
記住我








A 47-year-old woman, non-smoker, with history of asthma and pollen allergy contacted the emergency services for subacute dyspnea, exercise intolerance and chest tightness. Her daily medication consisted of: desloratadine, a beclomethason/formoterol inhaler and an ethinylestradiol/levonorgestrel contraceptive, which she took on a continuous basis (without pill-free days) because of pre-menopausal menometrorrhagia. She had been feeling unwell for two days and thought her symptoms were due to an asthma attack. She had already tried increasing her inhaler, but without effect. Two days earlier she had returned from holiday after an 18-hour bus ride. She had taken the same bus on the outward journey 10 days earlier.
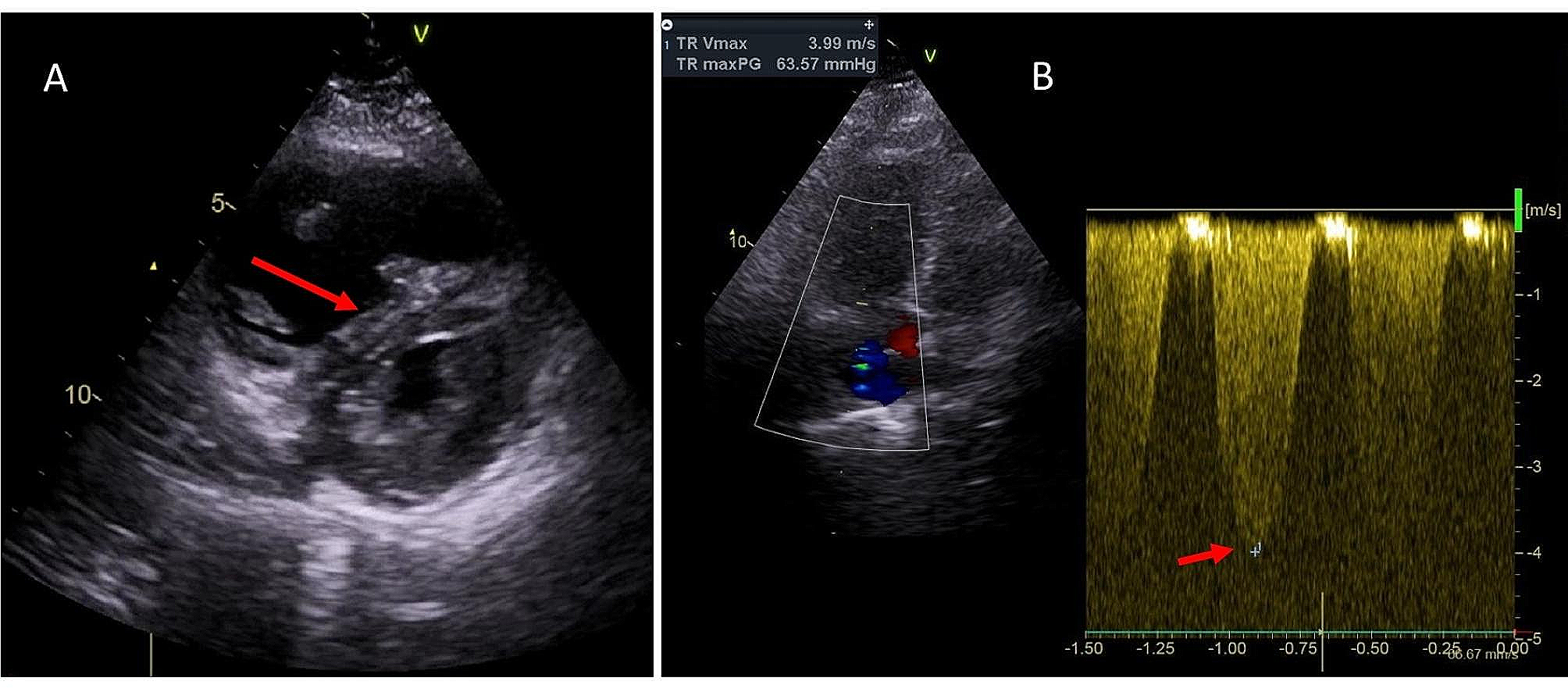
On arrival, the first responders team found her sitting on the ground in respiratory distress, tachypneic, tachycardic, hypoxic, hypotensive, and afebrile. Her vital signs were: respiratory rate 36 breaths per minute, heart rate 142 beats per minute (bpm), oxygen saturation 72% on room air, blood pressure 64/43 mmHg and temperature 35.8 °C. ECG showed sinus tachycardia, without Q waves or ischemic ST/T changes. The patient was given 12 L/m of oxygen via face mask and 500 mL of normal saline and was brought to the hospital. Repeat ECG showed similar findings, lab (results of which were only available later) showed hemoglobin of 14.0 g/dL, troponin 330 ng/L, d-dimers 7509 mcg/L, C-reactive protein 30.4 mg/L and creatinine of 1.31 mg/dL, corresponding to estimated glomerular filtration rate of 48 mL/min/1.73m2. Quick-look echocardiogram showed a nondilated and normocontractile left ventricle, a dilated right ventricle with leftward shift of the interventricular septum and pulmonary hypertension with an estimated right ventricular systolic pressure of 64 mmHg + central venous pressure (Fig. 1). Inferior caval vein was plethoric without respiratory variation. There was no severe valvular pathology. At that moment, blood pressure was 142/95 mmHg, heart rate 139 bpm and oxygen saturation 97% while breathing 12 L/m oxygen via face mask.
