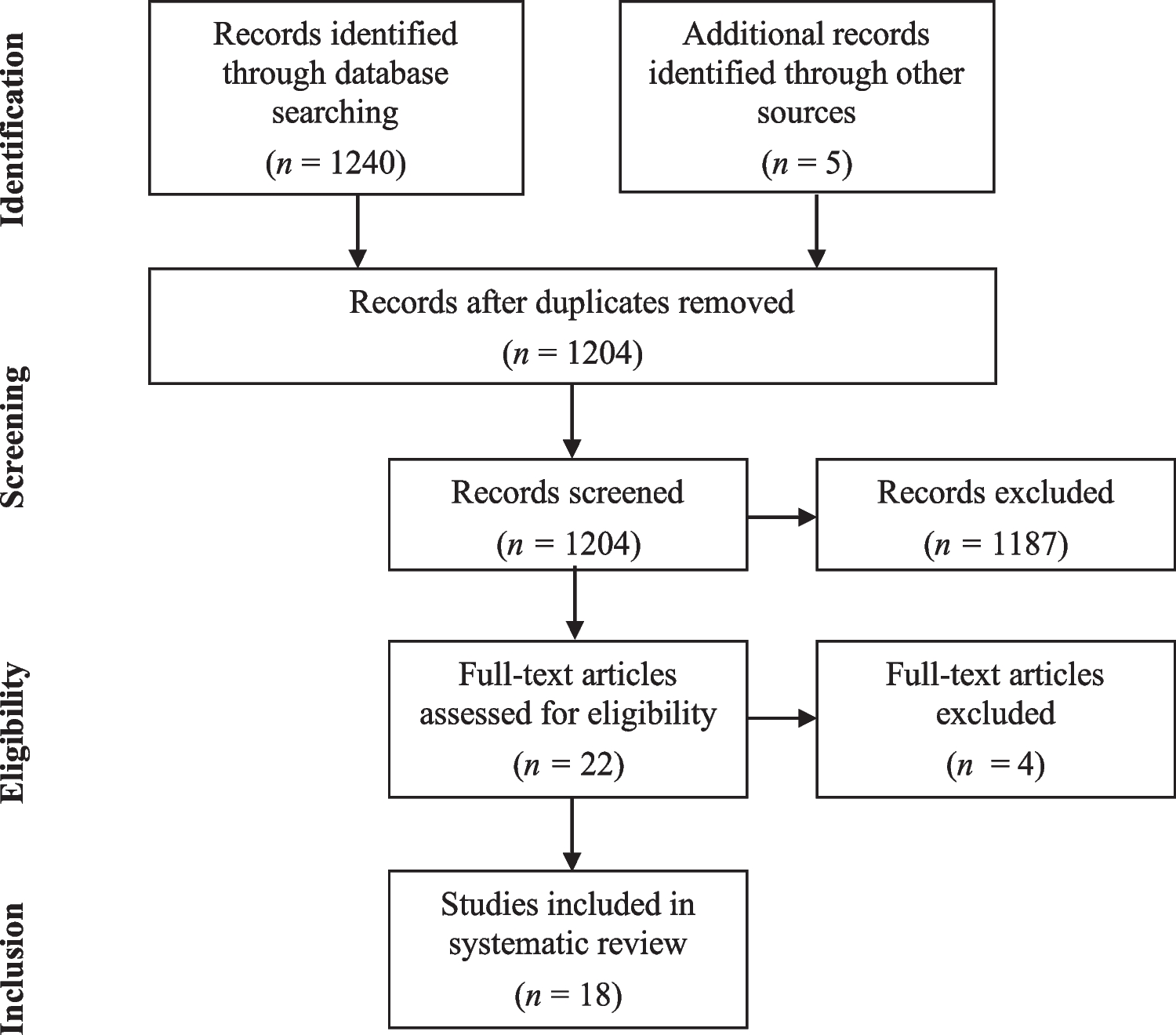
Eighteen studies met inclusion criteria and comprised a total sample of 4,420 patients. This included 2,883 (68.9%) patients with relapsing–remitting MS (RRMS), 407 (9.7%) patients with secondary-progressive MS (SPMS), 279 (6.7%) patients with primary progressive MS (PPMS), 178 (4.3%) patients defined as early RRMS (including Clinically Isolated Syndrome, which not all countries routinely document), and 33 (0.8%) patients with progressive-relapsing MS (PRMS). A further 402 (9.61%) patients had an ‘unclear’ diagnosis. One study did not provide information on patient diagnoses [9], with diagnostic information available for 4,182 patients. Gender information was available for 4,320 patients. The mean age of patients was 40.6 years and 3,013 (65.3%) patients were female. Country of recruitment was reported in 17 studies, with 1,979 (45.8%) recruited from Germany, 995 (23%) from Italy, 742 (17.2%) from the USA, 200 (4.6%) from Saudi Arabia, 152 (3.5%) from Australia, 96 (2.2%) from Brazil, 81 (1.9%) from Canada, 29 (0.7%) from Spain, 20 (0.5%) from Turkey, 14 (0.3%) from the Netherlands and 11 (0.3%) from Serbia.
