
記住我








This work may not be copied, distributed, displayed, published, reproduced, transmitted, modified, posted, sold, licensed, or used for commercial purposes. By downloading this file, you are agreeing to the publisher’s Terms & Conditions.
 Abstract
Abstract
Objective: This study examined the effects of a multicomponent intervention program on cognitive function in community-dwelling older adults with mild cognitive impairment (MCI) and subjective cognitive decline (SCD).
Methods: This was a 2-arm, randomized controlled trial in which a multicomponent intervention was applied. Participants were recruited from June 2020 to August 2020, randomization and intervention began in August 2020, and the entire program ended in January 2021. It included cognitive training (mnemonic strategy training) and lifestyle guidance (diet, sleep, and exercise guidance) for 7 weeks. A total of 123 Chinese community-dwelling older adults experiencing MCI or SCD were randomly divided into a multicomponent intervention group (n = 62) and a health education group (n = 61). The global cognitive function was measured using the Mini-Mental State Examination (MMSE). The cognitive domains outcomes included memory functions measured using the immediate and delayed tests of the Auditory Verbal Learning Test (AVLT) and Logical Memory Test (LMT), and executive function and attention measured using the Digital Symbol Substitution Test (DSST) and Digit Span Test (DST). Data were collected at baseline and postintervention.
Results: For cognitive outcome, the results of linear mixed-effect model showed significant time í group effects in the MMSE (Cohen d =0.63 [95% CI, 0.27 to 1.00], F = 10.25, P = .002). This study found significant time í group effects in AVLT-immediate (Cohen d = 0.47 [95% CI, 0.11 to 0.83], F = 8.18, P = .005), AVLT delayed (Cohen d = 0.45 [95% CI, 0.10 to 0.81], F = 4.59, P = .034), LMT-delayed (Cohen d = 0.71 [95% CI, 0.34 to 1.07], F = 4.59, P = .034), DSST (Cohen d = 0.27 [95% CI, −0.08 to 0.63], F = 4.83, P = .030), and DST (Cohen d =0.69 [95% CI, 0.33 to 1.05], F = 8.58, P = .004).
Conclusions and Implications: The results support the feasibility and effectiveness of the multicomponent intervention program in improving cognitive function in community dwelling older adults at risk of dementia. The high adherence of this program shows its potential for promotion in the community and supports a larger and longer trial.
Trial Registration: Chinese Clinical Trial Registry (ChiCTR2200061420).
J Clin Psychiatry 2024;85(2):23m15112
Author affiliations are listed at the end of this article.
According to the World Health Organization, there are approximately 55 million dementia patients globally, and this number is estimated to rise to 78 million by 2030; the global societal cost of dementia is expected to increase to US $2.8 trillion by 2030.1 Additionally, family members of patients with dementia face huge physical and psychological burdens.2 China’s population is aging significantly faster than in other low and middle-income countries.3 The number of patients with dementia in China is approximately 10 million, ranking the highest worldwide.4
With approximately 60% of patients diagnosed with dementia currently living in communities5 with a large population, inadequate management of patients with dementia or mild cognitive impairment (MCI) at the community level increases the burden of cognitive impairment.6 The community, as the first point of contact for patients with dementia,7 needs to strengthen the management of dementia and its preceding stages and develop community-based intervention programs for older adults without dementia to delay or even avoid dementia.
Older adults with MCI and subjective cognitive decline (SCD) are at greater risk of developing dementia than older adults with normal cognition.8–10 The natural pathogenesis of Alzheimer disease (AD) begins with SCD, which progresses to MCI at a rate of 6.67% per year; approximately 50% of patients with MCI will develop AD within 5 years.11 Interventions for at-risk older adults in the early stages before dementia develops, such as MCI or SCD, can effectively delay or even prevent the onset of dementia.12,13
One such intervention is a widely used form of cognitive training based on mnemonic strategies, which has demonstrated good results in improving cognitive function for individuals with MCI and SCD.14–17 Mnemonic strategies can be widely conceptualized as cognitive methods that contribute to the organization and association of new information, thus increasing the depth of processing.18 Mnemonic-strategy interventions usually include teaching participants about brain structure, how memory functions, and training memory strategies and guiding their application in everyday life.19
Multidomain lifestyle interventions have been shown to be effective in preventing dementia.20,21 In general, cognitive impairment is complex and multifactorial, and older adults with cognitive impairment have multidimensional influences, such as physical activity,22,23 lifestyle factors such as diet24,25 and sleep,26,27 and social interaction.28,29 Therefore, individuals with cognitive impairment require multicomponent interventions to obtain optimal prevention. A Finnish intervention study on the prevention of cognitive impairment and disability (FINGER) is the first large-scale multidomain intervention study, using diet, exercise, and cognitive training to prevent cognitive decline and dementia in at risk older adults,30 which suggests that a multicomponent intervention can be used to improve cognitive function in people at high risk of dementia.
