
記住我




Diakonhjemmet Hospital treats 450 patients with hip fractures yearly, within a dedicated orthogeriatric unit. Hip fractures are operated during daytime and the evening, but not during the night (23–08). Most procedures are done by orthopedic surgeons in training, often assisted by consultant orthopedic surgeons. There are no guidelines restricting the timing of the surgery itself after intake of DOACs. Anesthesia is provided by the anesthesiologist on call, and the choice of anesthesia is based on this anesthesiologist’s clinical judgment. In our department, SA is the preferred mode of anesthesia in hip fracture patients. This is because SA gives good postoperative pain relief and because GA is viewed as more complicated in patients with respiratory and cardiovascular comorbidities. Internal guidelines state that SA should be delayed 48 h after intake of DOACs. Patients who have been using DOACs can be operated in GA at any time, if the anesthesiologist considers this to be safe.
The databaseSince 2006, all patients with hip fractures have been registered in an internal registry (Diakonhjemmet Hip Fracture Registry (DHFR)). The database contains data about comorbidities, medication, treatment, complications, demographic information, laboratory tests, fracture classification, operation type, ASA class, and time of surgery. The information is collected from the electronic patient file by a trained nurse after discharge of the patient, and information about deaths are collected from the Norwegian National Population register.
Information about DOAC use has been systematically recorded from 2015, and patients treated before this time were excluded from the analysis. To ensure complete one-year mortality data, patients treated after 31.12.2021 were also excluded.
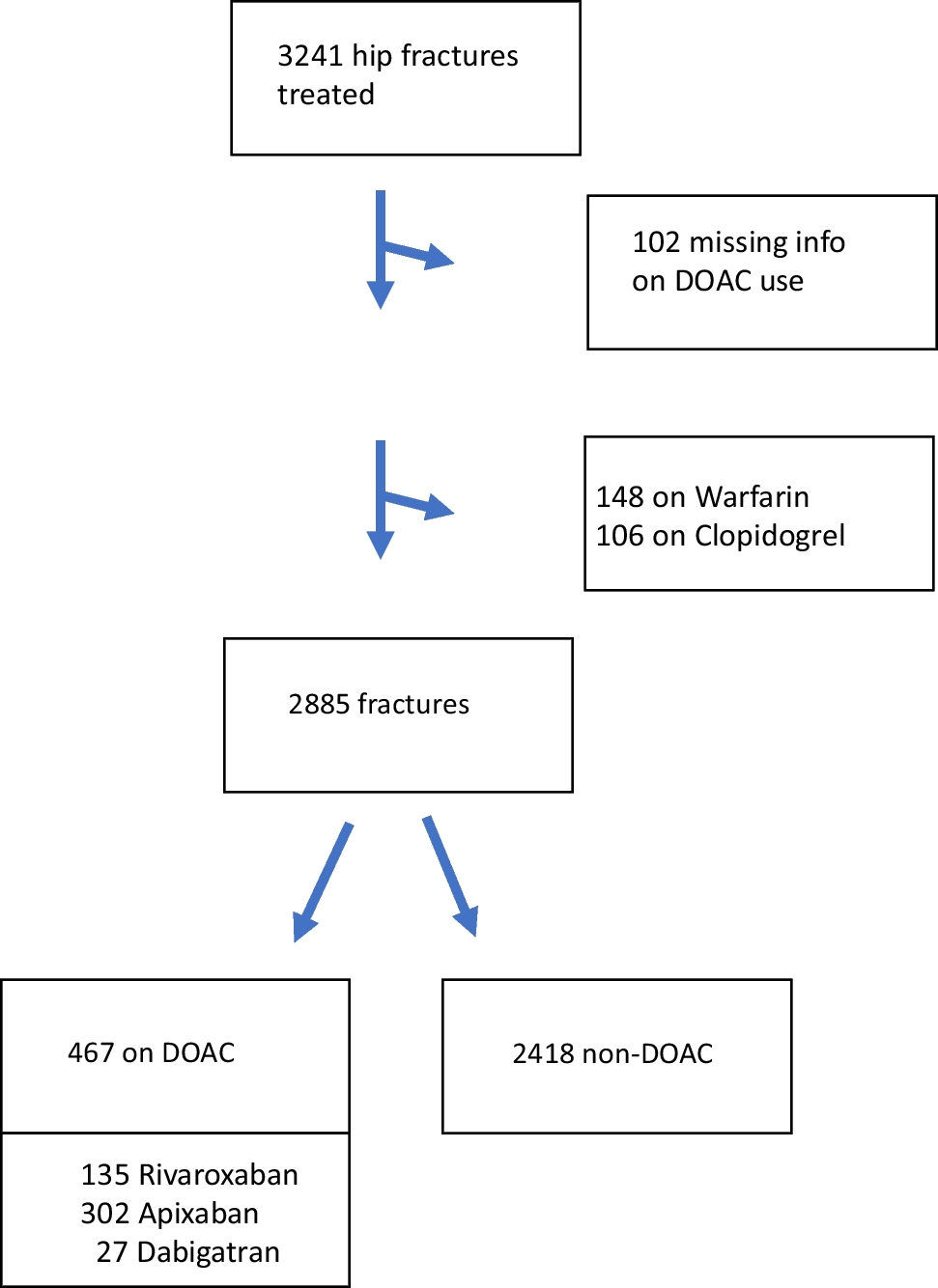
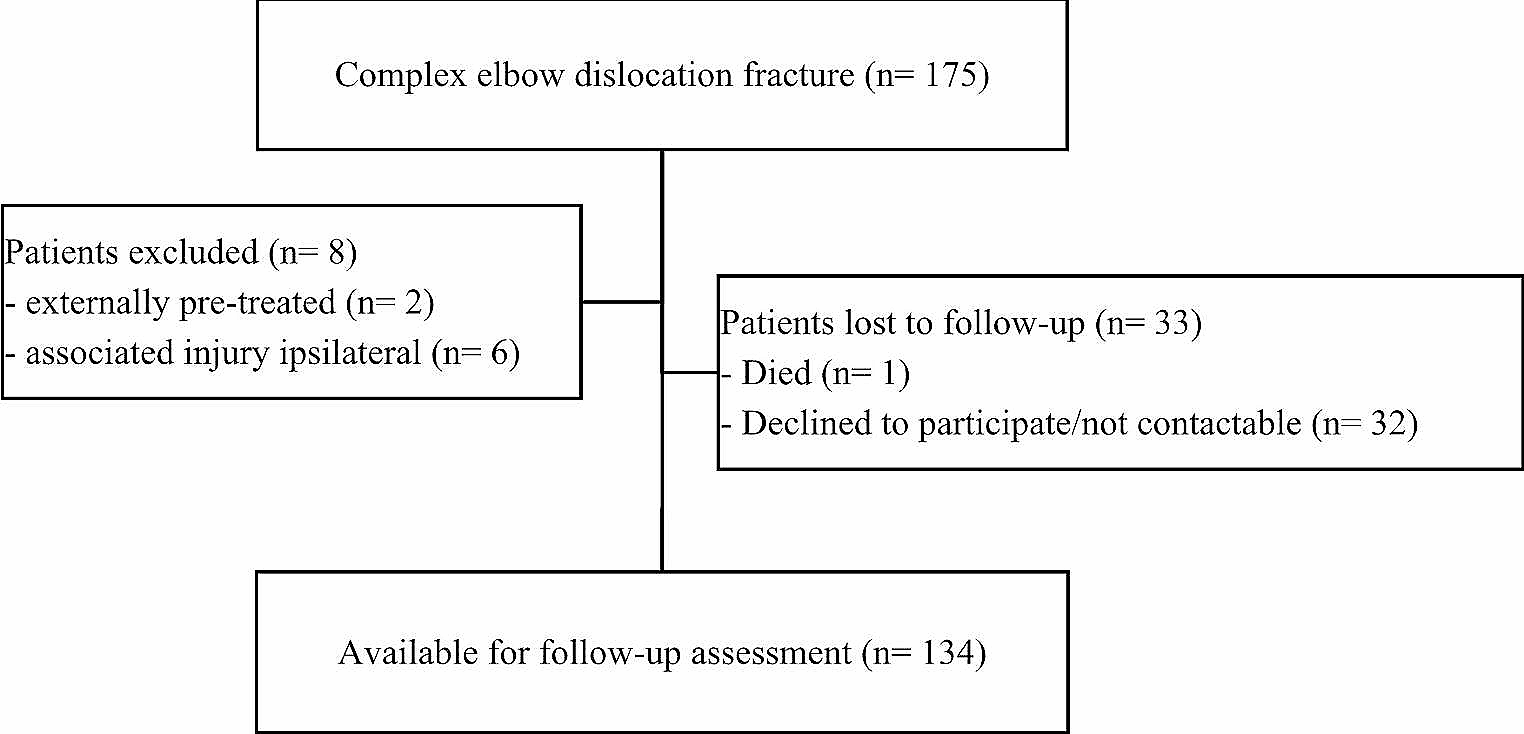