Quality assessment
The EPHPP Quality Assessment Tool for Quantitative Studies [25] was used to assess study quality (Table 1). Fourteen studies were rated overall ‘weak’, 1 overall ‘moderate’ and 3 overall ‘strong’. Data from studies with ‘weak’ ratings should be considered cautiously due to having less control over additional factors potentially implicated in the results than studies with randomised-controlled designs.
Table 1 Study quality ratingsMS knowledgeValidated measures
Seven studies used validated MS knowledge measures. Abulaban et al. [9] conducted an internet survey to assess patients’ MS knowledge in Saudi Arabia. A large sample of MS patients completed the MS Knowledge Questionnaire (MSKQ) [11]. With a mean score of 13.6 (SD = 3.6) out of a maximum of 23, the authors concluded patients’ knowledge of MS disease types and treatment was lower relative to their knowledge of its pathophysiology.
Bruce et al. [26] assessed how MS patients weigh disease modifying therapy (DMT) risks and benefits when making treatment decisions. Patients completed a medical decision making task to assess their willingness to take a hypothetical DMT as their efficacy and side effects probabilities varied. Patients completed the MSKQ to assess how MS knowledge related to self-reported likelihood of initiating treatment. The authors reported a mean MSKQ score of 17.4 (SD = 3.4).
Using an analogous medical decision making task, Bruce et al. [27] investigated how patients weigh treatment decisions, with specific consideration given to how patients discount DMT efficacies and side effects. The association of demographics, clinical characteristics, MS knowledge, cognitive and emotional functioning, and treatment adherence were studied. The authors obtained a mean MSKQ score of 17.5 (SD = 3.4). The authors further observed poorer cognitive functioning was related to greater benefit discounting.
To measure MS knowledge, Giordano et al. [11] developed and validated the MSKQ on a small sample of MS patients. Further to compiling the final 25-item multiple choice questionnaire, newly diagnosed patients completed the MSKQ, with a median score of 17 obtained from a possible score of 25.
Giordano et al. [28] measured cross-cultural differences in MS knowledge and MS risk knowledge using the MSKQ and Risk Knowledge questionnaire 2.0 (RIKNO 2.0) [10]. The mean MSKQ score was 19.3 (SD = 3.2; n = 298).
In their validation of the RIKNO 2.0, Heesen et al. [10] invited a large group of MS patients to complete the MSKQ and RIKNO 2.0. Measures of patient demographics, clinical characteristics, disease severity, quality of life and self-reported cognitive functioning were collected. Heesen et al. [10] obtained a mean MSKQ score of 20.1 (SD = 2.6).
Examining MS patients’ sensitivity to DMT prices and how these related to adherence and MS knowledge, Jarmolowicz et al. [29] invited a large sample to complete the MSKQ and measures of demographics, disease severity, emotional and cognitive functioning, adherence and a medication purchasing task. The mean MSKQ score obtained was 17.1 (SD = 3.5). A recent review of MS disease-related knowledge measures has only provisionally recommended use of the MSKQ and RIKNO, until further psychometric evidence is provided [30].
Unvalidated measures
Four studies used bespoke knowledge measures within intervention studies to assess baseline MS knowledge. Feicke et al. [31] compared the effectiveness of a self-management training programme with a standard information brochure. Self-management ability and MS knowledge were measured before, immediately post- and 6 months post-intervention. Patients showed a good degree of MS knowledge at baseline, with more than 75% correct responses provided.
