
記住我






Similar to a more recent US-based study, we reviewed the currently available over-the-counter citrate-based alkali supplements sold in Germany [27]. Noticeable differences between the identified supplements were encountered, both with regard to the mineral content as well as with the PRAL-lowering potential of each product.
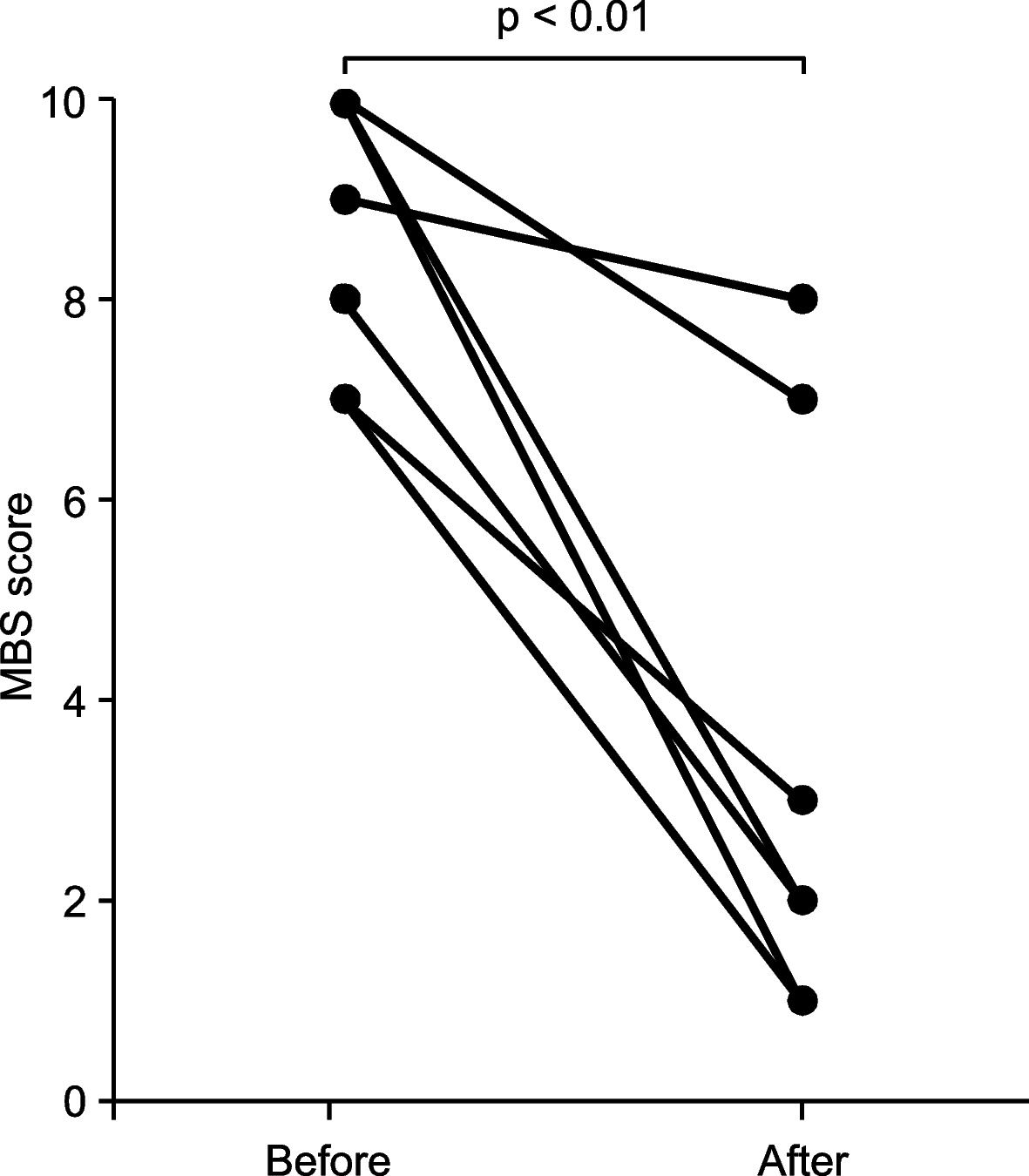
Prospective clinical studies investigating the effects of such supplements rich in alkaline minerals on the acid-base balance in humans are generally scarce and limited to a handful of trials [28, 29]. Vormann et al. hypothesised that a latent chronic acidosis subsequent to a high PRAL might contribute to low back pain (LBP), and conducted an open prospective study in n = 82 patients with chronic LBP who received 30 g of a lactose based alkaline multimineral supplement (Basica®) daily for a period of 4 weeks [28]. Pain symptoms were assessed with the “Arhus low back pain rating scale” (ARS), and mean ARS scores dropped significantly by 49% (-20 points in total) after 4 weeks of supplementation. König et al. enrolled n = 25 (15 females; 10 males) participants in a study investigating the effects of a multimineral alkali supplement (MMS) on acute and chronic regulation of acid-base balance with the pH of blood, urine and saliva as potential surrogate markers [29]. Blood and urinary pH significantly increased in this uncontrolled study. Following a longer supplementation period, both the increase in urinary pH in the morning and in the evening occurred within 24 h. Compared to pH values without the MMS, average pH in urine was more than 10% higher in the morning and approximately 5% higher in the evening.