Warfarin and clopidogrel are anticoagulants that are not DOACs, but patients using these drugs have related comorbidities and the same considerations concerning spinal anesthesia, and these patients were therefore excluded from the study. Patients using acetylsalicylic acid and/or dipyridamole were included in the non-DOAC group. Figure 1 contains a flowchart of study subject inclusion.
Fig. 1
Flow chart of the patients included in the study
Exposures and outcomesThe main exposure in this study was the use of DOACs (rivaroxaban, apixaban, edoxaban or dabigatran). We also assessed the choice of anesthesia (SA or GA) in DOAC patients. We had no information about the timing of the last intake of DOACs.
The main outcome in this study was waiting time between admission and surgery, reported in hours. Other outcomes were blood transfusion (yes/no), length of stay (days), death within a month (30 days) after admission, and death within a year (365 days) after admission.
Data analysisEach hip fracture was analyzed as a separate case, although some patients had a repeated admission for a contralateral fracture. Demographic factors were described by means or frequencies (percent), grouped by whether they used DOACs or not. The statistical significance of differences in proportions was tested with chi-square tests, differences in means were tested with linear regression, and differences in medians were tested with quantile regression. The outcomes waiting time and hospital stay were right-skewed and not normally distributed, but due to the large number of observations the assumptions for linear regression were met. Directed acyclic graphs (DAGs) were utilized to develop a model of the causal relationship between DOAC use as an exposure, and mortality as an outcome (Fig. 2). The Charlson Comorbidity Index (CCI), age, and gender were chosen as adjustment covariates when analyzing all outcomes. Nursing home status (yes/no) was also included as