Patients’ perceived knowledge of therapeutic decisions was investigated by Heesen et al. [15]. A large sample of MS patients completed questionnaires of their self-reported knowledge, information interests and treatment decisional role preferences. Most patients rated their subjective perceived level of knowledge as 63% (100% representing maximal subjective knowledge).
Evaluating a decision aid for female MS patients considering beginning or enlarging their families, Prunty et al. [32] measured changes in MS knowledge, decisional self-efficacy, and decisional conflict. Patients completed baseline knowledge measures in relation to the decisional aid. From a maximum score of 10, mean knowledge scores did not significantly differ between those who then received the intervention (4.1) or control (4.2) condition.
Skinner et al. [33] studied expectations for receiving a genetic counselling session in which family-specific recurrence risks were discussed in a small sample of MS patients. 43.5% reported having an ‘average’ understanding of MS aetiology, 17.8% reported a ‘greater than average’ and 38.7% reported a ‘less than average’ understanding.
Factors associated with MS knowledge
Studies have measured demographic or disease-related variables alongside MS knowledge to examine their association.
Age
Assessing correlates of MS knowledge, Giordano et al. [11] found MS knowledge scores were not associated with age (Odds Ratio (OR): 1.1; Confidence Interval (CI): 0.5–2.2; p = 0.27). Similarly, Heesen et al. [10] found MS knowledge was not associated with age (β = 0.03, p = 0.486). Generally, age has not been associated with MS knowledge.
Gender
Giordano et al. [11] studied the association between female gender and MSKQ scores. A positive correlation was identified between the two factors (OR: 2.2; CI: 1.0–4.6; p = 0.03). Abulaban et al. [9] found MSKQ scores were marginally higher in female patients. However, Heesen et al. [10] did not find a strong relationship between gender and MSKQ scores (β = 0.03, p = 0.442). Studies have yielded mixed results with regards to gender and MS knowledge.
Education
Giordano et al. [11] found MSKQ scores positively and significantly correlated with higher educational attainment (OR: 5.0; CI: 1.7–14.4; p = 0.001). Heesen et al. [10] also found higher levels of MS knowledge correlated significantly with higher levels of education (β = 0.26, p < 0.001). Further, Abulaban et al. [9] found higher MSKQ scores positively correlated with higher levels of educational attainment (p = 0.07). Conversely, Skinner et al. [33] found the percentage of correct knowledge scores did not differ according to educational level (p = 0.915). Apart from one study, positive relationships between higher educational level and MS knowledge have been identified.
Ethnicity
Giordano et al. [28] compared MSKQ scores between patients from 3 countries. MSKQ scores in Germany (n = 117; mean = 19.8; SD = 3.1), Italy (n = 53; mean = 18.3; SD = 3.6) and the Netherlands (n = 128; mean = 19.1; SD = 3.1) were similar. No further studies measured ethnicity as a correlate of MS knowledge.
Disease duration
Giordano et al. [11] found higher MSKQ scores significantly correlated with a shorter disease duration (p = 0.03). Conversely, Skinner et al. [33] found MS knowledge scores did not differ according to time since diagnosis (p = 0.31). Relying on a scattering of studies, results have been mixed in relation to disease duration.
DMDs
Bruce et al. [26] found higher MSKQ scores positively correlated with increased willingness to take DMDs (ρ = 0.28, p < 0.001). In relation to self-reported treatment adherence determination, Bruce et al. [27] reported a significant correlation with higher MS knowledge (r = 0.22, p = 0.002). Jarmolowicz et al. [29] reported lower level of price sensitivity to DMDs correlated with higher MS knowledge (r = -0.24, p < 0.01). Varied factors related to DMD use have been associated with higher MS knowledge, including willingness to take medication and self-reported medication adherence.
Disability
Heesen et al. [10] found MSKQ scores were not associated with self-reported disability (β = − 0.02, p = 0.595). No further studies measured disability as a correlate of MS knowledge.
Mood
Giordano et al. [11] found MS knowledge was not associated with anxiety (OR: 0.6; CI: 0.3–1.3; p = 0.16). Studies correlating mood with MS knowledge have been limited, whilst no studies measured the association with MS risk knowledge.
Cognition
In relation to cognition, Heesen et al. [10] found self-rated cognitive functioning was not significantly correlated with MSKQ scores (β = − 0.07, p = 0.073) or RIKN0 2.0 scores (β = − 0.07, p = 0.052). No further studies measured the association between mood and MS knowledge or MS risk knowledge.