Therefore, multicomponent interventions may be more effective in improving cognitive function and preventing dementia in older adults at risk of dementia. This study combined and implemented mnemonic strategy–based cognitive training with a multidomain lifestyle intervention to explore whether there would be an improvement in cognitive function and generalizability of the intervention to older adults in the community.
There are few studies on multicomponent interventions for community-dwelling older adults at risk of dementia, particularly in China. Therefore, we conducted a randomized controlled trial to understand the effectiveness of a 7-week group-based multicomponent intervention program, which includes mnemonic strategy training and multidomain lifestyle guidance, on improving cognitive function in community dwelling older adults at risk of dementia. The cognitive domains addressed included global cognitive function (memory, executive function, and attention). Additionally, attendance of the participants during the intervention was recorded.
METHODS Study DesignThis study was a single-blind, 2-arm, randomized controlled trial of a multicomponent intervention program with community-dwelling older adults. Older adults who attended a previous cognitive impairment screening program in Minhang District, Shanghai, in August 2019 were invited to participate in this study.31 Participants at risk of dementia were randomly assigned to the intervention or control group using a 1:1 ratio. All assessors were blinded to allocation and were not involved in the intervention activities. The intervention was carried out in small groups to ensure intervention effects. Participants in the intervention group were divided into 3 groups to participate in the intervention sequentially. We tested the effectiveness of the intervention protocol after the intervention. This study was approved by the Ethics Review Committee of Fudan University School of Public Health (IRB#2020-07-0840) and was registered with the Chinese Clinical Trial Registry (ChiCTR2200061420). Participants who agreed to participate in the study provided written informed consent before participating in the program.
ParticipantsCommunity-dwelling older adults with MCI or SCD were recruited. The initial inclusion criteria for all participants were as follows: (1) aged ≥55 years, (2) primary school education or above, (3) community dwelling, and (4) had subjective memory complaints. Inclusion criteria for participants with MCI32 were as follows: (1) subjective memory complaints, preferably confirmed by an informant; (2) Montreal Cognitive Assessment Scale Basic (MoCA-B)33 scores ≤19, 22, or 24 for participants who had primary school, middle school, or higher education, respectively, and Mini Mental State Examination (MMSE)34 scores ≥23; (3) overall intact activities of daily living; (4) without dementia; and (5) without other medical explanations for the cognitive impairment. Inclusion criteria for participants with SCD were as follows: (1) subjective memory complaints, (2) no objective cognitive impairment as measured by the MoCA-B and MMSE, and (3) overall intact activities of daily living.
The exclusion criteria were as follows: (1) cognitive impairment caused by other diseases (including but not limited to cerebrovascular disease, central nervous system infection, Parkinson disease, metabolic encephalopathy, folic acid and vitamin B12 deficiency, and hypothyroidism); (2) nervous system diseases (such as stroke, Parkinson disease, and epilepsy); (3) mental disorders included in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; (4) serious diseases of the heart, lung, liver, kidney, or hematopoietic system; (5) participated in any other similar cognitive intervention within 30 days of the study; and (6) other reasons for not completing the study.
InterventionsThe control group received a 7-week routine health education program. The health education program was carried out with health education lectures that included protection in daily life for older adults at risk of dementia: prevention of self-harm, prevention of falls, prevention of accidents, prevention of unsafe medications, prevention of wandering, and prevention of poor lifestyle habits, as well as health education for family members of older adults at risk of dementia, including how to make older adults feel close and connected during caregiving, avoiding exposure to dangerous objects, and taking older adults for regular memory checkups. There was also preventive content on dementia prevention, including its causes as well as its precursors. The lectures were given once to the older adults and once to their family members, and there was no homework or other interaction with the control group other than the lectures.
