
記住我
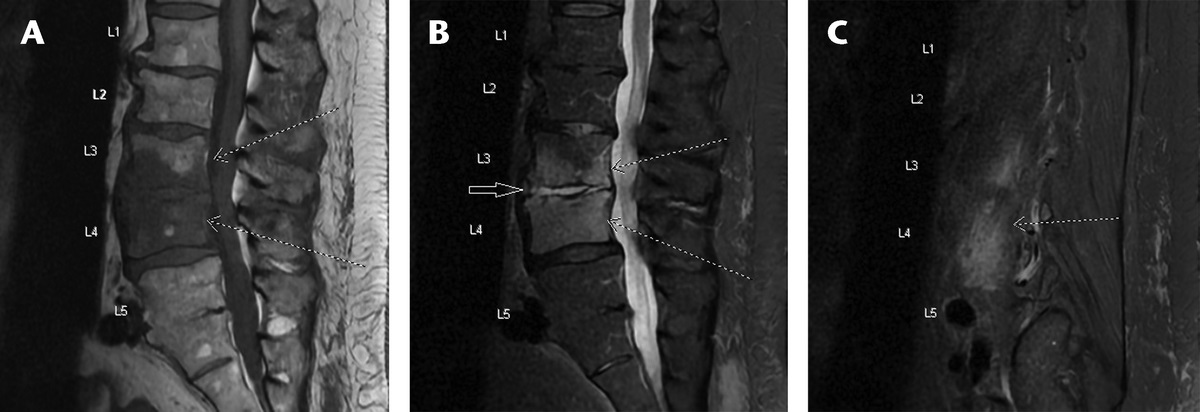

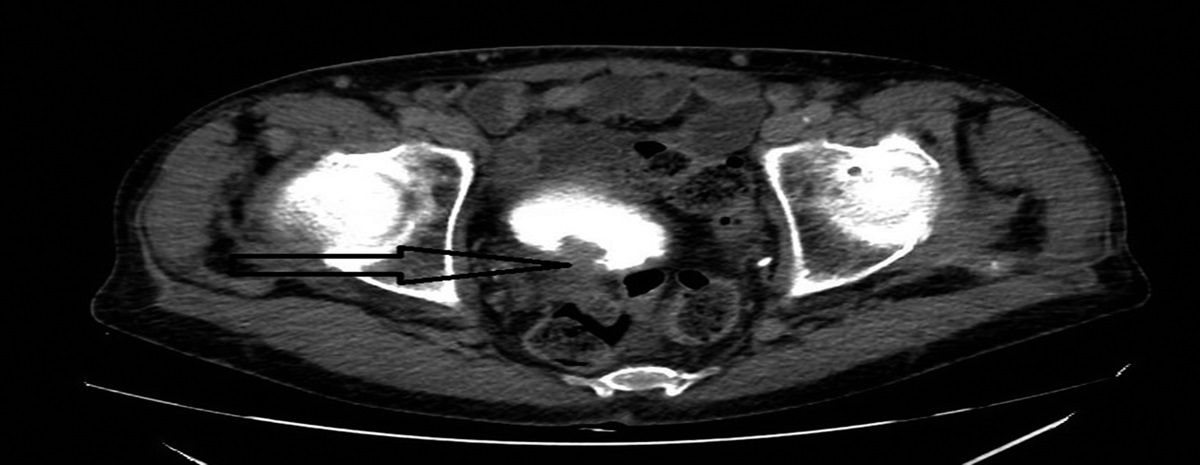
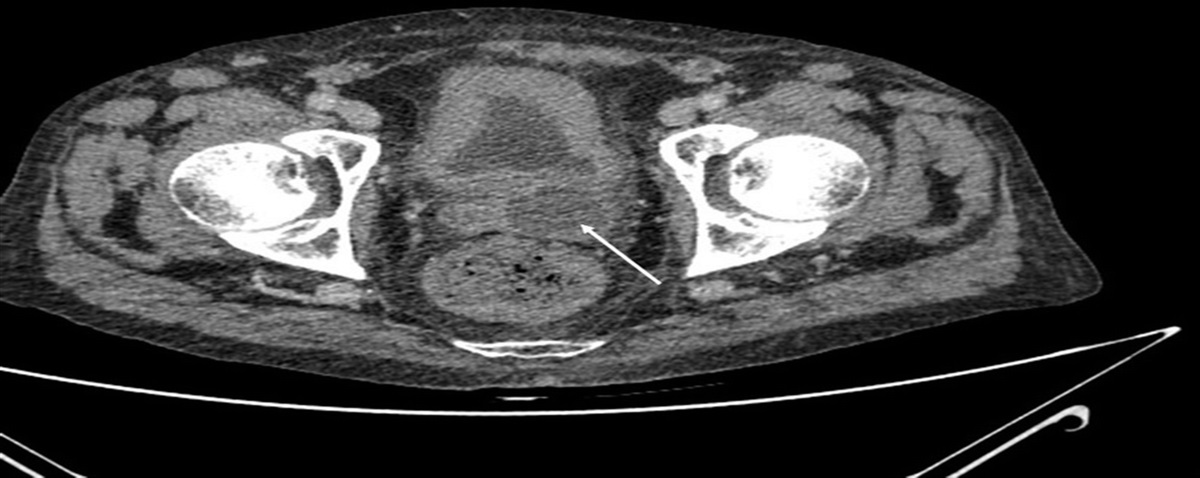
A 62-year-old man with hypertension and extensive smoking history presented with hematuria, urinary retention and 40-pound weight loss over 6 months. He worked as an apple farm manager in Western New York, where he cleaned barns occupied by nesting pigeons and had frequent contact with farm cats and dogs. He weighed 81.6 kg. Temperature was 36.6°C, pulse 61 beats/minute, blood pressure 98/53 mm mercury, respiratory rate 18 breaths/minute, oxygen saturation 98%, and urine output of >800 mL with placement of urethral catheter. Physical examination was remarkable for edentulous oropharynx, tanned skin with actinic keratoses. Laboratory results notable for leukocyte count 7.8 × 103/microliter, sodium 126 mEq/L, creatinine 0.5 mg/dL, and albumin 2.8 g/dL. Urinalysis showed large nitrite and leukocyte esterase, 21–40 bacteria, and 21–40 white blood cells/high powered field. Urine culture grew >100,00 cfu/mL Escherichia coli, and he was treated with ciprofloxacin. Three months later, hematuria recurred and computed tomography urography showed mucosal irregularity of posterior urinary bladder with pedunculated mass measuring 1.6 × 1.3 × 1.2 cm concerning for malignancy (Fig. 1).
 FIGURE 1:
FIGURE 1: Computed tomography urography demonstrating mass-like pedunculated filling defect on the posterior aspect of bladder.
During cystoscopy, a nodular, pedunculated tumor was resected from the right posterior bladder wall, and plaque-like thickened yellow mucosa of the left posterior bladder wall was biopsied. Histopathologic evaluation of both sites revealed sheets of histiocytes with granuloma formation and numerous 2–4 μm, round yeast-like cells with thick walls on H&E (hematoxylin and eosin) stain (Fig. 2A), equivocal budding pattern observed on GMS (Gomori methenamine silver) stain (Fig. 2B), and intracellular location within histiocytes confirmed with a CD68 immunohistochemical stain (Fig. 2C). Organism size and intracellular pseudo-halo appearance were suggestive of Histoplasma species; however, round, thick walls and inability to definitively characterize breadth of budding were concerning for Blastomyces. The biopsy specimens were not cultured as gross appearance intraoperatively was highly suggestive of neoplasm. Histopathology findings subsequently prompted infectious disease consultation.