MS risk knowledgeValidated measures
Seven studies used validated MS risk knowledge measures within survey designs or as baseline measures in intervention studies.
Giordano et al. [28] summarised patients’ risk knowledge scores on the RIKNO 2.0. From a possible score of 21, the mean RIKNO 2.0 score was 8.7 (SD = 3.5; n = 1153). MSKQ scores were significantly higher than RIKNO 2.0 scores (adjusted mean difference = 36.2; p < 0.01).
Alongside investigating MS patients’ perceived level of knowledge, information interests and decisional role preferences, Heesen et al. [15] developed the MSK to assess MS risk knowledge. From a maximum score of 19, the authors described patients having low risk knowledge, with a mean score of 6.4 (SD = 2.4) obtained.
Heesen et al. [16] developed the RIKNO 1.0 to assess MS risk knowledge. In a pilot study, a small group of patients received 4 sessions of an educational programme and completed the questionnaire. The programme entailed a 4-h educational session on MS diagnosis, prognosis and treatment. The mean baseline RIKNO 1.0 score was 9.8 (SD = 3.2).
In validating the RIKNO 2.0, Heesen et al. [10] obtained a mean RIKNO 2.0 score of 8.9 (SD = 3.6) from a large sample. The authors observed higher scores were generally obtained on the MSKQ.
Köpke et al. [34] compared the efficacy of an educational programme with a stress management control condition in promoting informed treatment decision making and patient autonomy. Risk knowledge was measured using the MSK at baseline and 2 weeks post-intervention. ‘Good risk knowledge’ was classed as attaining at least a score of 12 out of 19. At baseline, the mean MSK score was 10.6 (SD = 2.6) for those who then received the intervention and 9.4 (SD = 2.9) for those in the control condition.
Similarly, Köpke et al. [35] compared the effectiveness of a 6-h educational programme with standard information in promoting informed decision making. Adequate risk knowledge was defined as at least 9 correct responses out of 19 on the RIKNO 1.0. At baseline, the mean score was 6.1 (SD = 2.8) for those who then received the intervention and 6.51 (SD = 2.5) for those in the control condition.
In an RCT, Rahn et al. [36] compared the efficacy of a decision coaching programme on DMD benefits and risks with care as usual in a small group of patients with RRMS. From a maximum score of 19, mean baseline RIKNO 1.0 scores were 8.3 (SD = 3.4) for intervention group and 8.1 (SD = 3.1) for control group patients.
Unvalidated measures
Three studies used bespoke MS risk knowledge measures within survey or intervention studies. Bichuetti et al. [37] measured knowledge of risks associated with Natalizumab (NAT) in a small sample of Brazilian patients with RRMS. Patients considered MS a severe disease, and generally understood risks associated with NAT, with most patients considering risk of PML as ‘moderate to high’.
Heesen et al. [38] investigated patients’ understanding and acceptance of risks associated with NAT, including risk of PML. The authors reported on data from two trials (PERCEPT and CONSIDER). In the CONSIDER trial, data were collected from a subset of PERCEPT trial patients at baseline, 1 month and at 12 month follow-up regarding knowledge of NAT efficacy and side effects. 61.6% of patients were aware PML is unlikely in the first year of treatment and 64.6% could identify outcomes associated with having all three risk factors present. 51.5% underestimated the risk of PML following 2 years of therapy. 29.3% provided a correct response regarding degree of risk increase due to deficient immunosuppression.
In assessing MS patients’ knowledge of risks associated with taking Mitoxantrone (MITOX), Hofmann et al. [39] invited patients to complete a questionnaire before and after they received evidence-based information. At baseline, 40% of patients correctly selected the correct risk for leukaemia and 16% selected the correct risk for cardiotoxicity. 58% underestimated risks for leukaemia and 82% underestimated risks of cardiotoxicity.
Factors associated with MS risk knowledge
Alongside measuring MS risk knowledge, studies have measured associations between knowledge and demographic or disease-related variables.