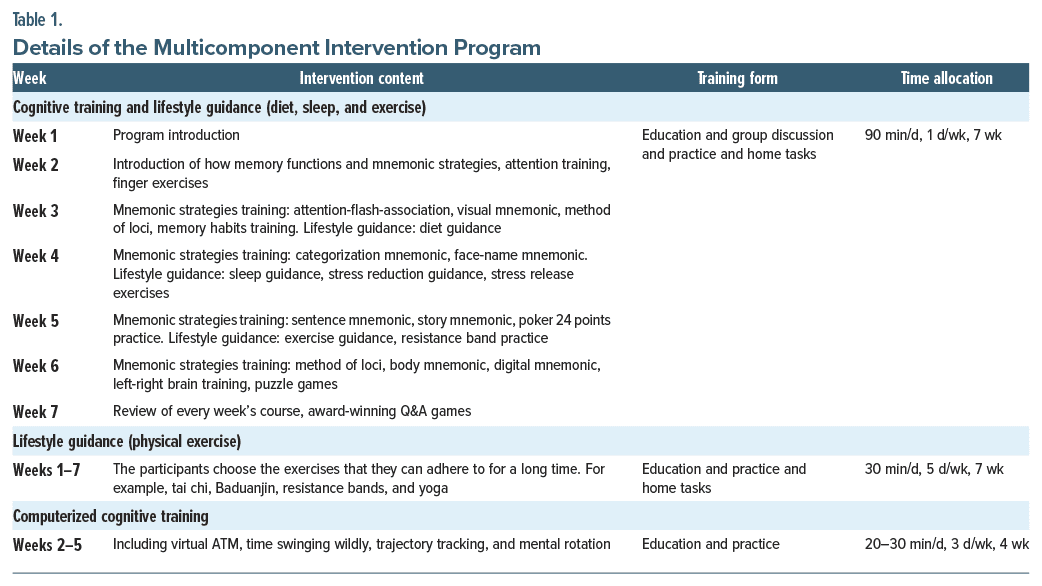
The intervention group participated in the 7-week multicomponent intervention program. The multicomponent intervention included cognitive training (mnemonic strategy training) and lifestyle guidance intervention (diet, sleep, and exercise guidance). The intervention was implemented by professionals, such as general practitioners in community health service centers and public health doctors in mental health centers, who received unified training to ensure standardization and quality of the intervention.
The cognitive training included memory and brain health knowledge, mnemonic strategies, and application of mnemonic strategies in daily life. Mnemonic strategies included visual mnemonic, story mnemonic, face-name mnemonic, and method of loci. The trainer taught each memory strategy to the participants and guided their application of the strategies in their daily lives. In addition, participants played computerized cognitive games to further enhance the fun and acceptability of the training. Participants were required to complete 90 minutes of cognitive training 1 day each week for 7 weeks and computerized cognitive training for 20–30 minutes 3 days each week for 4 weeks.
The lifestyle guidance intervention included diet, sleep, and physical exercise guidance. Participants received lifestyle guidance on diet during week 3, sleep and stress during week 4, and exercise during week 5. Each participant in the intervention group shared their 3 daily meals in a WeChat group for trainers to record. The trainers talked to the participants about their diet and sleep each week and made suggestions for adjustments. Exercise types included tai chi, Baduanjin, yoga, and resistance bands, depending on participants’ preferences, and they were required to exercise for 30 minutes 5 days per week for 7 weeks. Each week, participants were given home tasks to practice and puzzle exercises. Table 1 and Supplementary Table 1 show the details of the 7-week multicomponent intervention program.
Global cognitive function was measured by the MMSE. Three cognitive domains included memory, executive function, and attention. Memory function was measured using the immediate and delayed tests of the Auditory Verbal Learning Test (AVLT) and Logical Memory Test (LMT).35 Executive function and attention were measured using the Digital Symbol Substitution Test (DSST)36 and Digit Span Test (DST).37 Additionally, we recorded and assessed attendance in the intervention.
Statistical AnalysisAll analyses were performed according to the intent to-treat principle. Baseline demographic characteristics were determined to conduct the χ2 test for categorical data and the independent t test for continuous data. Changes in cognitive scores were evaluated using the linear mixed-effect model with cognitive scores as the response variable; time (between baseline and postintervention), group, and interaction between time and group as fixed effects; and age and gender as covariates. To determine the magnitude of exercise effects, we calculated Cohen d effect sizes. The outcome scores were calculated as Z scores, which standardized to the baseline scores and SD, with higher scores suggesting better postintervention performance compared with baseline. Statistical significance was set at P < .05 (2-tailed). All statistical analyses were undertaken using SPSS version 26.