 FIGURE 2:
FIGURE 2: A, Hematoxylin-eosin stain showing numerous thick walled intra-cytoplasmic spherical structures. B, Gomori-methenamine silver stain showing round yeast-like forms with equivocal budding pattern. C, CD68 immunohistochemical stain demonstrating intra-cytoplasmic location of round thick walled yeast-like organisms within histiocytes.
Additional investigations included negative urine Histoplasma galactomannan antigen (MiraVista Diagnostics), negative serum Histoplasma mycelial and yeast antibodies by complement fixation (ARUP Laboratories), as well as negative combined anti-Histoplasma IgG and IgM antibody serology by immune diffusion (ARUP Laboratories). Blastomyces antibody serology was positive by enzyme immunoassay (Mayo Clinic) and negative by immune diffusion (Quest Diagnostics).
An investigational multiplex polymerase chain reaction (PCR) assay of the formalin-fixed paraffin-embedded biopsy tissue was positive for H. capsulatum nucleic acids with a cycle threshold (Ct) value of 31 (strongly positive) and negative result for Coccidioides, Blastomyces, and Pneumocystis nucleic acids (MiraVista Diagnostics, assay validation in progress). This was useful in confirming a possible diagnosis of histoplasmosis in absence of culture data and conflicting findings on histopathologic examination and serologic assays.
Itraconazole was initiated with rapid improvement of symptoms, weight gain, and resolution of findings on repeat cystoscopy. The patient remains symptom free at 12 months post resection of possible Histoplasma-associated urothelial pseudotumor. Urine Histoplasma galactomannan antigen (MiraVista Diagnostics) and H. capsulatum serologies (ARUP Laboratories) remained negative during treatment and follow-up.
DISCUSSIONHistoplasma capsulatum is a dimorphic fungus, existing in mycelial form in the environment while transitioning into yeast form in temperatures at approximately 37°C. The mycelial form exists in culture and is characterized by septate hyphae bearing tuberculate macroconidia. Histoplasmosis can be found in many locations across the world but is especially common in the Ohio and Mississippi river basins of the United States, where it is endemic and pear-shaped microconidia are ubiquitous in soil, particularly in areas contaminated with bat or bird excrement.1 Infection occurs when Histoplasma microconidia are inhaled. Disseminated disease occurs in about 8% of patients with histoplasmosis,2 most often in those with impaired cellular immunity.3 Most patients present with systemic findings including fever, fatigue, and weight loss, accompanied by localizing findings such as cough, shortness of breath, lymphadenopathy, hepatomegaly, splenomegaly, abdominal pain, joint pain, headache, neck stiffness, and memory impairment.4
The gold standard for diagnosis of suspected histoplasmosis entails demonstration of characteristic yeasts on histopathologic examination of infected tissue, typically 2–5 μm in diameter exhibiting narrow based budding. Alternatively, diagnosis can be made through demonstration of typical growth in culture of clinical specimens, appearing as a white to light tan mold on Sabouraud's dextrose agar after 2–6 weeks of incubation at 25°C, followed by direct identification via nucleic acid testing, or mass spectrometry.3 Antigen-based tests and serologic testing have evolved to offer an attractive alternative for diagnosing histoplasmosis, as cultures require strict methodology and may be slow growing. Urine Histoplasma galactomannan assays can near sensitivity of 95% in settings of high microbiologic burden, as in disseminated histoplasmosis with HIV/AIDS.5 Use of urine galactomannan testing is less reliable in subacute histoplasmosis, only approaching a sensitivity of 30% in some large multicenter studies,6 and offering limited utility in chronic, anatomically sequestered disease such as mediastinal granuloma and fibrosing mediastinitis.5 Urine concentration and potential need for ultrafiltration may affect low-positive urine antigen results.7,8 Testing for Histoplasma antibodies by EIA, complement fixation, or immune diffusion assays is widely available, but subject to significant interassay variability.1 While serologic testing can be generally helpful in ruling out exposure, concomitant antigen or tissue based testing is required to evaluate for active disease.5 Negative serology and urine Histoplasma antigen created diagnostic uncertainty in this presentation of possible genitourinary histoplasmosis, with diagnosis further complicated by lack of culture data, absence of expected budding pattern, and characteristic cell wall structure on histopathologic examination.
