
記住我

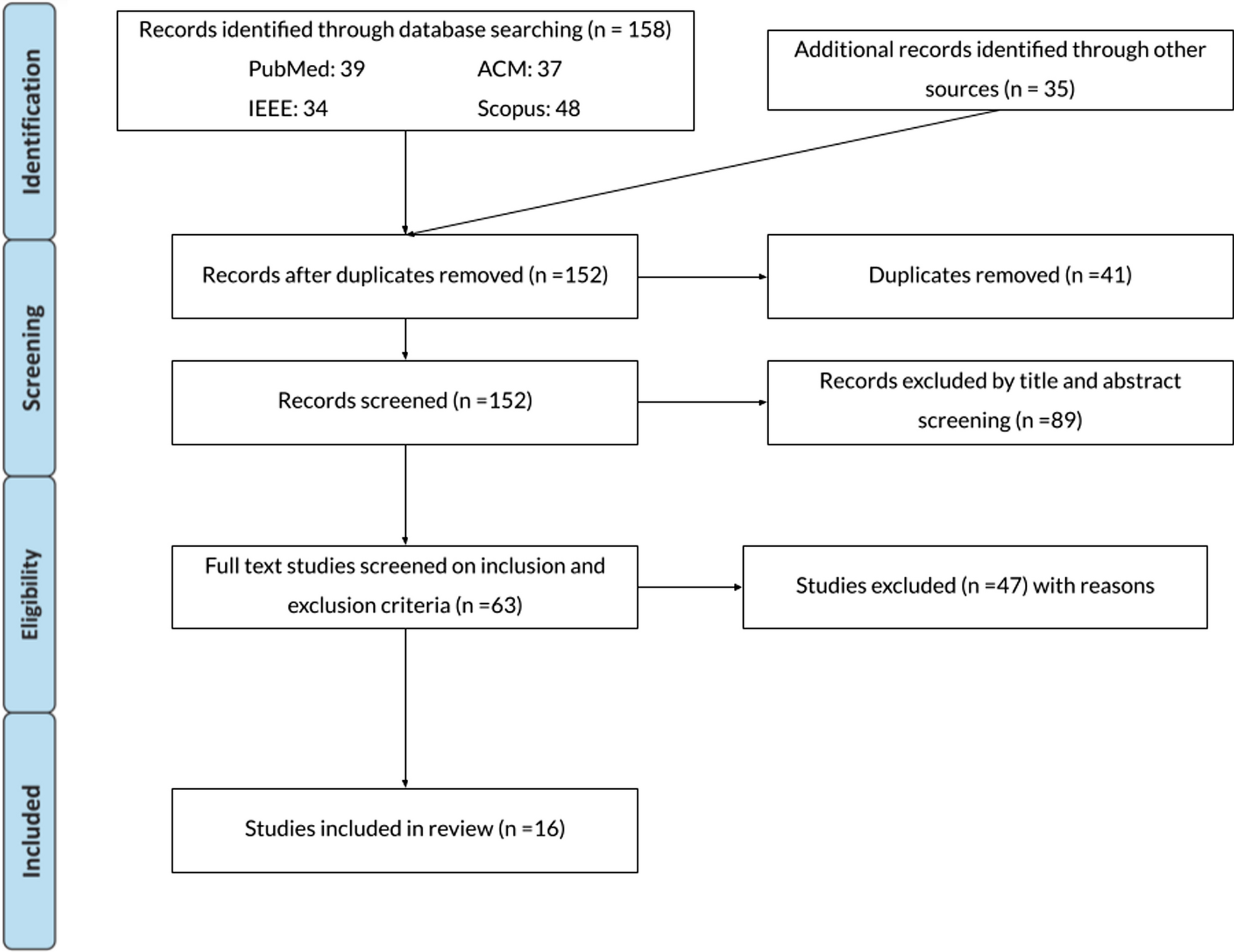







The search yielded 309 articles from Scopus (n = 181), PubMed (n = 117), and IEEE Xplore (n = 11). After removing 96 duplicates, a total of 213 articles were screened by title and abstract and 195 were subsequently excluded, showing an almost perfect level of agreement between two authors M.C. and E.L. (Cohen’s Kappa coefficient = 0.914 [27]). The full text of 18 articles was evaluated for eligibility and 5 articles were eventually excluded because they did not meet the inclusion criteria for full text described in the Methods section (Cohen’s Kappa = 1.0 between MC and EL). Thus, the final synthesis included a total of 13 records (Fig. 1).