RESULTSFigure 1 shows the flow diagram of the participants. A total of 123 participants from Xinzhuang Town, Minhang District, Shanghai, were enrolled in the trial and assigned to the intervention group (n = 62) and the control group (n = 61); however, 3 intervention group participants and 4 control group participants withdrew during the study period.
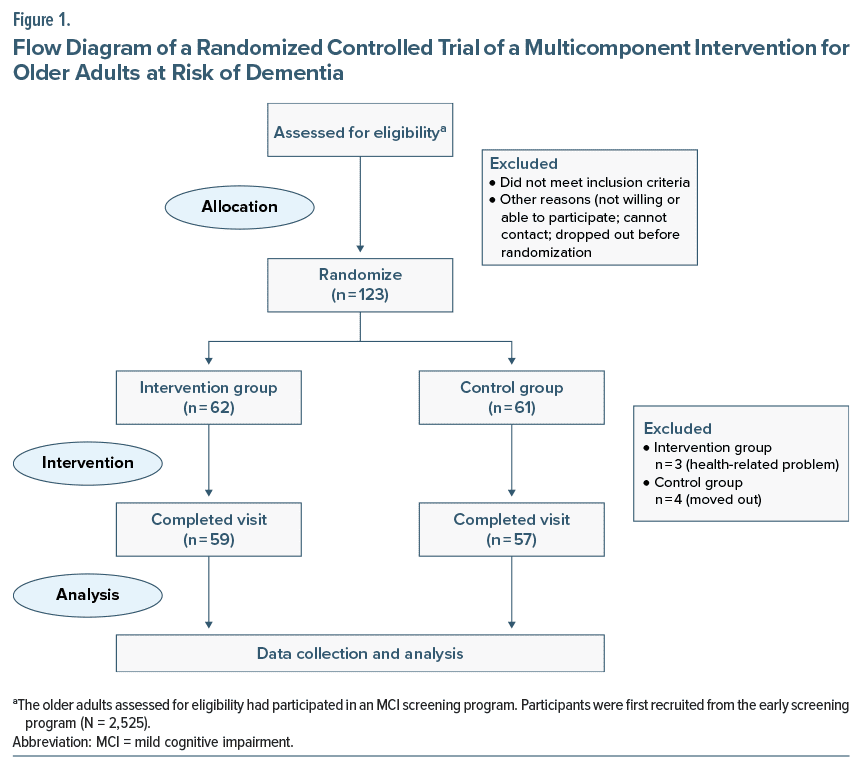
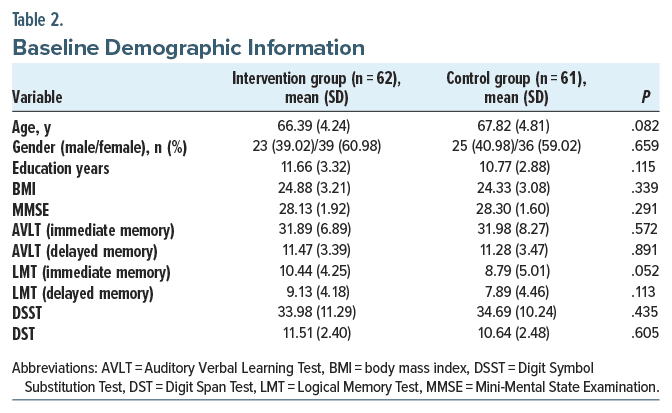
Table 2 shows the baseline characteristics of the participants in the intervention and control groups. At baseline, participants had a mean age of 67.10 years (SD=4.57). There were 75 (61.0%) women, and the average number of years of education was 11.22 (SD=3.13).
Overall, participants were able to comply with the intervention requirements. For the intervention group, the overall attendance rate of the participants was 92.01%. Supplementary Table 2 shows the details of participants’ attendance in the intervention group. For the control group, the overall attendance rate of the participants and their families was 100.00%.