The development and widespread availability of molecular methods for detection of Histoplasma nucleic acids in clinical specimens have been hampered by inconsistent performance characteristics,9 although the sensitivity and specificity of some PCR based assays have been reported to approach 86% and 100%, respectively.10 A recent report by Alanio and coauthors describes a promising real-time quantitative PCR (RT-q PCR) technique which yielded positive results of at least one blood, respiratory, or biopsy specimen in 43 of 44 patients (97.7% sensitivity) with culture-based or histopathologically proven histoplasmosis, with particularly high rates of testing concordance noted in settings of disseminated disease affecting immunocompromised hosts.11 An investigational pulmonary fungal pathogen multiplex PCR panel (MiraVista Diagnostics) was useful in diagnosis of the current case. The research panel targets internal transcribed spacer (ITS) sequences to detect and differentiate H. capsulatum, H. dubosii, Blastomyces dermatiditis and B. gilchristii, Coccidioides immitis and C. posadasii species, and mitochondrial ribosomal RNA genes to detect Pneumocystis jirovecii and Pneumocystis canis in multiple sample types including bronchoalveolar lavage, cerebrospinal fluid, sputum, and formalin-fixed paraffin-embedded tissue.
Literature review suggests that difficulties encountered in diagnostics for the current report are not surprising. Disseminated histoplasmosis can involve any organ,3 however, although the largest disseminated histoplasmosis autopsy series12 found some level of genitourinary involvement was incidentally noted in 17–40% of examined cases, symptomatic genitourinary histoplasmosis remains rare, as supported by our own literature search using keywords “genitourinary histoplasmosis”, “immunocompromised”, and “immunocompetent” in PubMed and GoogleScholar. A recent extensive review13 of published genitourinary histoplasmosis cases highlights relative infrequency of urinary bladder involvement, only present in 6 of 131 cases reviewed. A higher predilection toward upper tract infection, with renal parenchymal lesions or diffuse nephritis, and extra-urinary disease involving prostate, testes, and external genitalia was observed in 81 of 131 cases reviewed.13 Despite anatomically proximal location within the urinary tract and high inoculum of suggestive microorganisms on pathologic examination of excised tissue, confirmatory diagnosis with traditional serologic and urine antigen based methods was elusive in the current case. Only 2 additional case reports of antigen-negative histoplasmosis of the urinary bladder were identified in the literature.12,14
The current report is also notable for neoplasm-like pedunculated growth with intravesicular protrusion of pseudotumor. Fifteen additional cases1,7,15–27 of histoplasmosis mimicking neoplastic growth in various organ systems were identified. While 2 cases note mass-like phenomenon with testicular and epididymal involvement,13 no additional cases of Histoplasma-related pseudotumor of the urinary bladder have been published, to our knowledge. Histopathological tissue examination was diagnostic in majority of published pseudotumor cases (Table 1), with culture-based methods of detection, serology, and urine antigen testing performing inconsistently, similar to current report. Demonstration of yeast-like cells suggestive of Histoplasma in resected bladder tissue prompted a possible diagnosis in the current case; however, antigen could not be detected in the urine most likely due to localized involvement of the interior of the mass, rather than widespread involvement of reticuloendothelial tissues, characteristic of systemic disseminated histoplasmosis. Identification using an investigational multiplex PCR assay for Histoplasma nucleic acids on formalin fixed tissue samples was particularly useful.
TABLE 1 - Tabular Review of the 16 Published Cases of Pseudotumor Due to Histoplasmosis (Including Current Case) and Results of Diagnostic Testing Location of Histoplasma-Associated Mass Gastrointestinal GenitourinaryHistoplasma-associated pseudotumor cases as reported in literature review; vertical columns display diagnostic characteristics of each case, separated by location of the mass, as cited in each case report, listed horizontally in the header row.
留言 (0)