Age
Heesen et al. [16] found younger age correlated with higher RIKNO 1.0 scores (β = - 0.22, p = 0.002) in patients who completed the PEDAPIP trial [34]. Similarly, Heesen et al. [15] found age negatively correlated with higher MSK scores (r = - 0.46, p < 0.001). However, in validating the RIKNO 2.0, Heesen et al. [10] found MS risk knowledge was not associated with age (β = − 0.06, p = 0.093). Similarly, Heesen et al. [38] found age did not predict knowledge of PML risk when commencing NAT in patients with RRMS. Hofmann et al. [39] found patients’ knowledge of risks associated with taking MITOX did not differ according to patients’ age. In summary, the association between age and knowledge has generally been inconsistent.
Gender
Heesen et al. [10] found RIKNO 2.0 scores were not associated with female gender (β = − 0.02, p = 0.558). Heesen et al. [38] found gender was not predictive of risk knowledge for developing PML when taking NAT. Further, Hofmann et al. [39] found gender was not associated with estimation of risks for developing leukaemia when taking MITOX. Relationships between gender and knowledge have been inconsistent between studies.
Education
Heesen et al. [16] found higher levels of educational attainment significantly correlated with higher MS risk knowledge (β = 0.21, p = 0.005). Heesen et al. [10] found higher levels of education (β = 0.3, p < 0.001) were positively and significantly associated with higher RIKNO 2.0 scores. Relationships between education and risk knowledge have been consistent.
Ethnicity
Giordano et al. [28] noted higher mean scores were obtained in Germany (n = 242; mean = 9.3; SD = 4.4) and Serbia (n = 107; mean = 11.7; SD = 3.6), whilst scores in Italy (n = 100; mean = 7.2; SD = 3.1), Spain (n = 363; mean = 6.3; SD = 3.5), Turkey (n = 203; mean = 6.6; SD = 2.7) and the Netherlands (n = 138; mean = 9; SD = 2.7) were similar.
MS subtype
In evaluating disease course as a determinant of MS risk knowledge, Heesen et al. [15] found mean MSK scores were highest in patients diagnosed within the previous year (mean = 8.3; SD = 3), followed by RRMS patients (mean = 7.2; SD = 2.6) and PPMS patients (mean = 5.2; SD = 2.6) (F(2,166) = 15.9, p = 0.001). Heesen et al. [16] identified a relapsing–remitting course was significantly associated with higher RIKNO 1.0 scores (β = 0.22, p = 0.002). A limited number of studies correlated MS subtype with MS risk knowledge, whilst no studies measured the association with MS knowledge.
Disease duration
Heesen et al. [38] found time since diagnosis was not predictive of risk knowledge for developing PML when receiving NAT. In evaluating how responses on the MSK differed according to years since diagnosis, Heesen et al. [15] noted recently diagnosed patients obtained the highest MSK scores. Although few studies have measured an association between disease duration and risk knowledge, studies have identified mixed relationships between these variables.
DMDs
Heesen et al. [16] identified an autonomous preference for making treatment decisions negatively correlated with higher RIKNO 1.0 scores (β = - 0.19, p = 0.01). Heesen et al. [38] found length of NAT treatment was not predictive of risk stratification knowledge for developing PML. Heesen et al. [15] found patients in receipt of interferon therapies provided more correct calculations of the therapeutic effects of their therapies (mean = 7.4; SD = 2.7) than patients not in receipt of these therapies (mean = 6.2, SD = 2.8) (F(1,167) = 9.5, p = 0.002). Hofmann et al. [39] found MS risk knowledge did not differ between patients taking DMDs over the past 5 years or earlier (p = 0.31). Studies associating a range of factors relating to DMDs and MS risk knowledge have produced mixed results.
Disability
Heesen et al. [10] found RIKNO 2.0 scores were not associated with PDDS scores (β = − 0.07, p = 0.049). Further, Heesen et al. [38] found baseline EDSS scores were predictive of risk stratification knowledge for developing PML when taking NAT (β = - 0.25, p = 0.033).
Summary
Generally suboptimal levels of MS knowledge and MS risk knowledge were identified across studies. Because some studies used unvalidated measures, it is difficult to compare studies. Significant positive relationships have been demonstrated between higher levels of educational attainment and greater levels of knowledge, with relationships with MS risk knowledge being consistent. Associations between greater MS knowledge and varied aspects of DMD use were observed, while relationships between both knowledge domains and other demographic and disease-related variables were inconsistent.








留言 (0)