Cognitive OutcomeTable 3 shows the cognitive outcomes at postintervention in the intervention group and the control group as well as timeígroup effects. Figure 2 shows the comparison of Z score means between the intervention group and the control group. The results of the linear mixed-effect model showed a significant timeígroup effect in the MMSE (Cohen d=0.63 [95% CI, 0.27 to 1.00], F=10.25, P=.002). When examining the within-group changes after the intervention, the MMSE scores increased significantly in the intervention group (d=0.94) and decreased slightly in the control group (d=−0.14).
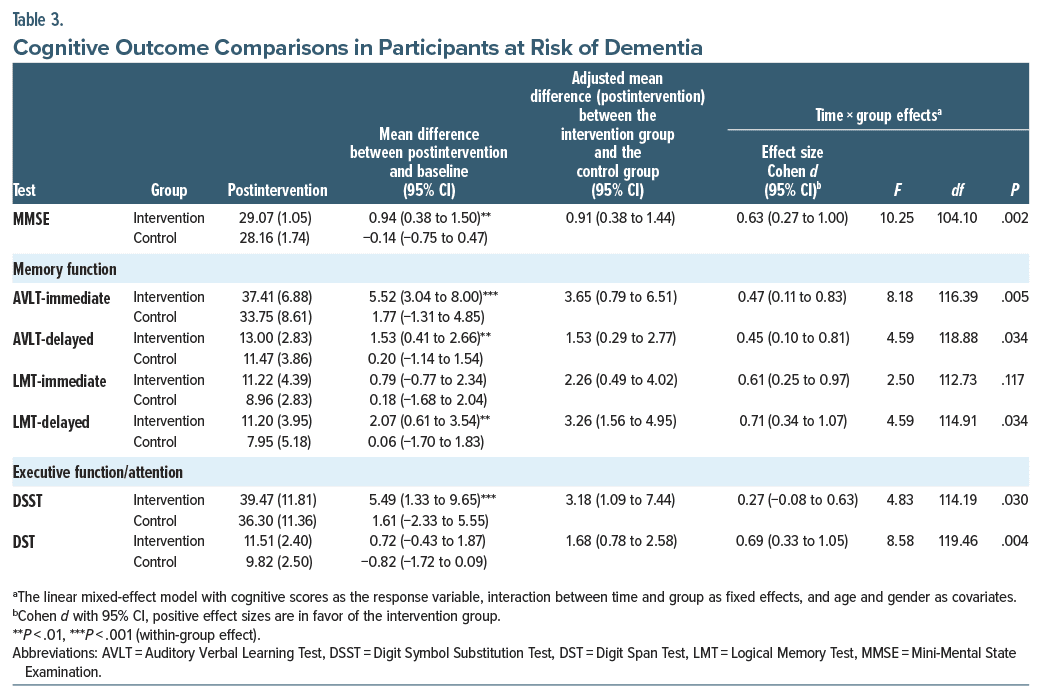
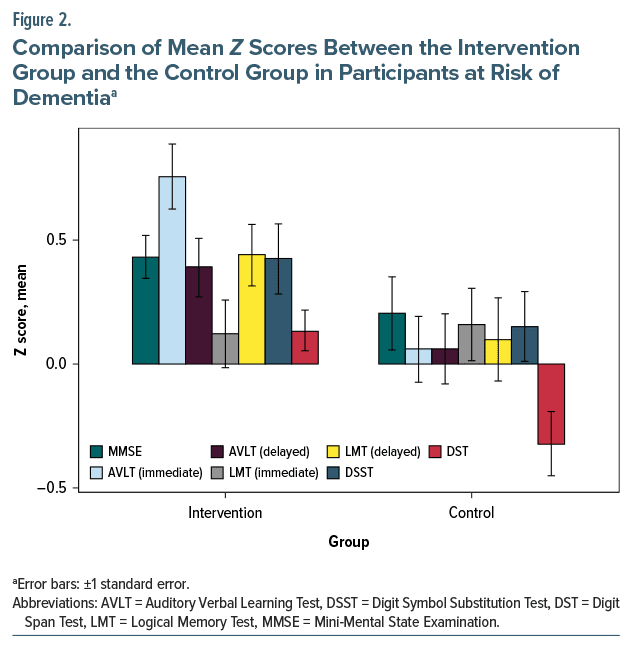
This study found significant time í group effects in AVLT-immediate (Cohen d = 0.47 [95% CI, 0.11 to 0.83], F = 8.18, P = .005), AVLT-delayed (Cohen d = 0.45 [95% CI, 0.10 to 0.81], F = 4.59, P = .034), LMT-delayed (Cohen d = 0.71 [95% CI, 0.34 to 1.07], F = 4.59, P = .034), DSST (Cohen d = 0.27 [95% CI, −0.08 to 0.63], F = 4.83, P = .030), and DST (Cohen d = 0.69 [95% CI, 0.33 to 1.05], F = 8.58, P = .004). For the within-group differences after the intervention, the intervention group showed significant improvements in AVLT-immediate (d = 5.52), AVLT-delayed (d = 1.53), LMT-delayed (d = 2.07), and DSST (d = 5.49), while the control group showed no significant improvements.