Fig. 1
Transthoracic echocardiogram: (A) Parasternal short axis image, showing dilated right ventricle with systolic D-shaping of the interventricular septum (arrow); (B) Continuous wave doppler in apical four chamber view, showing estimated pulmonary artery systolic pressure of 64 mmHg + central venous pressure, as measured by tricuspid regurgitation jet velocity (arrow)
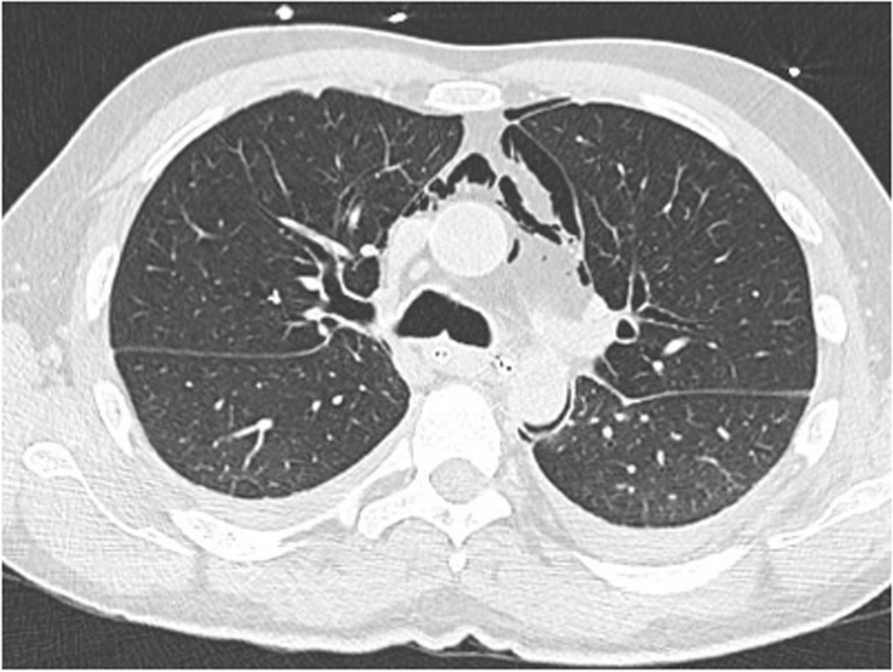
Acute pulmonary embolism was suspected. The patient was given 80 mg of enoxaparin (weight = 83 kg) and an urgent computerized tomography scan with intravenous contrast was performed, which confirmed the diagnosis of bilateral pulmonary embolism (Fig. 2).
Fig. 2
Computerized tomography scan with intravenous contrast, showing pulmonary embolism (arrows) in right and left pulmonary artery
The Pulmonary Embolism Severity Index (PESI) score, calculated with the help of an online tool [2], was 167: very high risk. Based on hemodynamic compromise, right ventricular dysfunction on echocardiogram and a very high-risk PESI score, thrombolysis was administered. Alteplase was given as a 10 mg bolus and 90 mg infusion over 2 hours and the patient was admitted to the cardiac intensive care unit. Her condition gradually improved over the next few hours, with a decrease in heart rate from 130 bpm to 80 bpm and normalization of serum creatinine to 0.81 mg/dL (corresponding to eGFR of 85 mL/min/1.73 m2) by the second day. Repeat echocardiography showed a marked decrease in right ventricular dimensions and lowering of estimated right ventricular pressure to 27 mmHg + central venous pressure. In addition to the pulmonary embolism, the patient was found to have extensive deep venous thrombosis of the right femoral vein. Thrombophilia screening revealed a Factor V Leiden mutation. After two days of enoxaparin, 80 mg (1 mg/kg) twice daily, she was switched to rivaroxaban, 15 mg twice daily and at day 6 she was discharged with this therapy for a total of 21 days, after which she should decrease the dose to 20 mg once daily. She was instructed to discontinue her combined oral contraceptive pill indefinitely.
Five days later, however, the patient was re-admitted to the hospital with pre-syncope. She was looking pale. During the few days between hospital admissions, she had had severe vaginal bleeding, with need for hygienic pad change every few hours. Vital signs were: blood pressure 102/74 mmHg, heart rate 114 beats per minute, respiratory rate 18 per minute, saturation 99% on room air, temperature 36.7 °C. There was no hematuria, melaena or hematochezia. Hemoglobin was 6.3 g/dL, ß-HCG negative, creatinine 0.96 mg/dL and C-reactive protein 2.1 mg/L. INR was 1.4 (12 h after last intake of rivaroxaban).
Fig. 3
Graph showing evolution of Hemoglobin (y-axis, in g/dL) over Time (x-axis, in days). First hospitalization (admission on day 0, discharge on day 6) and second hospitalization (admission on day 11 and discharge on day 18) are indicated. Vertical arrow indicates transfusion of 2 units packed cells and 500 mL of normal saline
Figure 3 shows the evolution of anemia since the previous hospitalization. 500 mL of normal saline and two units of packed cells were infused. Rivaroxaban was withheld for 5 days and substituted for prophylactic dose enoxaparin, 40 mg once daily. Lynestrenol, an oral progestin, was administered at 5 mg twice daily for two weeks, and then switched to nomegestrol 5 mg once daily, to be taken continuously. An oral iron supplement was started to replete the iron stores. The patient was discharged on day 7.
留言 (0)