Moseley et al. suggest that potassium citrates may also improve skeletal health [30]. The authors conducted a randomized, double blind and placebo controlled study in 52 elderly women and men with a mean age 65.2 ± 6.2 years. Participants were randomly assigned to one of the following regimens: potassium citrate 60 mmol per day, 90 mmol per day or placebo. Bone turnover markers, net acid excretion and calcium balance were examined at baseline and after a half year. Notably, net acid excretion decreased significantly in both treatment groups when compared to the place. The regular supplement intake resulted in a complete neutralization of the participants’ dietary acid load. Favorable findings were also reported by Granchi et al. in a 2018 study, which also employed a potassium citrate supplement in osteopenic women [31].
While large-scale randomized-controlled clinical trials are scarce in this field of study for endpoints unrelated to the human kidneys or bone health, alkali supplements might serve several purposes. From our personal clinical perspective, they might be a helpful tool to decrease PRAL in individuals with an otherwise high dietary acid load, particularly when transitioning towards a more plant-based diet. For a quantitative comparison, Fig. 4 summarizes the PRAL values of some commonly consumed alkalizing fruits and vegetables, based on data obtained from Remer and Manz [26].
Fig. 4
Potential renal acid load of commonly consumed alkalizing vegetables. Based on [26], images modified from Servier Medical Art database by Servier (Creative Commons 3.0; https://smart.servier.com/)
A clear reservation must be made that such supplements do not qualify as fruit and vegetable substitutes, and may not replace a healthy diet. Fruits and vegetables contain numerous health promoting substances, including carotenoids, phenolic antioxidants, and anthocyanidin, which all have proven benefits to human health [32].
In this context, a reduction in dietary acid load has been shown to reduce kidney injury in patients with moderately reduced eGFR (glomerular filtration rate) due to hypertensive nephropathy, and fruits and vegetables were comparable to sodium bicarbonate in an investigation by Goraya et al. [33]. Notably, newer studies by the same authors highlighted the additional benefits of fruits and vegetables over oral alkali supplementation [34].
Here, we reviewed citrate-based supplements available in Germany and found noticeable differences between the different supplements. Not designed as a head-to-head comparison, we intentionally focused on a descriptive analysis and do not recommend one supplement over another supplement. To the contrary, we encourage the reader to carefully review the unique characteristics of each examined supplement described here, and to consider whether an enrichment with other minerals might be suitable in a particular clinical situation or not. This might be of particular importance because many supplements contained additional nutrients that may not necessarily decrease PRAL but are marketed under different purposes. A common example is zinc, which is added to almost all examined supplements (Table 2), and which - according to the PRAL formula by Remer and Manz - does not alter PRAL. We can only guess why additional nutrients were added to the examined supplements and supposed that they were included for marketing purposes (e.g., because an optimal zinc status is associated with a healthy immune system). Whether necessary is subject to a controversial debate and beyond the scope of this paper. Yet, we deemed it important to systematically capture these nutrients and vitamins added to the examined dietary supplements even when they do not add to their PRAL-lowering potential.
Whether such supplements enriched with additional vitamins and nutrients may be helpful in a particular clinical situation cannot be answered with this cross-sectional study design and is beyond the scope of the paper. Likewise, we did not review supplement characteristics such as flavor, taste or consistency.
As such, this short contribution has strengths and weaknesses that warrant a careful consideration. Entirely descriptive, we do not recommend a particular supplement over another supplement, but provide the reader with a list of potentially available citrate-based dietary alkali supplements in Germany. Although we carefully screened multiple online pharmacies and local drug stores to capture as many products as possible, we may not guarantee a complete list of products. In addition, we only considered food/dietary supplements for this analysis; medicinal products and drugs that warrant a prescription from a physician for a specific medical indication were not considered here. Finally, we acknowledge that the primary source of each examined product (e.g. rock (dolomite, limestone), animal (oyster shellfish powder, coral), plant (plant and wood ash) was not ascertainable from the available data. Although many products were declared “vegan” and as such contained no ingredient of animal origin, we may not provide additional details here.
The authors wish to emphasize that they declare no conflicts of interest and no supplement was reviewed more favorably than another one.
留言 (0)