiological feature of the intestinal tract in MEN 2B was known as transmural intestinal ganglioneuromatosis [8, 11, 13, 21]. Ganglioneuromas are characterized by an increased number of ganglion cells, supportive cells, and nerve fibers in all bowel wall layers. Ganglioneuromas can lead to the loss of bowel tone, distension, segmental dilation, and ultimately megacolon [22]. This phenomenon is described by RET overactivation in MEN 2B, which lead to a large increase in intrinsic nerve fibers in the myenteric and submucosal ganglia, including the rectum [18, 21]. Ganglioneuromatosis extends from the lips to the rectum based on autopsy or surgical tissues [8]. In the present case, the histological findings were compatible with ganglioneuromatosis in the resected transverse colon. A review of previous reports evaluating the intestinal histopathology of MEN 2B showed that a small number of patients were diagnosed as intestinal neuronal dysplasia (IND) type B [13, 23]. In Japan, IND is currently classified as a subgroup of ADHD [17]. Additionally, ADHD is a disease group characterized by symptoms and signs similar to those of Hirschsprung’s disease, despite the presence of ganglionic cells in the rectum. Intestinal neuronal dysplasia type B accounts for up to 95% of IND cases. In terms of pathology, malformation of the intestinal parasympathetic nervous system is present, and AChE staining shows evidence of submucosal giant ganglia, hyperganglionosis, ectopic ganglia, and the growth of AChE-positive nerve fibers [17]. Histopathological differences between ganglioneuromatosis-like hyperplasia and IND type B remains controversial [24]. A reliable diagnosis of MEN 2B based on genetic testing and high-quality pathological diagnosis should be considered in a large number of cases. Moreover, histopathological evaluation of both the rectum and dilated colon is useful for the appropriate diagnosis of MEN 2B.
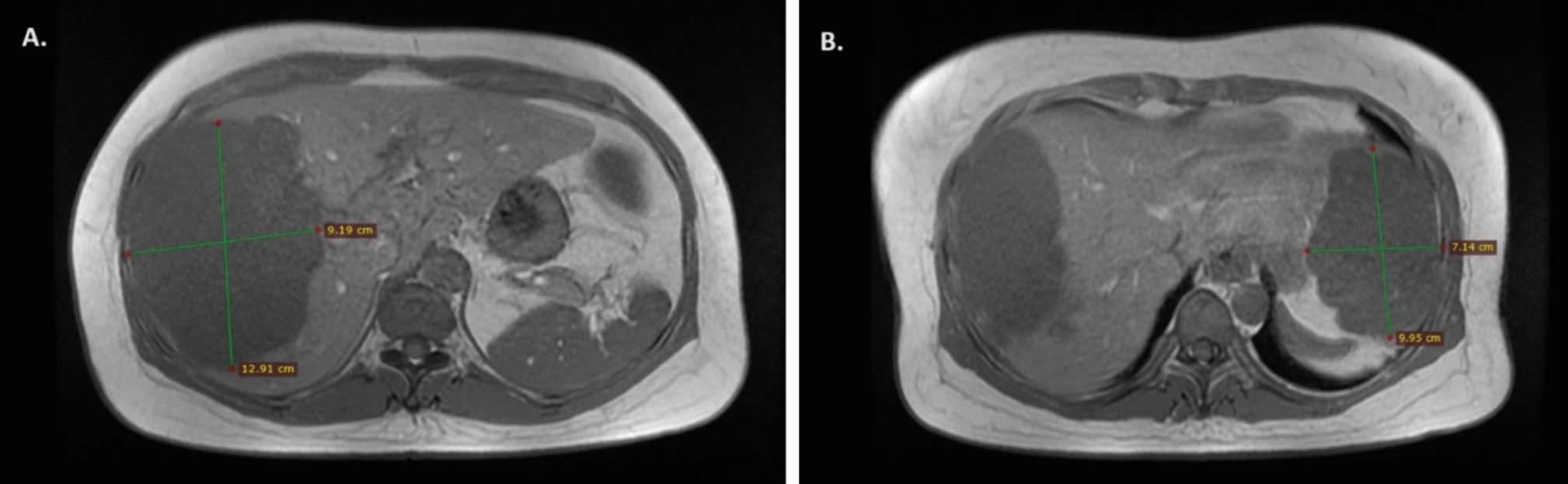
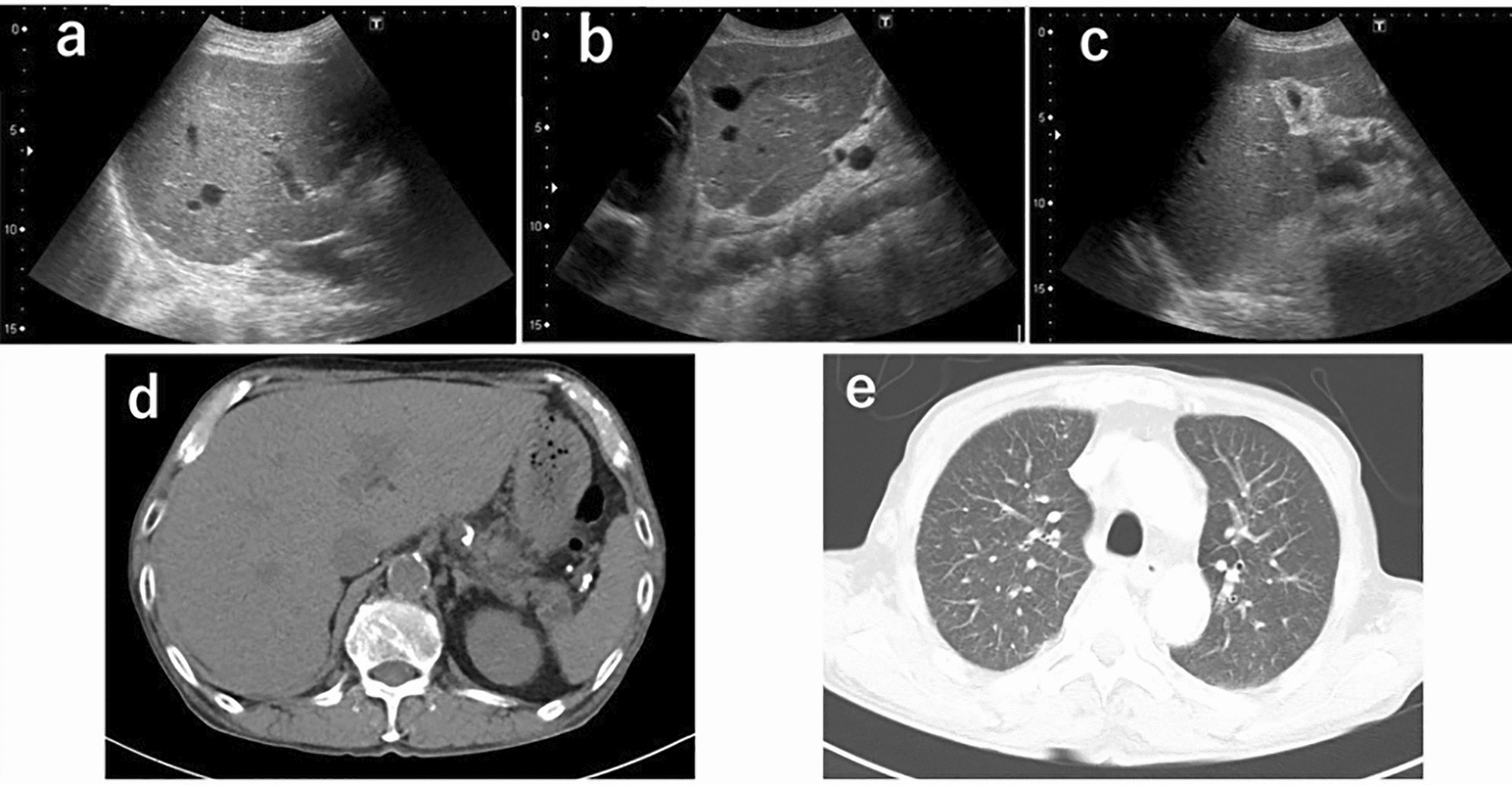