Fig. 1
PRISMA flow diagram of scoping review results
A comprehensive summary of key information extracted from the studies, including pathology, time since injury, sample size, population age, participants’ prior experience with VR, research aims, and study type and design is provided in Table 1. The analysis of these results reveals a notable trend: the use of immersive VR for upper-limb rehabilitation has emerged relatively recently, with the oldest paper included in this review published in 2016.
Table 1 Participants, study aims and designKey characteristics of selected studiesType of diseasesGiven the global prevalence of stroke [28], stroke survivors have naturally emerged as primary candidates for immersive VR-based rehabilitation programs (Fig. 2). Symptoms of stroke vary depending on the damaged brain area, but in more than 80% of the cases, patients have upper limb impairments [29], including weakness or paralysis, decreased range of motion, spasticity, coordination problems, sensory alteration, and impaired fine motor skills [30]. All the analyzed studies focusing on stroke survivors aimed at improving their upper-limb motor functions (n = 8) [30,31,32,33,34,35,36,37]. Moreover, stroke conditions can be classified based on the time elapsed from the lesion between the acute stage (1–7 days), subacute stage (≤ 6 months) and chronic stage (> 6 months) [38]. We found that the studies selected in this scoping review were almost equally distributed among two groups, with three focusing on subacute patients [30, 31, 37] and the other five focusing on chronic patients [32,33,34,35,36]. The presence of studies that used immersive VR in acute and subacute phases of stroke rehabilitation reflects the clinical priority given to interventions during these vital early stages, emphasizing the importance of acting as soon as possible [8, 11].
Fig. 2
Studies taxonomy structured per pathologies and tasks
Other two types of diseases for which studies using immersive VR for upper-limb rehabilitations has been used are conditions associated with pain (n = 4) [39,40,41,42], such as phantom limb pain and complex regional pain syndromes, and multiple sclerosis (n = 1) [43].
Type of virtual tasksThe studies identified in this scoping review can be further categorized based on the virtual rehabilitation tasks performed by the participants (Table 2). Three main types of tasks were used: mirror therapy, motor tasks, and motor imagery.
Table 2 Experimental protocolsMirror therapy is a rehabilitation technique that traditionally uses a mirror to create a visual illusion of normal limb movement [44]. By reflecting the unaffected limb, it makes the brain perceive that the affected limb is functioning properly. VR mirror therapy is a variant of traditional mirror therapy in which patients see a virtual representation of their affected limb moving in synchrony with the actual movement of the unaffected limb [30, 35, 39, 40]. By having the illusion of the correct functioning of the affected limb, the brain receives positive visual feedback that can help alleviate pain, reduce swelling, and improve motor function and coordination. Mirror therapy takes advantage of the brain's neuroplasticity and promotes the rewiring of neural pathways and the reintegration of sensory and motor functions [41].
Motor rehabilitation tasks aim to improve motor control, coordination, and functional abilities by actively engaging the affected limb in goal-directed actions. In the selected studies, motor tasks involved using the affected limb to reach and grasp objects freely moving in the virtual environment [31, 42], interacting with a virtual kitchen [37, 41], manipulating objects [37], or other arm movements (e.g., wrist or fingers extension) [32,33,34, 43].