DISCUSSIONThis is the first study on a multicomponent intervention focusing on mnemonic strategy training and lifestyle intervention targeting community-dwelling older adults at risk of dementia in China. We found it effective in improving participants’ cognitive function. The program showed potential as an effective intervention; however, it warrants further validation with larger sample sizes and longer follow-up. The training components included in this intervention program are simple to implement and do not require specific equipment. The program requires community workers with a medical background to participate in a 2- day training session and obtain the courseware and the associated computer program (computerized cognitive training games). The significant improvements, good adherence, and replicability of trainers’ training suggested its suitability for community replication for older adults at risk of dementia.
This study showed that the multicomponent intervention was effective in improving cognitive function, including MMSE, memory, executive function, and attention, in older adults at risk of dementia. This is supported by findings in previous studies. A review has shown that a multidomain intervention yields greater improvements in global cognition, executive function, memory, and verbal fluency scores compared to a single domain intervention.38 The FINGER study in Finland, one of the largest multidomain interventions in a community, showed an improvement in overall neuropsychological test battery scores and significant improvements in executive function and processing speed in older adults at risk of dementia after 2 years of the intervention.30 The Body Brain Life for Cognitive Decline, a multidomain dementia risk reduction randomized controlled trial for older adults in Australia with SCD or MCI that included dementia and lifestyle risk factors, Mediterranean diet, physical activity, and cognitive engagement, showed significant cognitive improvement in the intervention group, supporting the idea that improving lifestyle risk factors for dementia can improve cognitive performance in a short period of time.39 A review found that multidomain lifestyle interventions that address multiple risk factors may delay the onset of cognitive impairment or dementia by reducing neuropathic damage and increasing cognitive reserve.21 However, the review also mentioned that multidomain interventions on single measures, such as MMSE or MoCA, showed no significant improvement in global cognition and only a slight improvement. The present study showed that a similar multicomponent intervention was effective in improving global cognitive function in Chinese community-dwelling older adults.
At the end of the intervention, the AVLT and LMT delayed scores improved more in the intervention group than in the control group, which indicates a significant improvement in memory. The mnemonic strategy training in the multicomponent intervention of this study may have played a role in the improvement of memory function because it mainly trains participants in memory skills and helps them to store memories more effectively. These results are consistent with studies on the effects of mnemonic strategy training with older adults with SCD or MCI,40,41 and imaging results of mnemonic strategy training have shown improvements in brain activity.15,42
In a study of older adults with SCD, participants tended to spontaneously use more mnemonic strategies to compensate for the memory decline they experienced, and using the strategies in everyday life situations made them more beneficial.43 This study suggests that the effectiveness of emphasizing mnemonic strategy training in a multicomponent intervention may have a positive effect on the more effective implementation and use of mnemonic strategies in daily life to consistently strengthen memory in older adults at risk of dementia. In addition, lifestyle interventions may also play a role in memory improvement. A multicomponent holistic health group intervention study of older adults with MCI in a Chinese community showed similar results for interventions including diet, exercise, and socialization, with results showing a strong effect size on improving participants’ delayed memory.44 An intervention study45 of older adults at risk of dementia found that an active lifestyle, defined as activity diversity in cognitive, physical, and social activities, was significantly associated with changes in global cognition and memory. Furthermore, the association between lifestyle and cognitive change produced stronger effects than specifically designed cognitive training for older adults at risk of dementia.