In MEN 2B patients with gastrointestinal symptoms, endocrinological screening and treatment are the first priority. Persistently elevated calcitonin levels induce diarrhea in patients with active MTC. Elevated secretion of catecholamines by pheochromocytomas may exacerbate reduced colonic tone, thereby leading to toxic megacolons [25]. After appropriate evaluation of endocrinopathies and neoplasms, most patients can manage their gastrointestinal symptoms conservatively with medication and dietary changes during childhood [7, 21]. However, gastrointestinal symptoms affect the patients’ quality of life [14]. More than one-third of patients with MEN 2B required gastrointestinal surgery, including colectomy for megacolon [7, 15, 21]. Surgery for megacolon is performed to reduce gastrointestinal symptoms and improve the quality of life. In children, some cases disappear symptoms after a single surgery. However, it is reported that patients who underwent colectomy in childhood needed re-operation in adulthood [7]. In the present case, the megacolon was exacerbated, and the dilated colon compressed the surrounding organs. Although the patient currently only has symptoms of flatulence and no symptoms of bowel obstruction, we are considering extended colon resection as a scheduled surgery, taking into account the invasiveness of the surgery and the possibility of re-operation in adulthood. Further evaluation of esophageal motility problems or evacuation disorders is required after colectomy [15]. To the best of our knowledge, this is the first report of a patient with MEN type 2B complicated by volvulus. A significantly dilated colon was suspected of occupying the abdominal cavity; thus, small intestinal volvulus was induced. Small intestinal volvulus is associated with the risk of intestinal ischemia and small intestinal resection.
In conclusion, we report the case of an adolescent with MEN 2B proceeding constipation and megacolon complicated by volvulus before the diagnosis of MEN 2B. Timely diagnosis may lead to appropriate treatment of MTC and improve mortality.


留言 (0)