an adjustment factor in the analysis of outcomes of SA or GA in DOAC patients. Waiting time before surgery was viewed as a mediator on the causal paths between DOAC use/choice of anesthesia and mortality (Fig. 2) and was not adjusted for in the analysis. To analyze the direct effect of DOAC use on mortality, waiting time grouped into categorical categories were included as an adjustment covariate. Directed Acyclic Graphs for the other analyses, made with Dagitty software [13], are available in the online supplementary information. The effect of age was non-linear, and age was therefore analyzed as a categorical covariate by decades. The CCI had a linear association with mortality and was used as a continuous covariate. There were 2% missing values for nursing home status, and these were excluded in the one analysis where this was used for adjustment. There were no missing values for the other adjustment covariates, and no imputation was necessary. All analyses were done using STATA version 17.0 (StataCorp, College Station, Tx, USA).
Fig. 2
Directed acyclic graph of the association between DOAC use and survival. In this analysis the red covariates are confounders, and should by adjusted for. Waiting time is a mediator between DOAC-use and mortality, and should not be adjusted for to measure the total effect. When investigating the direct effect of DOACs on mortality, waiting time should be adjusted for (source: dagitty.net)
Ethical issuesThe study has been performed in accordance with the standards of the Helsinki declaration. The database is approved by our hospital research board and our data protection officer. Patients are informed about their registrations in the database, but do not provide a formal written consent. This is in accordance with Norwegian legislation about research on data from quality databases. No harm is conceivable for the patients by inclusion in the study.
留言 (0)