Another adopted approach was motor imagery [36]. Motor imagery involves mental rehearsal or imagination of specific movements without physically executing them. It is a cognitive technique often employed in stroke rehabilitation to promote motor recovery [45]. Patients imagine performing specific actions with their affected limb and the imagined movements are translated into motor commands from brain signals, usually recorded with electroencephalography (EEG) [46, 47]. In the study selected in this review, the participants were asked to row a boat by imagining moving either the left or the right hand [36].
Prior VR experienceWe found that any of the included studies contained information regarding participants' prior experience with VR. This gap is likely due to the relatively recent emergence of immersive VR for rehabilitation purposes. Consequently, for the authors, it is improbable to encounter participants who have previously been exposed to this paradigm.
Type of clinical assessmentThe selected studies included in our review show a considerable diversity in the implemented clinical assessments and outcome measures (Table 2). Among the studies on stroke patients, the most utilized assessment was the Fugl-Meyer Assessment (FMA) [48] or Fugl-Meyer Assessment-Upper Extremity (FMA-UE) [22], employed in seven out of eight studies [30,31,32,33, 35,36,37]. In addition, the Action Research Arm Test [26] was used in four out of eight studies [32,33,34,35]. Regarding the studies on phantom limb pain and complex regional pain syndrome, the most prevalent assessment was the Short-Form McGill Pain Questionnaire [49], which, along with its Japanese version [50], was used in three out of four studies [40,41,42].
Characteristics of studies on stroke survivorsAmong the studies in acute and subacute stroke patients, rehabilitation tasks are quite balanced (Fig. 2). Specifically, mirror therapy was used in one study [30], and motor tasks in two studies [31, 37]. Conversely, the studies in chronic patients mainly used motor tasks (n = 3) [32,33,34] and less, mirror therapy (n = 1) [35] and motor imagery (n = 1) [36].
In terms of homogeneity regarding clinical and demographic characteristics within subgroups, the three studies within the acute plus subacute stroke group focusing on motor tasks exhibit similar age ranges (Table 1): Heinrich et al. [30] reported participants’ ages ranging from 51 to 75 with a mean of 62 years, the single subject in the case study by Park et al. [31] was 56 years old, and Huang et al. 2018 [37] reported participants’ ages ranging from 44 to 79 years with a mean age of 69 years. The time since injury reported was similar for two studies: Heinrich et al. [30] (mean: 2.04 months; std: 1.87), and Huang et al. [37] (mean: 2.19 months; std: 1.13), while it cannot be compared as it was not reported by Park et al. [31]. The three studies on chronic stroke patients in the motor task subgroup show comparable clinical profiles in terms of time since injury: Erhardsson et al. [32] (mean: 2.51 years; std: 1.96), Marin Pardo et al. [33] (mean: 3.17 years; std: 1.03), and Lee et al. 2020 [34] (range: 3 years; std: 5.16). Furthermore, the age profiles are consistent between Erhardsson et al. [32] (range: 48–74 years; mean: 60.6) and Marin Pardo et al. [33] (range: 42–66 years; mean: 56.3). Only Lee et al. [34] have a population with a wider age range, starting from a lower minimum (range: 19–70 years; mean: 40.2).
As regards, instead, the comparison between studies in acute plus sub-acute and chronic stroke patients, there are some differences including the duration of a single session and the total number of sessions conducted (Table 2). For studies with participants in the sub-acute post-stroke stage [30, 31, 37], who are more sensitive to the intensity and duration of exercises because of their fragile condition, the average session duration was 13 ± 6 (mean ± std) minutes, and the average number of sessions was 14 ± 6. In contrast, in the studies involving chronic stroke patients [32,33,34,35,36], longer experimental sessions were performed, lasting 40 ± 17 min on average. In this case, the total number of sessions was lower, 11 ± 4 sessions on average. These findings suggest that the duration and repetition of the experimental protocol may vary based on the stroke phase, resulting in personalized approaches tailored to individual patient’s conditions and needs. However, it is important to note that the lack of studie
留言 (0)