This study showed significant between-group effects for DSST and DST scores, suggesting that this multicomponent intervention improved participants’ executive function and attention. A study46 of a combined diet and exercise intervention with older adults with cardiovascular disease risk factors and cognitive impairment without dementia showed that diet and exercise lifestyle changes promoted better executive function. In addition, the study identified the potential mechanisms for these lifestyle interventions to improve neurocognition and to increase functional capacity, all of which were associated with improvements in executive function. In this study, daily instruction and monitoring of diet and exercise may have led participants to follow a more active lifestyle during the intervention. In addition, group-based training caused participants to question and interact more, and computerized cognitive training required their continuous attention to the training process, which may have been associated with improvements in executive function and attention.
The participants in this study had high attendance and low dropout rates, suggesting the potential for replication and scaling of this multicomponent intervention program for a community. This multicomponent intervention program combines cognitive training with lifestyle guidance, which may be attractive to the older adult population by aiding with concerns about cognitive decline and providing guidance for their daily health needs. One review has mentioned that a multidomain intervention may have higher adherence and greater appeal than a single intervention.21 In addition, no adverse events were reported with the implementation of this study, suggesting that it is safer for older adults at risk of dementia.
This study has several limitations. First, this study did not have a long follow-up period; longer follow-up observations are required to further determine the effects of the intervention. Second, the generalizability of the study results may be limited by the small sample size, and larger community randomized controlled trials are needed to test the feasibility of scaling and implementing the intervention in a community. Third, more neuropsychological tests and measures should be included to measure changes in cognitive domains and lifestyle more comprehensively. Fourth, it is possible that due to the limitations of the baseline scores, the MMSE scores in the intervention group may not reach the minimum clinically important difference. Future studies will require longer follow-up periods, larger sample sizes, and more complete and varied measures.
ConclusionsThe results showed that a multicomponent intervention program of mnemonic strategy training combined with lifestyle intervention including diet, sleep, and exercise instruction significantly improved global cognitive function, memory, executive function, and attention in the participants. The positive results of this randomized controlled trial suggest that it may have the potential to improve cognitive function in community dwelling older adults at risk of dementia and can be replicated in the community.
Article InformationPublished Online: May 13, 2024. https://doi.org/10.4088/JCP.23m15112
© 2024 Physicians Postgraduate Press, Inc.
Submitted: September 19, 2023; accepted January 8, 2024.
To Cite: Wang P, Yang T, Peng W, et al. Effects of a multicomponent intervention with cognitive training and lifestyle guidance for older adults at risk of dementia: a randomized controlled trial.
J Clin Psychiatry. 2024;85(2):23m15112.
Author Affiliations: School of Public Health, Fudan University, Shanghai, China (P. Wang, Peng, Yao, Y. Wang); NHC Key Laboratory of Health Technology Assessment, Fudan University, Shanghai, China (P. Wang, Y. Wang); Shanghai Center for Clinical Laboratory, Shanghai, China (T. Yang, Y. Yang); Eye & ENT Hospital, Fudan University, Shanghai, China (M. Wang, Chen); Department of Geriatrics, Huashan Hospital, Fudan University, Shanghai, China (Huang); Tian Qiao and Chrissy Chen Institute Clinic Translational Research Center, Shanghai, China (Huang); Minhang District Mental Health Center of Shanghai, Fudan University, Shanghai, China (Jiang, F. Wang, Ding); Shanghai Municipal Center for Disease Control and Prevention, Shanghai, China (Sun, Ruan).
Drs P. Wang and T. Yang contributed equally to this work.
Corresponding Authors: Ying Wang, PhD (wangying1013@fudan.edu.cn), and Ye Yao, PhD (yyao@fudan.edu.cn), No. 130 Dong’an Rd, Xuhui District, Shanghai 200032, China.
Relevant Financial Relationships: The authors declare that there are no conflicts of interest.
Funding/Support: This work was supported by the National Key Research and Development Project (2017YFC1310504), National Natural Science Foundation of China (71673055), Shanghai Leading Academic Discipline Project of Public Health (GWV-10.1-XK18), and Public Health Key Discipline Construction Project of Minhang District, Shanghai (MGWXK05).
Role of the Sponsor: The sponsors had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgments: We would like to thank all participants and trainers involved in the study. We would also like to thank all the staff who contributed to participants’ recruitment, the intervention, and data collection for this study.
Ethics Approval: This study was approved by the Ethics Review Committee of Fudan University School of Public Health (IRB#2020-07-0840).
Supplementary Material: Available at Psychiatrist.com.
留言 (0)